Diabetic nephropathy
Reading File
Finding Sources
Finding Sources
Searching PubMed
"diabetic nephropathy" AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full, detailed response.
Diabetic Nephropathy (Diabetic Kidney Disease)
Definition and Epidemiology
Diabetic nephropathy (DN) - also called diabetic kidney disease (DKD) - is the leading cause of chronic kidney disease (CKD) and end-stage kidney disease (ESKD) requiring renal replacement therapy in Western societies and increasingly in Asia. It affects approximately 30-40% of patients with type 2 diabetes and a similar proportion with type 1 diabetes. In Japan, DN surpassed glomerulonephritis as the #1 cause of dialysis since 1997; in the US, it accounts for the majority of new ESKD cases annually. Risk is disproportionately elevated in Black, Native American, and Hispanic individuals.
- Harrison's Principles of Internal Medicine, 22E, p. 3267-3268
- Brenner and Rector's The Kidney, p. 3381
Pathogenesis
Chronic hyperglycemia is the central driver, acting through multiple converging mechanisms:
| Mechanism | Details |
|---|---|
| Hemodynamic | Glomerular hyperfiltration and hyperperfusion; increased glomerular capillary pressure; early GFR elevation |
| Soluble factors | AGEs (advanced glycation end-products), angiotensin II, endothelin, TGF-β, growth factors |
| Structural/ECM changes | GBM thickening, mesangial expansion, increased extracellular matrix, fibrosis |
| Tubular dysfunction | Tubulointerstitial damage, fibrosis, tubular hypertrophy |
| Epigenetic | Chromatin remodeling, metabolic memory |
| RAAS activation | Intrarenal angiotensin II drives fibrosis and podocyte injury |
| Genetic factors | ACE gene I/D polymorphism (D allele = high ACE activity = worse nephropathy risk), IL-6, IL-10, ICAM1 polymorphisms |
- Harrison's, p. 3268
- Brenner and Rector's The Kidney, p. 3381
Pathology
The renal lesions span three broad categories:
1. Glomerular Lesions (most important)
a) Glomerular basement membrane (GBM) thickening
- Detectable by electron microscopy within a few years of DM onset, often before any functional change
- Thickening occurs along the entire capillary length
b) Diffuse mesangial sclerosis
- Increase in mesangial matrix + mesangial cell proliferation + BM thickening
- Present in most patients with >10 years of disease
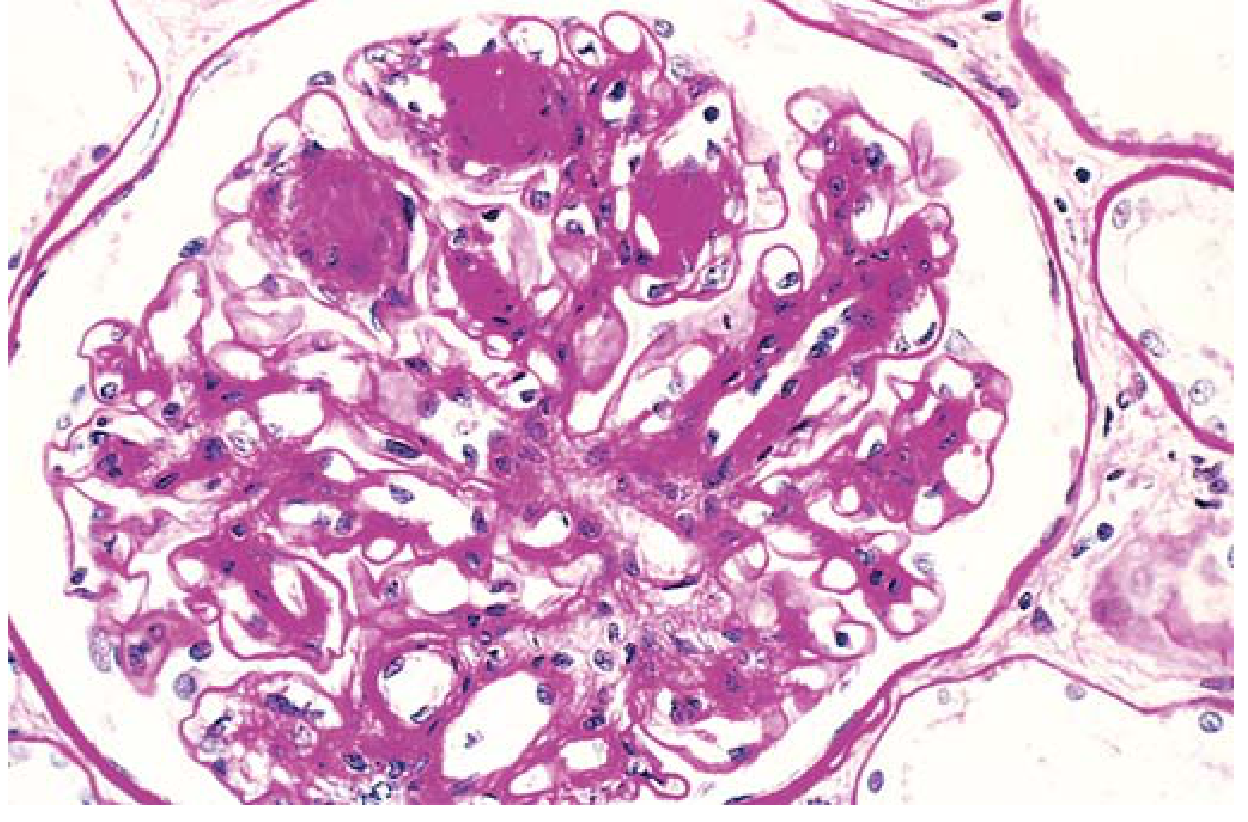
c) Nodular glomerulosclerosis (Kimmelstiel-Wilson lesion)
- Ball-like laminated matrix deposits in the glomerular periphery
- Seen in ~15-30% of long-term diabetics
- Virtually pathognomonic of diabetes (distinguishes it from diffuse form)
- Major contributor to renal dysfunction; when severe, causes nephrotic syndrome
2. Vascular Lesions
- Hyaline arteriolosclerosis affects both afferent AND efferent arterioles - efferent involvement is virtually unique to diabetes
- Renal atherosclerosis as part of systemic macrovascular disease
- Vascular compromise → ischemia → diffuse cortical scarring (nephrosclerosis) → finely granular cortical surface
3. Tubular and Interstitial Lesions
-
Thickening of tubular basement membranes
-
Pyelonephritis (both acute and chronic) - more severe in diabetics
-
Necrotizing papillitis (papillary necrosis) - much more prevalent in diabetics
-
Robbins & Kumar Basic Pathology, p. 751
Natural History / Stages
The classic sequence was first defined in type 1 DM but applies similarly in type 2:
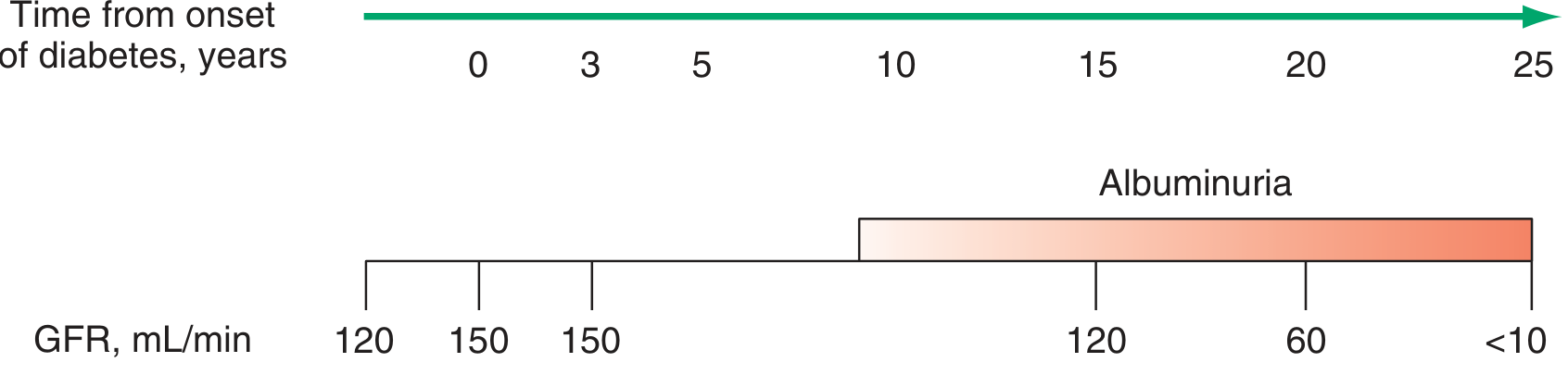
| Stage | Timing | Findings |
|---|---|---|
| Hyperfiltration | Onset | GFR elevated (120-150 mL/min), renal hypertrophy, no albuminuria |
| Silent/Structural | Years 0-5 | GBM thickening, mesangial expansion; GFR normalizes; normoalbuminuria |
| Incipient nephropathy | ~5-10 years | Microalbuminuria (UACR 30-299 mg/g); early GFR may still be normal or elevated |
| Overt nephropathy | ~10-15 years | Macroalbuminuria (UACR ≥300 mg/g); GFR declining; HTN common |
| ESKD | >15-20 years | GFR <10-15 mL/min; dialysis or transplant required |
- Once marked albuminuria and GFR reduction occur, pathologic changes are likely irreversible
- Harrison's, p. 3268
Screening and Diagnosis
- Screen with both UACR (spot urine) and eGFR - some patients have GFR decline without albuminuria
- Type 1 DM: Screen 5 years after diagnosis, then annually
- Type 2 DM: Screen at time of diagnosis, then annually
- ADA defines albuminuria as UACR >30 mg/g (persistently elevated on 2-3 occasions over 3-6 months)
- Moderate: 30-299 mg/g creatinine
- Severely elevated: ≥300 mg/g creatinine
- Confirm elevated UACR on 2-3 occasions (rule out: exercise, fever, UTI, CHF, hyperglycemia, hypertension)
- Routine urinalysis does not detect low-level albuminuria
Concurrent findings to monitor:
-
Type IV RTA (hyporeninemic hypoaldosteronism) → hyperkalemia + acidemia - exacerbated by ACEi/ARBs/MRAs
-
Radiocontrast nephrotoxicity risk is elevated; ensure adequate hydration pre/post procedure
-
Harrison's, p. 3268-3269
Treatment
1. Glycemic Control
- Reduces rate of albuminuria onset and progression in both T1D and T2D
- Less effective once moderate albuminuria is established
- Glucose-lowering adjustments by eGFR:
- Sulfonylureas and metformin: contraindicated in advanced CKD
- SGLT2 inhibitors: not effective with eGFR <20 mL/min/1.73 m²
- GLP-1 agonists and DPP-4 inhibitors: may require dose adjustment
- 10 years of normoglycemia (via pancreas transplantation) can reverse mesangial lesions
2. Blood Pressure Control
- Target: <130/80 mmHg (possibly lower if high ASCVD or CKD progression risk)
- If BP >150/90 mmHg: start with two antihypertensive agents
- Lifestyle: weight loss, sodium restriction, DASH-style diet, exercise, smoking cessation
3. RAAS Blockade (cornerstone)
- ACEi or ARB: first-line for any patient with DM + albuminuria or CKD
- Reduces albuminuria and slows GFR decline in T1D and T2D
- Both classes considered equivalent
- Use ARB as alternative if ACEi causes cough/angioedema
- Titrate to maximum tolerated dose
- A rise in serum creatinine up to 30% is acceptable
- Dose goal in overt proteinuria (UACR >300 mg/g): reduce UACR by ≥30%
- Monitor serum K⁺ closely
- Do not combine ACEi + ARB (no added benefit, increased harm)
4. SGLT-2 Inhibitors (transformative modern addition)
- Recommended with eGFR >20 mL/min/1.73 m² in type 2 DM + CKD (with any level of albuminuria), added to ACEi/ARB
- Reduce CKD progression and cardiovascular events
- Mechanism: reduce intraglomerular pressure, reduce glucotoxicity, reduce tubular workload
- Caution in T1DM/insulin-deficient T2DM: risk of euglycemic DKA
5. Finerenone (Nonsteroidal MRA)
- Reduces cardiovascular risk in type 2 DM + CKD
- More selective and less hyperkalemia risk than spironolactone/eplerenone
- Monitor K⁺ closely; avoid dual MRA + high-dose RAASi
6. GLP-1 Receptor Agonists
- Semaglutide specifically improves kidney outcomes and reduces cardiovascular death in type 2 DM + CKD
- Also reduces body weight and blood pressure
7. Lipid Management
- ASCVD is the leading cause of death in patients with DN - treat dyslipidemia aggressively (statins)
8. Dietary Protein Restriction
- ADA recommends: 0.8 g/kg/day protein in patients with diabetic kidney disease
9. Nephrology Referral Indications
- eGFR <30 mL/min/1.73 m²
- Albuminuria >300 mg/g creatinine
- Atypical features: hematuria, rapidly declining renal function
10. Renal Replacement Therapy
-
Preemptive (pre-dialysis) kidney transplantation from living donor should be considered approaching ESKD
-
For T1DM or insulin-deficient T2DM: simultaneous pancreas-kidney (SPK) transplant from deceased donor is an option
-
SPK prevents recurrence of diabetic nephropathy in the allograft
-
Hemodialysis in DM: more complications (hypotension from autonomic neuropathy, difficult vascular access, accelerated ASCVD)
-
Harrison's 22E, p. 3268-3270
Summary Table: Key Drug Therapies
| Agent | Indication | Key Benefit | Limitation |
|---|---|---|---|
| ACEi / ARB | Albuminuria ± CKD | Reduces proteinuria, slows GFR decline | Hyperkalemia, ↑Cr (up to 30% OK) |
| SGLT2 inhibitor | T2DM + CKD (eGFR >20) | Cardio-renal protection | Euglycemic DKA in T1D/insulin-deficient |
| Finerenone (MRA) | T2DM + CKD | CV risk reduction | Hyperkalemia |
| Semaglutide (GLP-1) | T2DM + CKD | Kidney + CV outcomes | Nausea, GI side effects |
| Statin | All DN patients | Reduces CV mortality | - |
Recent Evidence Update
A 2026 network meta-analysis (PMID: 41147324) confirms that among novel antidiabetic agents in T2DM + CKD, SGLT2 inhibitors show the most favorable renal outcome profile, consistent with current guidelines. A 2024 Cochrane review (PMID: 39171639) evaluated education programs for patients with DKD and diabetes, highlighting the importance of patient-centered self-management alongside pharmacotherapy.
Sources:
- Harrison's Principles of Internal Medicine, 22E (2025) - Chap. 417
- Robbins & Kumar Basic Pathology - Chap. 18
- Brenner and Rector's The Kidney - Chap. 80 and 6
- Goldman-Cecil Medicine - Chap. 109
Symptoms
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive, stage-by-stage symptom data from multiple authoritative sources. Here is the full answer:
Symptoms of Diabetic Nephropathy
The defining feature of diabetic nephropathy is that it is largely asymptomatic for years to decades. Symptoms emerge only as the disease advances through well-defined stages. This is precisely why annual screening (UACR + eGFR) is mandatory - waiting for symptoms means the disease is already advanced.
Stage-by-Stage Symptoms
Stage I - Hyperfiltration (onset)
- No symptoms
- GFR elevated (>150 mL/min), kidneys enlarge
- Blood pressure: normal (in T1DM); may already be elevated in 10-25% of T2DM patients
- Transient microalbuminuria may appear under stress (exercise, illness, poor glycemic control) but disappears at rest
- Kidney enlargement detectable on imaging but not clinically apparent
Stage II - Silent/Structural (years 0-5)
- Completely asymptomatic
- GFR ~150 mL/min (still elevated or normalizing)
- Normal albumin excretion (<30 mg/day) on standard testing
- Structural damage (GBM thickening, mesangial expansion) is already occurring at the microscopic level
- Blood pressure: normal
Stage III - Incipient Nephropathy / Microalbuminuria (~5-10 years)
- Still largely asymptomatic - detected only by laboratory screening
- Fixed microalbuminuria (30-300 mg/day; UACR 30-299 mg/g)
- GFR ~125 mL/min (still relatively preserved)
- Blood pressure begins to rise - often the first detectable clinical sign in T1DM
- In T2DM, pre-existing hypertension becomes harder to control
- Commonly associated with other microvascular signs: proliferative retinopathy, peripheral neuropathy - their co-presence supports the diagnosis
- Microalbuminuria is a risk marker for cardiovascular disease even at this stage
Stage IV - Overt Nephropathy (~10-15 years)
Symptoms now become clinically apparent:
| Symptom | Mechanism |
|---|---|
| Foamy / frothy urine | Heavy proteinuria (>300 mg/day; may reach nephrotic range >3.5 g/day) |
| Edema - periorbital (morning), ankle, pedal, facial | Hypoalbuminemia → reduced oncotic pressure → fluid shift to interstitium |
| Hypertension | Established; often severe and difficult to control |
| Fatigue / malaise | Anemia of CKD (reduced erythropoietin), fluid overload |
| Reduced urine output | As GFR falls below 60-100 mL/min |
| Weight gain | Fluid retention / edema |
| Dyslipidemia symptoms | Xanthelasma, xanthomas (nephrotic-range proteinuria drives hyperlipidemia) |
- A subset of T2DM patients develops progressive CKD without nephrotic-range proteinuria - an atypical presentation
Stage V - Uremia / ESKD (>15-20 years)
Terminal symptoms of kidney failure:
| System | Symptoms |
|---|---|
| GI | Nausea, vomiting, anorexia, metallic taste, hiccups |
| Neurological | Confusion, encephalopathy, asterixis (flapping tremor), peripheral neuropathy (worsened) |
| Skin | Pruritus (severe, generalized), uremic frost (urea crystals on skin - late sign), pallor from anemia |
| Cardiovascular | Dyspnea (fluid overload, pericarditis), pericardial friction rub, HTN crisis |
| Hematological | Pallor, easy bruising (uremic platelet dysfunction), severe anemia |
| Musculoskeletal | Bone pain (renal osteodystrophy), muscle cramps, restless legs |
| Reproductive | Amenorrhea, impotence |
| General | Extreme fatigue, weight loss, weakness |
Associated / Concurrent Symptoms (all stages)
Because diabetic nephropathy is a microvascular complication, it rarely occurs in isolation. Patients typically also present with:
- Diabetic retinopathy - visual blurring, floaters, reduced vision (virtually always present with overt nephropathy; its absence should prompt reconsideration of the diagnosis)
- Peripheral neuropathy - numbness, tingling, burning pain in feet ("glove-and-stocking" distribution)
- Autonomic neuropathy - postural hypotension, gastroparesis (bloating, nausea), erectile dysfunction, neurogenic bladder
- Recurrent UTIs / pyelonephritis - flank pain, dysuria, fever (diabetics are more susceptible, and papillary necrosis can occur - presenting as hematuria + colicky pain)
- Hyperkalemia - muscle weakness, palpitations (from Type IV RTA / hyporeninemic hypoaldosteronism, worsened by ACEi/ARBs)
Key Clinical Rule
Diabetic nephropathy = "a disease found on a test, not from a complaint."
The absence of retinopathy in a diabetic patient with proteinuria/CKD should raise suspicion for a non-diabetic cause of kidney disease (e.g., IgA nephropathy, FSGS), because DN almost invariably coexists with retinopathy in T1DM and is strongly associated in T2DM.
Sources: Goldman-Cecil Medicine, Chap. 109 | Tietz Textbook of Laboratory Medicine, 7th Ed., Table 49.11 | Harrison's Principles of Internal Medicine, 22E, Chap. 417
This is a shared conversation. Sign in to Orris to start your own chat.