Can you tell me about hsv keratitis
Reading File
Finding Sources
Searching PubMed
"herpes simplex keratitis"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from Kanski's Ophthalmology, Goldman-Cecil, and Rosen's Emergency Medicine. Let me compile the full detailed answer.
Herpes Simplex Virus (HSV) Keratitis
HSV keratitis is the most common infectious cause of corneal blindness in developed countries. Up to 60% of corneal ulcers in developing countries may result from HSV, and an estimated 10 million people worldwide have herpetic eye disease. Approximately 10% of those with any history of HSK will eventually reach a final visual acuity of less than 6/60.
The Pathogen
HSV is a double-stranded DNA virus with two subtypes:
- HSV-1: Causes infection above the waist (principally the face, lips, and eyes). The main culprit in HSV keratitis.
- HSV-2: Genitally acquired; can rarely be transmitted to the eye through infected secretions or at birth (neonatal conjunctivitis).
The virus resides latently in neuronal ganglia (primarily the trigeminal ganglion) and reactivates under triggers such as UV light, stress, fever, trauma, immunosuppression, or systemic illness.
Clinical Classification
HSV keratitis is classified by the corneal layer involved:
1. Epithelial Keratitis (Dendritic Ulcer) - Most Common
- Caused by active viral replication in the corneal epithelium.
- Symptoms: Red eye, foreign body sensation, photophobia, tearing, reduced vision, and notably reduced corneal sensation (hypesthesia) due to viral damage to corneal nerves.
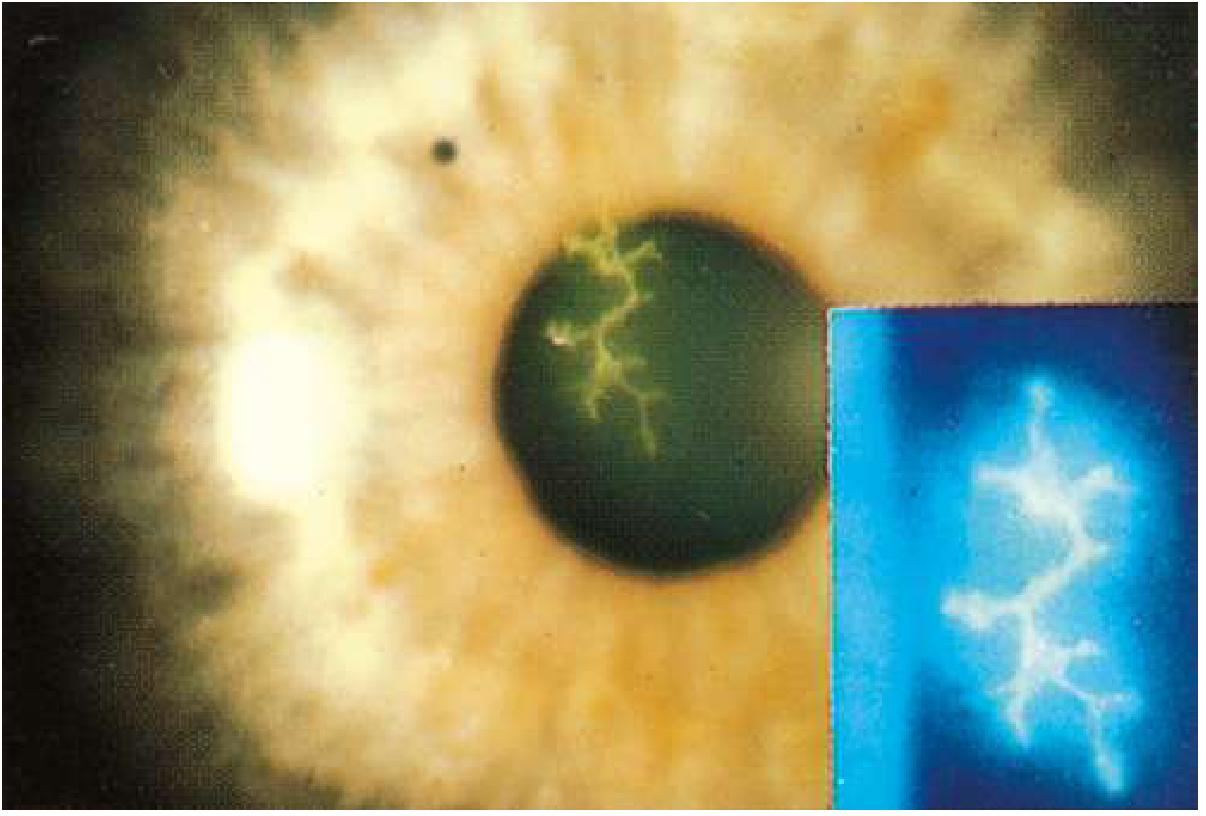
- Classic sign: A dendritic ulcer - a branching, tree-like epithelial lesion with terminal bulbs, which stains brilliantly with fluorescein and rose bengal.
- If untreated, the dendrite may enlarge into a geographic ulcer (ameboid shape), which heals more slowly.
- Key warning: Topical steroids are absolutely contraindicated in epithelial HSV keratitis - they worsen ulceration and can cause corneal perforation.
2. Disciform (Stromal) Keratitis - Immune-Mediated
- Also called endotheliitis. Etiology is unclear - may be active HSV infection of keratocytes/endothelium, or a hypersensitivity reaction to viral antigen.
- Symptoms: Gradual onset blurred vision, haloes around lights, mild discomfort and redness (milder than epithelial disease).
- Signs: Central zone of stromal oedema, often with overlying epithelial oedema; keratic precipitates (KPs) in the corresponding area of endothelium; raised intraocular pressure (IOP) due to trabeculitis.
- Unlike epithelial disease, topical steroids ARE used here (with antiviral cover) to suppress immune-mediated damage.
3. Necrotizing Stromal Keratitis - Most Severe
- Direct viral invasion of the stroma causing necrosis, dense infiltrate, and potentially perforation.
- Can lead to severe permanent corneal scarring.
4. Neurotrophic Keratopathy
- Results from chronic HSV-induced corneal anaesthesia and loss of trophic factors.
- The corneal surface breaks down despite the absence of active viral replication.
- Presents as a persistent epithelial defect, typically oval or round.
5. Iridocyclitis
- HSV can cause anterior uveitis, which may occur with or without evident keratitis.
Triggers for Recurrence
Reactivation of latent virus in the trigeminal ganglion is provoked by:
- UV light exposure
- Systemic illness / fever
- Physical or psychological stress
- Trauma or corneal surgery
- Immunosuppression (including topical or systemic steroids)
Diagnosis
Diagnosis is primarily clinical:
- Slit-lamp examination with fluorescein staining reveals the dendritic ulcer.
- Cobalt blue filter highlights the fluorescein-stained lesion vividly.
- Rose bengal staining stains devitalized epithelial cells and dendrite edges.
- Reduced corneal sensation tested with a wisp of cotton is a key supportive finding.
- Viral culture, PCR, and immunofluorescence are available but rarely needed clinically.
Treatment
Epithelial Keratitis
| Agent | Regimen |
|---|---|
| Ganciclovir 0.15% gel (topical) | 5 times daily for at least 1 week |
| Acyclovir 3% ophthalmic ointment | 5 times daily for 7-10 days |
| Oral acyclovir (if topical not tolerated) | 800 mg five times per day for 7-10 days |
| Valaciclovir / Famciclovir (oral) | Alternative oral agents, less frequent dosing |
- Debridement: Wiping the corneal surface with a sterile cellulose sponge or cotton-tipped applicator to physically remove virus-laden epithelial cells. Epithelium is removed 2 mm beyond the ulcer edge. Used for resistant cases or as an adjunct.
- Cycloplegia (e.g. homatropine 1%) for comfort.
- Avoid prostaglandin analogues for IOP control - they promote herpes virus activity.
Disciform (Stromal) Keratitis
- Topical steroids (e.g. prednisolone acetate, in tapering doses) with concurrent antiviral cover to prevent reactivation.
- The HEDS trial established that oral acyclovir reduces recurrence and that topical steroids + antiviral are beneficial for stromal disease.
Suppression of Recurrence
Patients with frequent recurrences benefit from long-term prophylaxis:
- Oral acyclovir 400-800 mg/day indefinitely
- This significantly reduces the rate of both epithelial and stromal recurrences.
End-Stage Disease
- Corneal transplantation (penetrating keratoplasty) for severe scarring - though recurrence in donor tissue limits success.
Complications
- Corneal scarring and opacification
- Persistent neurotrophic ulcers
- Corneal perforation (if steroids used inappropriately in epithelial disease, or from severe necrotizing keratitis)
- Glaucoma (from trabeculitis in disciform keratitis)
- Amblyopia (in children)
Key Pitfalls
- Do not use topical steroids for epithelial keratitis - this is the most dangerous mistake and can cause corneal perforation.
- Reduced corneal sensation can mask pain, leading to delayed presentation.
- Geographic ulcers (enlarged dendrites) may be mistaken for other keratitides.
- Mimics include acanthamoeba keratitis and fungal keratitis - consider these in resistant or atypical cases.
Sources: Kanski's Clinical Ophthalmology 10th Ed. (p. 220-225) | Goldman-Cecil Medicine International Ed. (Fig. 391-17) | Rosen's Emergency Medicine (p. 892)
This is a shared conversation. Sign in to Orris to start your own chat.