Tau protiens
Reading File
Finding Sources
Searching the Web
tau protein structure function tauopathies neuroscience 2025
Finding Sources
Searching PubMed
"tau protein" tauopathy neurodegeneration
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Here is a thorough overview of tau proteins, drawing from multiple authoritative medical textbooks:
Tau Proteins: A Complete Overview
1. What is Tau?
Tau is a microtubule-associated protein (MAP) encoded by the MAPT gene (Microtubule-Associated Protein Tau), located on chromosome 17. It is expressed abundantly in neurons of the brain, primarily in axons. Its core physiological role is to promote the assembly and stability of microtubules, which form the internal scaffolding of neurons and serve as tracks for axonal transport.
- In axons, tau binds along the length of microtubules, compressing and stabilizing them
- In dendrites, the analogous function is performed by MAP2
- Tau also regulates axonal transport via motor proteins (dynein and kinesin)
- Additional roles include synaptic plasticity, nuclear DNA/chromatin protection from oxidative stress, and intracellular signaling
"Tau is a microtubule-associated protein expressed abundantly in neurons of the brain. Hyperphosphorylated forms of tau compose the neurofibrillary tangles." - Thompson & Thompson Genetics in Medicine
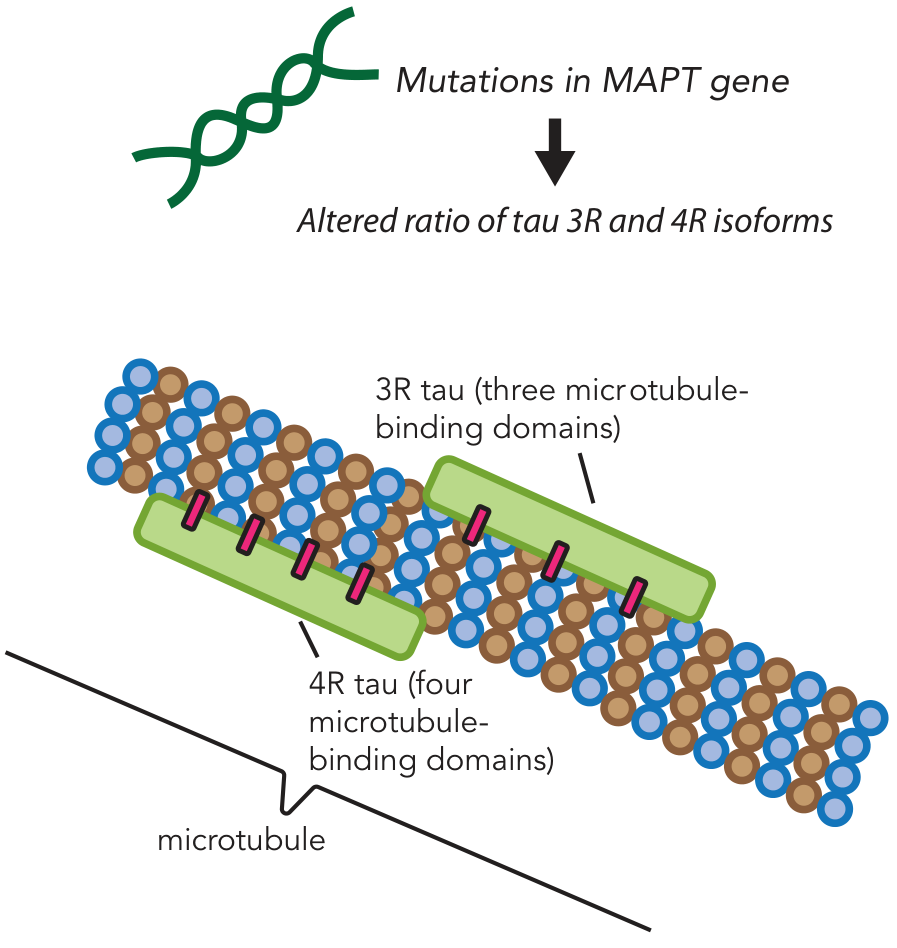
2. Structure and Isoforms
Tau exists as multiple isoforms produced by alternative mRNA splicing of the MAPT gene. The most clinically important distinction is between:
| Isoform | Microtubule-Binding Domains | Notes |
|---|---|---|
| 3R tau | 3 repeats | Equal with 4R in healthy adult brain |
| 4R tau | 4 repeats | Slightly stronger microtubule binding |
The balance between 3R and 4R isoforms is critical for normal neuronal function. Disturbances in this ratio provoke tau aggregation and disease.
3. Phosphorylation - The Key Regulatory Switch
Tau's binding to microtubules is regulated by phosphorylation. There is an inverse relationship between phosphorylation and microtubule binding:
- Normal tau: low phosphorylation → stable microtubule binding
- Hyperphosphorylated tau: detaches from microtubules → aggregates → forms neurofibrillary tangles (NFTs)
- Key kinases involved include GSK-3β (glycogen synthase kinase-3 beta) and CDK5
When tau hyperphosphorylates, it can no longer perform its stabilizing function. The resulting loss of microtubule integrity disrupts axonal transport, causing axons to wither and synaptic connections to be lost.
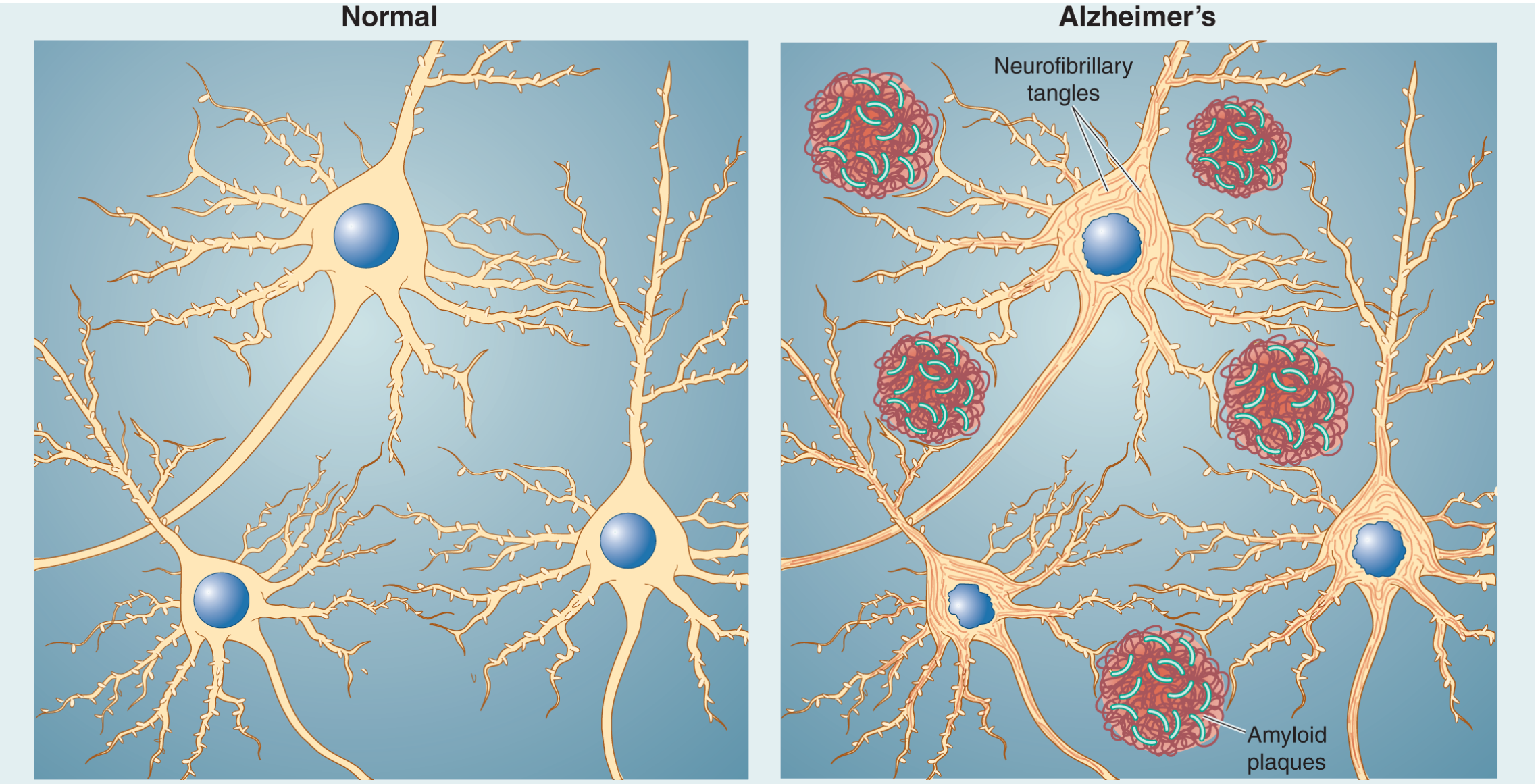
4. Neurofibrillary Tangles (NFTs)
NFTs are the pathological hallmark of tau disease:
- Structurally, they consist of paired helical filaments (PHFs) - two tau strands braided together like rope
- They form inside neurons (intracellular), in contrast to amyloid plaques which are extracellular
- Under silver staining (Bielschowsky method) or tau immunohistochemistry, they appear as dark inclusions within neuronal cytoplasm
- Neurons with heavy tangle burden eventually die, leaving only the tangle as a "tombstone"
"The severity of the dementia in Alzheimer's disease is well correlated with the number and distribution of neurofibrillary tangles, the 'tombstones' of dead and dying neurons." - Neuroscience: Exploring the Brain, 5th Ed.
5. Tauopathies - Diseases Caused by Tau Pathology
Any disease characterized by abnormal tau accumulation is called a tauopathy. They are classified by the predominant isoform involved:
Primary Tauopathies (tau alone, no amyloid)
| Disease | Tau Type | Key Features |
|---|---|---|
| Pick's Disease | 3R tau | Knife-edge frontal/temporal atrophy; Pick bodies (round tau inclusions) in neurons |
| Progressive Supranuclear Palsy (PSP) | 4R tau | Vertical gaze palsy, falls, parkinsonism |
| Corticobasal Degeneration (CBD) | 4R tau | Asymmetric limb apraxia, alien limb |
| FTLD-tau | 3R or 4R | Frontotemporal lobar degeneration due to MAPT mutations |
| Chronic Traumatic Encephalopathy (CTE) | 3R+4R | Head trauma history; perivascular tau deposits |
Secondary Tauopathies (tau + other pathology)
| Disease | Notes |
|---|---|
| Alzheimer's disease (AD) | NFTs + amyloid plaques; tau burden mirrors dementia severity |
| Down Syndrome | NFTs appear early; similar to AD |
| Dementia pugilistica | Punch-drunk syndrome; also has NFTs |
MAPT Gene Mutations in FTLD-tau
Two types of MAPT mutations are described (Robbins & Kumar):
- Missense point mutations - affect tau phosphorylation, tipping balance toward aggregation
- Splicing mutations (often intronic) - alter 3R:4R ratio, also promoting aggregation
There is both a loss-of-function component (tau depleted from microtubules) and a toxic gain-of-function component (aberrant aggregated tau).
6. Tau in Alzheimer's Disease
In AD, tau pathology follows a predictable anatomical progression (Braak staging):
- Early stages: NFTs in entorhinal cortex and hippocampus → episodic memory loss (mild cognitive impairment)
- Intermediate: Spreads to association cortices of frontal, parietal, temporal lobes
- Late/severe: NFTs reach occipital lobes and primary motor/sensory cortices
- NFTs appear in the medial temporal lobe and brainstem even in cognitively normal people in their 40s
- Tangle spread is thought to occur via transsynaptic propagation (prion-like spread)
- Unlike amyloid plaques (which plateau early), NFT burden closely mirrors dementia severity
The amyloid cascade hypothesis proposes: Aβ accumulation → triggers tau hyperphosphorylation → NFT formation → synaptic failure → neuronal death.
7. Tau as a Biomarker
CSF tau is one of the most validated biomarkers in neurology:
| Biomarker | What it measures | In AD |
|---|---|---|
| T-tau (total tau) | Overall neuronal/axonal damage | Elevated |
| P-tau181 (phospho-tau) | Specific AD-related phosphorylation | Elevated (high specificity for AD) |
| CSF Aβ42/tau ratio | Combined amyloid + tau | Reduced ratio = AD pattern |
The combination of low CSF Aβ42 + elevated CSF tau has ~85% sensitivity and ~86% specificity for AD diagnosis (Bradley & Daroff's Neurology).
Harrison's Principles of Internal Medicine (2025) classifies plasma Aβ and p-Tau as "core 1 biomarkers" - necessary and sufficient for AD diagnosis regardless of symptoms. Tau PET imaging is a "core 2 biomarker" for further staging.
8. Therapeutic Targets
Current research targets include (Stahl's Psychopharmacology):
| Strategy | Approach |
|---|---|
| Anti-tau antibodies | Active immunization against pathological tau |
| Tau aggregation inhibitors | Block filament formation |
| Tau phosphorylation inhibitors | Inhibit GSK-3β and other kinases |
| Microtubule stabilizers | Compensate for tau loss-of-function |
Summary
Tau is a neuronal scaffolding protein that keeps axonal microtubules stable. When it becomes hyperphosphorylated, it detaches, aggregates into paired helical filaments, and forms neurofibrillary tangles that kill neurons. The disease burden from tau - in Alzheimer's, FTD, PSP, Pick's, and other tauopathies - is one of the major unsolved challenges in neurodegeneration research. CSF and plasma tau biomarkers are now central to clinical diagnosis of these conditions.
Sources: Stahl's Essential Psychopharmacology | Thompson & Thompson Genetics in Medicine, 9th Ed. | Robbins, Cotran & Kumar Pathologic Basis of Disease | Neuroscience: Exploring the Brain, 5th Ed. | Goldman-Cecil Medicine | Bradley & Daroff's Neurology in Clinical Practice | Harrison's Principles of Internal Medicine 22E (2025)
This is a shared conversation. Sign in to Orris to start your own chat.