63 yr old hypertension, medicine to prescribe
Reading File
Finding Sources
Searching PubMed
"hypertension" AND "elderly" AND "antihypertensive"
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have sufficient information to provide a thorough, evidence-based answer. Let me also note that the question lacks specifics about comorbidities, so I'll present a comprehensive framework.
Antihypertensive Therapy for a 63-Year-Old Patient
Important note: The optimal choice of drug depends heavily on comorbidities (diabetes, CKD, heart failure, IHD, history of stroke, etc.) and ethnicity. The following is a framework based on current guidelines - always tailor to the individual patient.
Blood Pressure Target
| Guideline | Goal (age >60 yr) |
|---|---|
| JNC 8 | <150/90 mmHg (≥60 yr) |
| ACC/AHA 2017 | <130/80 mmHg (most patients) |
| ESC/ESH | <140/90 mmHg; consider <130/80 if tolerated |
At age 63, the ACC/AHA target of <130/80 mmHg is appropriate for most patients, provided this is tolerated without orthostatic hypotension (a concern in the elderly).
First-Line Drug Classes (Uncomplicated Hypertension)
The four major first-line classes are:
| Drug Class | Examples | Notes |
|---|---|---|
| Thiazide / Thiazide-like diuretics | Hydrochlorothiazide 12.5-25 mg OD; Chlorthalidone 12.5-25 mg OD (preferred - longer acting, more potent) | Monitor electrolytes (K⁺, Na⁺, uric acid) |
| ACE inhibitors | Enalapril 5-20 mg OD/BD; Ramipril 2.5-10 mg OD; Perindopril 4-8 mg OD | Avoid in bilateral renal artery stenosis; causes cough (~10%) |
| ARBs (alternative to ACEi) | Losartan 50-100 mg OD; Telmisartan 40-80 mg OD; Olmesartan 20-40 mg OD | Use if ACEi-intolerant due to cough; no angioedema risk |
| Calcium Channel Blockers (CCB) | Amlodipine 5-10 mg OD (dihydropyridine - preferred); Nifedipine SR | Preferred in Black patients and elderly with isolated systolic HTN; ankle edema is common SE |
Do NOT combine ACE inhibitor + ARB (dual RAAS blockade is contraindicated).
Preferred Combinations (if monotherapy insufficient)
Most patients (75%) will need 2+ drugs. The strongest evidence supports:
ACE inhibitor + CCB (amlodipine) - based on the ACCOMPLISH trial (superior to ACEi + thiazide in reducing CV events)
Acceptable alternatives:
- ACE inhibitor + thiazide diuretic
- ARB + CCB
- ARB + thiazide diuretic
Drug Selection by Comorbidity
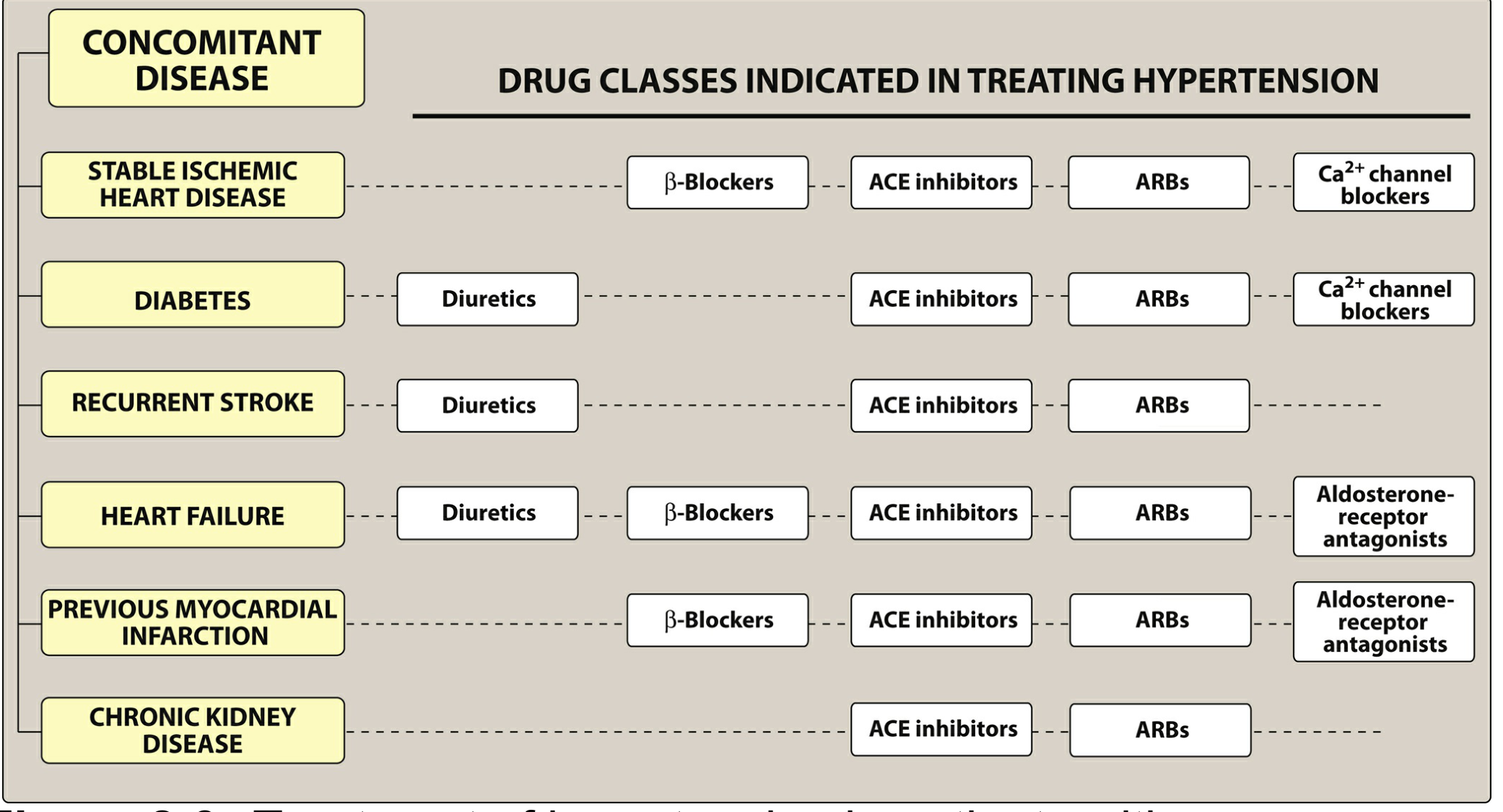
| Comorbidity | Preferred Agent(s) |
|---|---|
| Diabetes | ACEi or ARB (renoprotective) + CCB or thiazide |
| CKD / Proteinuria | ACEi or ARB (first choice) |
| Heart failure (HFrEF) | ACEi/ARB + beta-blocker + diuretic + aldosterone antagonist |
| Stable IHD / Post-MI | Beta-blocker + ACEi/ARB + CCB |
| Recurrent stroke prevention | ACEi + thiazide diuretic |
| Black patients | CCB or thiazide diuretic (ACEi less effective as monotherapy) |
| Isolated systolic HTN (elderly) | CCB (amlodipine) or thiazide-like diuretic |
Drugs to Generally Avoid in Elderly
- Beta-blockers - not recommended as monotherapy in uncomplicated HTN (inferior outcomes in trials); also cause fatigue, sexual dysfunction, mask hypoglycemia
- Alpha-blockers (e.g., doxazosin) - increased risk of orthostatic hypotension and falls in the elderly
- Central agents (methyldopa, clonidine) - CNS side effects in elderly
- Non-dihydropyridine CCBs (verapamil, diltiazem) - avoid in HFrEF
Practical Starting Regimen (Uncomplicated 63-Year-Old)
Option A - Monotherapy:
- Amlodipine 5 mg once daily (titrate to 10 mg if needed)
- OR Ramipril 2.5-5 mg once daily
- OR Chlorthalidone 12.5-25 mg once daily
Option B - If BP is >20/10 mmHg above target, start combination immediately:
- Perindopril 4 mg + Amlodipine 5 mg (fixed-dose combination available: Coveram, Prestalia)
- Reassess in 4 weeks; titrate doses as needed
Lifestyle Modifications (Always Combined with Pharmacotherapy)
- Sodium restriction (<2 g/day)
- DASH diet
- Weight loss if overweight
- Regular aerobic exercise (150 min/week)
- Limit alcohol
- Smoking cessation
Sources:
- Lippincott Illustrated Reviews: Pharmacology, Chapter 8 (Antihypertensives)
- Textbook of Family Medicine, 9e (Hypertension management)
- Recent Cochrane review: Pharmacotherapy for hypertension in adults ≥60 years (PMID 41065416) - confirms treatment reduces CV events in this age group
- 2025 systematic review of hypertension guidelines (BMC Cardiovasc Disord, 2025)
Diabetes patient with respiratory distress Bp -150/90 Spo2-90 Next step
Reading File
Finding Sources
Finding Sources
Finding Sources
This is a shared conversation. Sign in to Orris to start your own chat.