Hydralazine moa in anti hypertensive
Reading File
Finding Sources
Searching PubMed
hydralazine mechanism action vasodilation
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Here is a thorough breakdown of hydralazine's mechanism of action as an antihypertensive:
Hydralazine - Mechanism of Action
Primary Mechanism: Direct Arteriolar Vasodilation
Hydralazine is a direct-acting vasodilator that selectively relaxes arteriolar smooth muscle (resistance vessels), with little to no effect on venous capacitance vessels.
The exact molecular mechanism is not fully understood, but two key pathways are established:
1. K-ATP Channel Activation
- Hydralazine activates ATP-sensitive potassium (K-ATP) channels in vascular smooth muscle
- This leads to hyperpolarization of the smooth muscle cell membrane
- Hyperpolarization inhibits voltage-gated calcium channels, reducing Ca²+ influx
- The net result is decreased intracellular Ca²+ → smooth muscle relaxation → vasodilation
- This effect is seen predominantly in coronary, cerebral, splanchnic, and renal vascular beds
(Barash's Clinical Anesthesia, p. 1000)
2. Antioxidant / Nitric Oxide (NO) Preservation
- Hydralazine has antioxidant properties - it inhibits reactive oxygen species (ROS) and oxidases
- By blocking ROS production, hydralazine prevents the breakdown of endogenous NO (and exogenous NO from drugs like isosorbide dinitrate)
- Enhanced NO availability activates soluble guanylate cyclase (sGC) → increased cGMP → activation of protein kinase G (PKG) → vasodilation
- This is why hydralazine is often combined with isosorbide dinitrate: isosorbide provides the NO, hydralazine prevents its oxidative degradation
(Lippincott Pharmacology; Fuster's The Heart, 15th Ed.)
Hemodynamic Effects
| Effect | Result |
|---|---|
| Arteriolar dilation | ↓ Systemic vascular resistance (SVR) |
| ↓ Afterload | ↑ Cardiac output |
| No venous dilation | Preload (LV) relatively preserved |
| Baroreceptor activation | Reflex tachycardia |
| ↓ Renal vascular resistance | Maintained/increased renal blood flow |
Compensatory/Reflex Responses (Important!)
Because hydralazine drops blood pressure via peripheral vasodilation, the body triggers three compensatory responses:
- Reflex tachycardia - baroreceptor-mediated; the magnitude is often greater than expected and may partly reflect a direct CNS effect on cardiovascular regulation
- Fluid/sodium retention - activation of the renin-angiotensin-aldosterone system (RAAS) due to reduced renal perfusion pressure
- Increased cardiac output - from the tachycardia + reduced afterload
These compensatory responses are why hydralazine is rarely used as monotherapy - it is almost always combined with a beta-blocker (to blunt tachycardia) and a diuretic (to counteract sodium retention).
Diagram - Hydralazine's NO Preservation Role
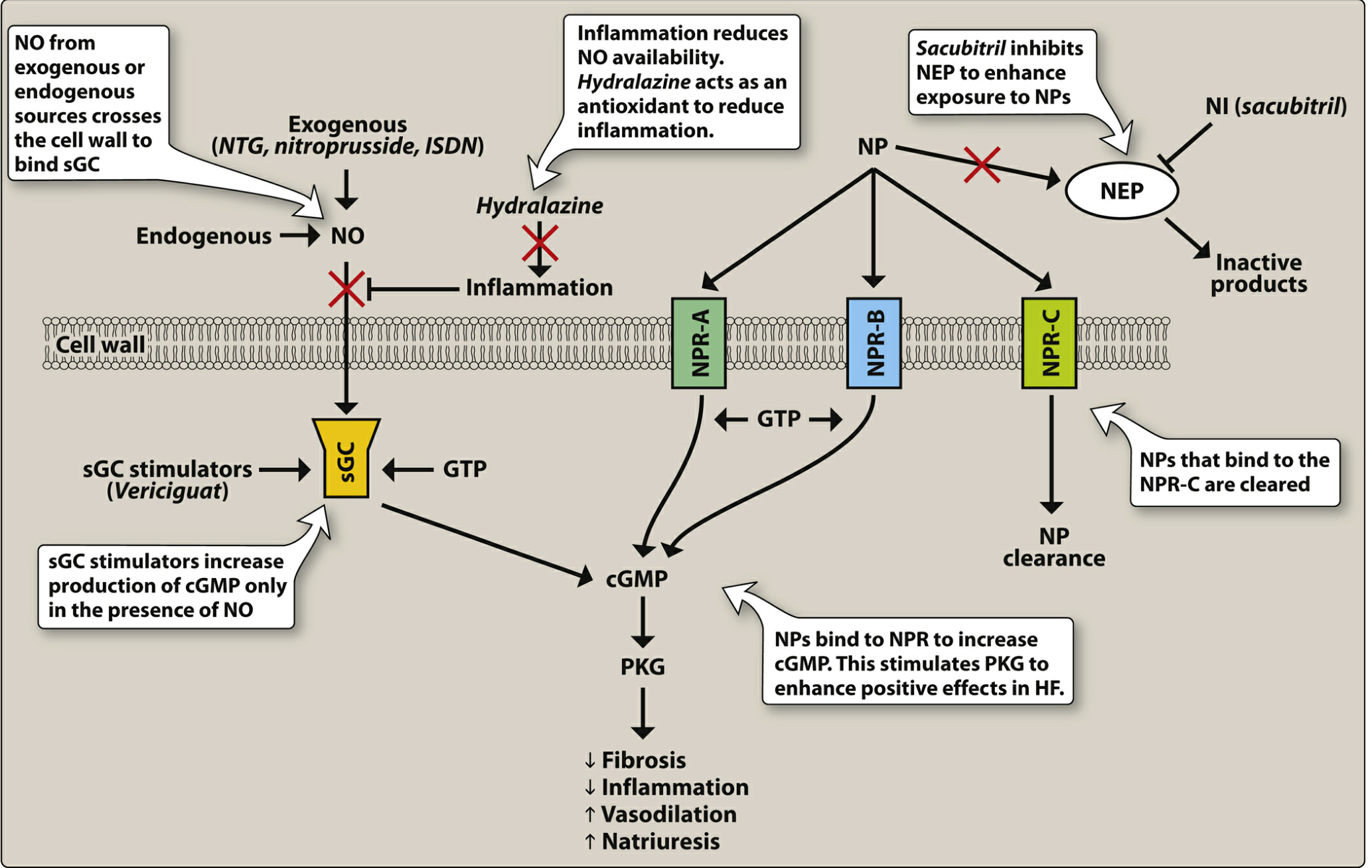
Hydralazine blocks inflammation-mediated NO breakdown, preserving the NO → sGC → cGMP → PKG → vasodilation cascade (Lippincott Illustrated Reviews: Pharmacology)
Summary of MOA in One Sentence
Hydralazine lowers blood pressure by directly relaxing arteriolar smooth muscle via K-ATP channel activation (reducing intracellular Ca²+) and antioxidant-mediated NO preservation (enhancing cGMP-mediated vasodilation), selectively reducing afterload with a compensatory reflex tachycardia and fluid retention that requires co-administration of a beta-blocker and diuretic.
Clinical Uses Tied to MOA
- Hypertensive urgency (IV/IM), especially in pregnancy (preeclampsia/eclampsia)
- Chronic HF (combined with isosorbide dinitrate) - particularly beneficial in African Americans intolerant of ACE inhibitors/ARBs
- Perioperative hypertension - when tachycardia is absent
Nitrates mos
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Here is a complete breakdown of the mechanism of action of nitrates:
Nitrates - Mechanism of Action (MOA)
Drug Class
Organic nitrates: Nitroglycerin (GTN), Isosorbide dinitrate (ISDN), Isosorbide mononitrate (ISMN)
Step-by-Step Molecular Mechanism
Step 1: Bioactivation to Nitric Oxide (NO)
- Organic nitrates enter vascular smooth muscle cells and are metabolized (reduced) to release nitric oxide (NO) - or nitrite, which is further reduced to NO
- This requires enzymatic bioactivation (primarily via mitochondrial aldehyde dehydrogenase - ALDH2)
- NO can also be formed from the nitrite metabolite
Step 2: Activation of Soluble Guanylyl Cyclase (sGC)
- Released NO diffuses into vascular smooth muscle cells and binds to the heme moiety of soluble guanylyl cyclase (sGC)
- This activates sGC, converting GTP → cGMP (cyclic guanosine monophosphate)
Step 3: cGMP-Mediated Smooth Muscle Relaxation
- Elevated cGMP activates cGMP-dependent protein kinases (PKG)
- PKG phosphorylates myosin light chain kinase (MLCK), inactivating it
- Inactivation of MLCK → decreased intracellular Ca²+ → smooth muscle relaxation → vasodilation
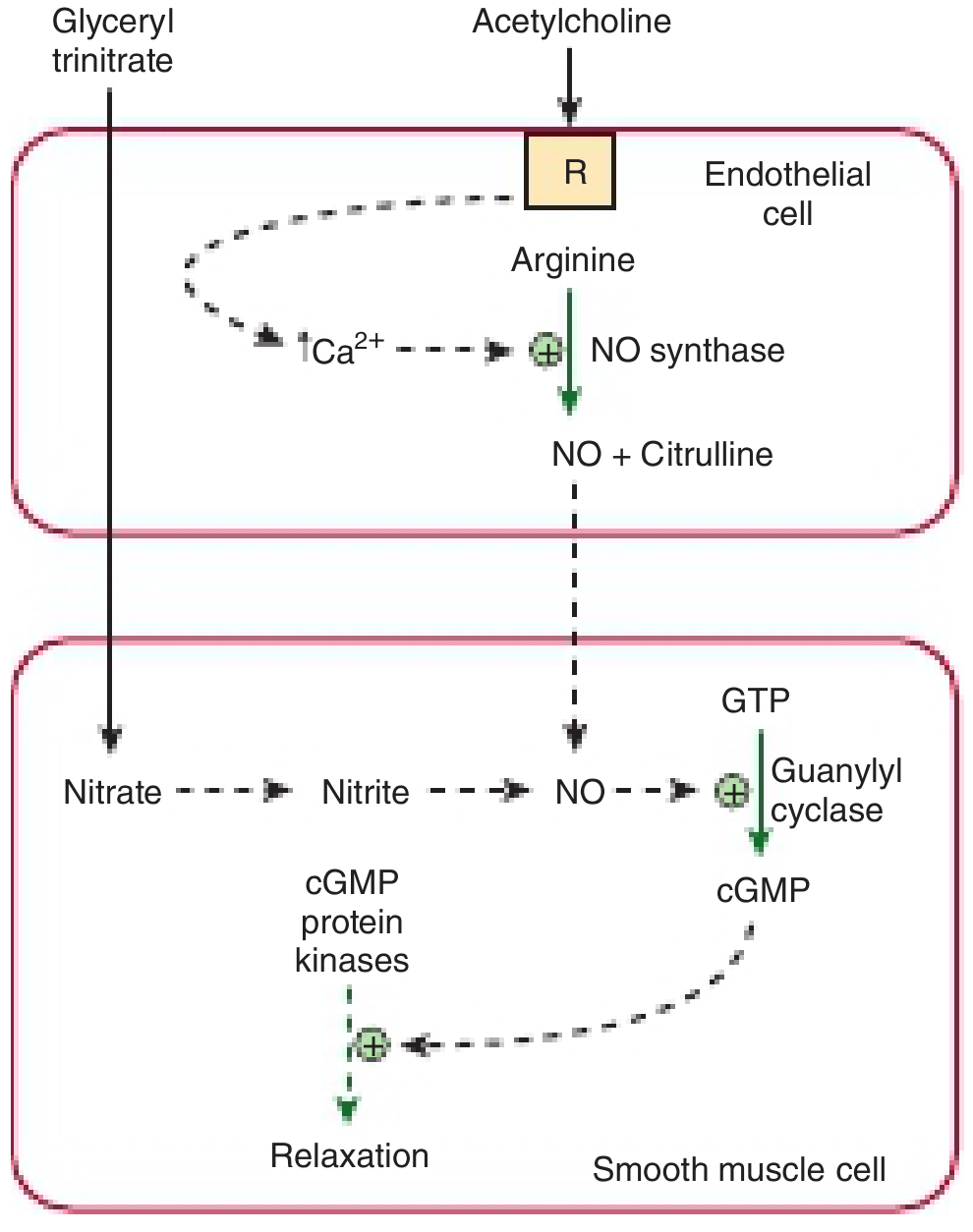
Nitroglycerin (glyceryl trinitrate) enters smooth muscle cells, metabolizes to nitrite → NO → activates guanylyl cyclase → cGMP → cGMP protein kinases → relaxation (Harper's Illustrated Biochemistry)
Vascular Selectivity: Veins > Arteries
| Vessel | Effect | Clinical Consequence |
|---|---|---|
| Veins (capacitance) | Strong dilation at low doses | ↓ Venous return → ↓ Preload → ↓ LV filling pressure |
| Arteries (resistance) | Dilation at higher doses | ↓ Afterload → ↓ SVR |
| Coronary arteries | Dilation (even at low doses) | ↑ Coronary blood flow, relief of vasospasm |
- At therapeutic doses, venodilation predominates - this is the key anti-anginal mechanism
- Arteriolar dilation occurs at higher doses, used in acute heart failure and hypertensive emergencies
(Morgan & Mikhail's Clinical Anesthesiology, p. 470)
How Nitrates Relieve Myocardial Ischemia
Nitrates reduce the O₂ supply-demand mismatch by:
- ↓ Preload - venous pooling in capacitance vessels → ↓ ventricular end-diastolic pressure → ↓ myocardial wall tension → ↓ O₂ demand + improved subendocardial perfusion
- ↓ Afterload (at higher doses) - arteriolar dilation → ↓ LV end-systolic pressure → ↓ O₂ demand
- ↑ Coronary blood flow - direct coronary artery dilation + collateral vessel dilation → redistribution of flow to ischemic subendocardium
- Relief of coronary vasospasm - important in Prinzmetal (variant) angina
(Fuster & Hurst's The Heart, 15th Ed.; Goldman-Cecil Medicine)
Additional effect: NO inhibits platelet aggregation (via cGMP in platelets) - antithrombotic benefit.
Tolerance (Tachyphylaxis)
- Continuous nitrate exposure leads to tolerance - reduced vasodilatory response
- Mechanism: depletion of sulfhydryl (-SH) groups needed for NO bioactivation; oxidative stress and ALDH2 inhibition
- Prevention: 8-12 hour nitrate-free interval daily (typically overnight)
(Goldman-Cecil Medicine)
Pharmacokinetics Summary
| Drug | Route | Onset | Duration | Notes |
|---|---|---|---|---|
| Nitroglycerin (GTN) | Sublingual | 1-3 min | 20-30 min | First-pass hepatic metabolism, bypassed sublingually |
| Nitroglycerin | IV infusion | Immediate | Infusion-dependent | Used in ACS, acute HF |
| Nitroglycerin | Transdermal patch | Slow | 24 h | Tolerance risk - needs patch-free period |
| Isosorbide dinitrate (ISDN) | Oral | 30-60 min | 4-6 h | Requires twice-daily dosing with gap |
| Isosorbide mononitrate (ISMN) | Oral | 30-60 min | 8-12 h | Active form, no first-pass metabolism |
- Metabolized by glutathione-organic nitrate reductase in liver and blood
- Nitrite metabolite can convert Hb → methemoglobin (rarely clinically significant; treat with IV methylene blue)
Key Clinical Uses
- Stable angina - sublingual GTN for acute attacks; long-acting nitrates for prophylaxis
- Unstable angina / NSTEMI - IV nitroglycerin for ongoing ischemia
- Acute decompensated heart failure - venodilation reduces pulmonary congestion
- Hypertensive emergency - IV nitroglycerin
- Esophageal spasm - smooth muscle relaxation
- Combined with hydralazine in HF (ISDN + hydralazine - especially in African Americans intolerant of ACE-I/ARB)
Side Effects (Direct from MOA)
- Headache - cerebral vessel dilation (most common)
- Hypotension / dizziness - excess venodilation
- Reflex tachycardia - baroreceptor response to BP drop
- Flushing - cutaneous vasodilation
- Methemoglobinemia - rare, with high doses
- Tolerance with continuous use
Contraindication
- Phosphodiesterase-5 (PDE5) inhibitors (sildenafil, tadalafil) - both raise cGMP via different mechanisms; combined use causes severe hypotension
This is a shared conversation. Sign in to Orris to start your own chat.