Stroke or CVA
Reading File
Finding Sources
Finding Sources
Searching PubMed
"stroke" AND "management"
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full stroke/CVA overview.
Stroke / Cerebrovascular Accident (CVA)
Definition & Overview
A stroke (CVA) is an acute focal neurological deficit resulting from a sudden interruption of blood supply to the brain. It is the leading cause of disability among all major neurological conditions and affects approximately 800,000 people annually in the United States. Globally, it was the second largest cause of death in 2016, responsible for 5.5 million deaths.
- Bradley and Daroff's Neurology in Clinical Practice classifies stroke into:
- Cerebral infarction (ischemic stroke) - >70% of all cases
- Intracerebral hemorrhage (ICH) - 10-15%
- Subarachnoid hemorrhage (SAH) - <5%
- Undetermined etiology - remainder
Classification
1. Ischemic Stroke (TOAST Classification)
The TOAST classification identifies these mechanisms:
| Mechanism | Description |
|---|---|
| Large-artery atherothrombosis | Stenosis/occlusion from atherosclerotic plaque rupture; artery-to-artery embolism |
| Small-vessel disease (lacunar) | Lipohyalinosis of small penetrating arteries, typically <1.5 cm infarcts |
| Cardioembolism | Source: atrial fibrillation (most common), intracardiac thrombus, valvular disease |
| Non-atherosclerotic vasculopathy | Dissection, vasculitis, Takayasu disease |
| Hypercoagulable states | Antiphospholipid syndrome, protein C/S deficiency, Factor V Leiden, etc. |
| Undetermined | Mixed or cryptogenic |
2. Hemorrhagic Stroke
Intracerebral Hemorrhage (ICH):
- Causes: hypertensive vasculopathy (most common), cerebral amyloid angiopathy, AVMs, cocaine use, anticoagulation
- Hypertensive hemorrhages occur in deep structures due to lipohyalinosis
Most common sites for hypertensive ICH:
| Site | Frequency | Clinical Presentation |
|---|---|---|
| Putamen | 44% | Contralateral motor/sensory deficit |
| Thalamus | 13% | Limb pain, speech difficulty |
| Cerebellum | 9% | Incoordination of trunk and limbs |
| Pons | 9% | Numbness, weakness, ataxia, dizziness |
| Other cortical | 25% | Variable |
ICH carries a 30-day mortality up to 50%, with half dying in the first 2 days. Only 1 in 5 survivors live independently at 6 months.
Pathophysiology
Normal cerebral blood flow (CBF) = 40-60 mL/100g/min
When CBF falls:
- Below 15-18 mL/100g/min: Brain loses electrical activity ("electrically silent"), neurons viable but non-functional - this produces the neurological deficit
- Below 10 mL/100g/min: Membrane failure occurs; extracellular K⁺ rises, intracellular Ca²⁺ rises - irreversible cell death
The ischemic penumbra is the zone of electrically silent but still viable tissue surrounding the infarcted core - this is the therapeutic target for reperfusion. If reperfusion is established quickly, the penumbra can be rescued.
Risk Factors
Non-modifiable:
- Age (risk doubles each decade after 55)
- Male sex, Black race
- Family history, prior TIA or stroke
Modifiable:
| Vascular | Cardiac | Lifestyle |
|---|---|---|
| Hypertension (most important) | Atrial fibrillation (5-fold risk increase; causes 1/6 of all strokes) | Smoking |
| Diabetes mellitus | Valvular heart disease | Obesity |
| Hypercholesterolemia | Low ejection fraction | Sedentary lifestyle |
| Carotid stenosis | Patent foramen ovale | Substance abuse (cocaine) |
Clinical Features
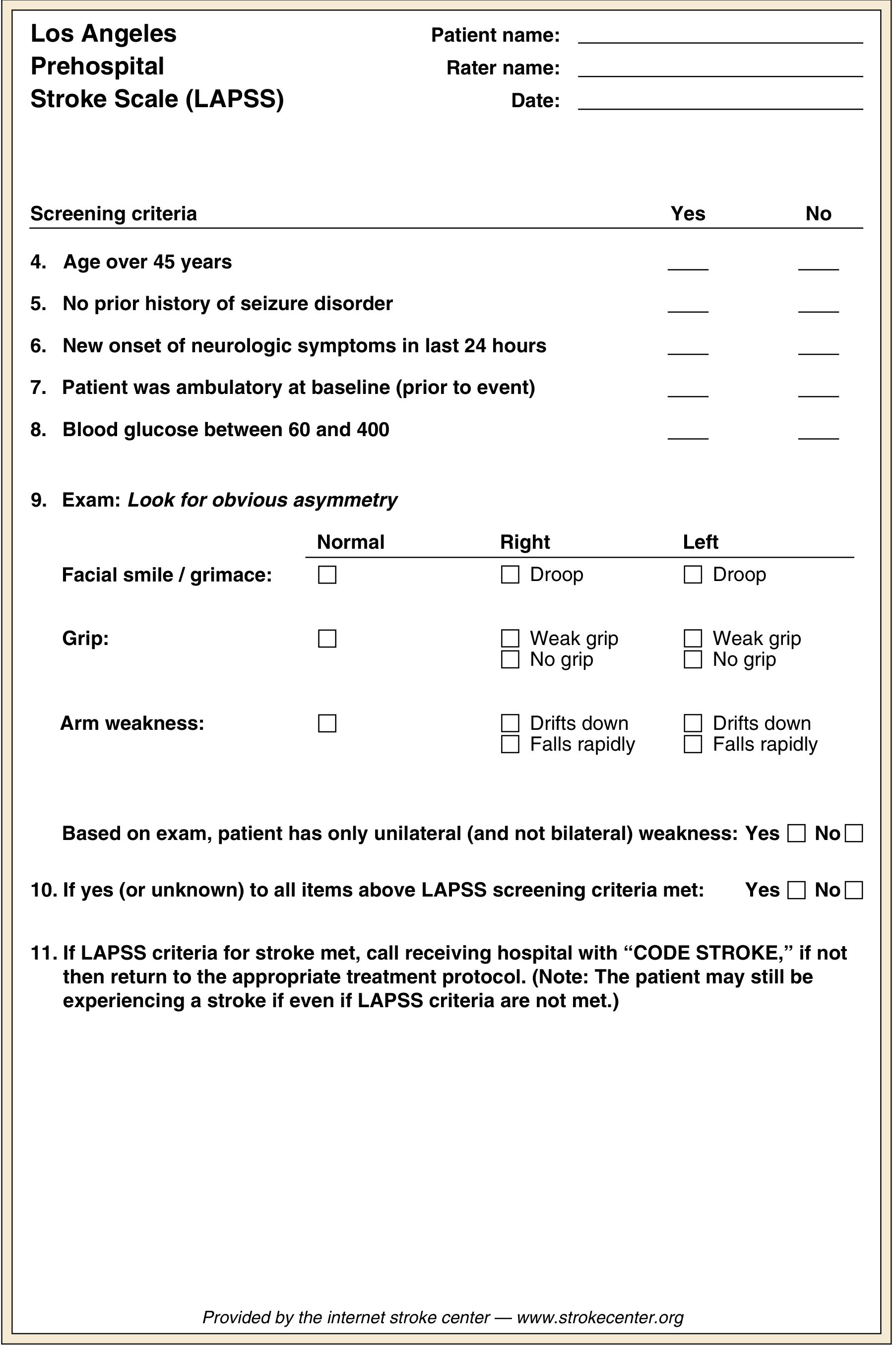
Prehospital Recognition - FAST / LAPSS
Anterior Circulation Strokes
Anterior Cerebral Artery (ACA):
- Contralateral leg weakness > arm weakness (opposite of MCA)
- Abulia, altered mentation, poor judgment, primitive reflexes (grasp, suck)
- Bowel and bladder incontinence
- Apraxia of gait
Middle Cerebral Artery (MCA) - most common:
- Contralateral hemiplegia and hemisensory loss (arm and face > leg)
- Contralateral homonymous hemianopsia
- Aphasia (if dominant hemisphere):
- Broca aphasia (expressive) - cannot speak fluently but comprehends
- Wernicke aphasia (receptive) - fluent but incomprehensible speech, impaired comprehension
- Contralateral gaze deviation (eyes look toward the lesion)
- Agnosia, spatial neglect (non-dominant hemisphere)
Posterior Cerebral Artery (PCA):
- Contralateral homonymous hemianopsia
- Visual agnosia, alexia
- Third nerve palsy (ipsilateral)
Posterior Circulation Strokes (Vertebrobasilar)
These are the most challenging to diagnose and can produce the widest variety of symptoms:
- Loss of consciousness (unique to posterior circulation)
- Nausea and vomiting (brainstem CTZ involvement)
- Diplopia, dysphagia, dysarthria ("the Ds")
- Ipsilateral cranial nerve deficits with contralateral long tract signs (crossed signs)
- Vertigo, ataxia, nystagmus
- Posterior strokes can progress for up to 3 days (vs. 24 hours for anterior strokes)
Diagnosis
Imaging
- Non-contrast CT - first line; rapidly excludes hemorrhage (hemorrhage appears hyperdense)
- CT Angiography (CTA) - identifies large vessel occlusion (LVO)
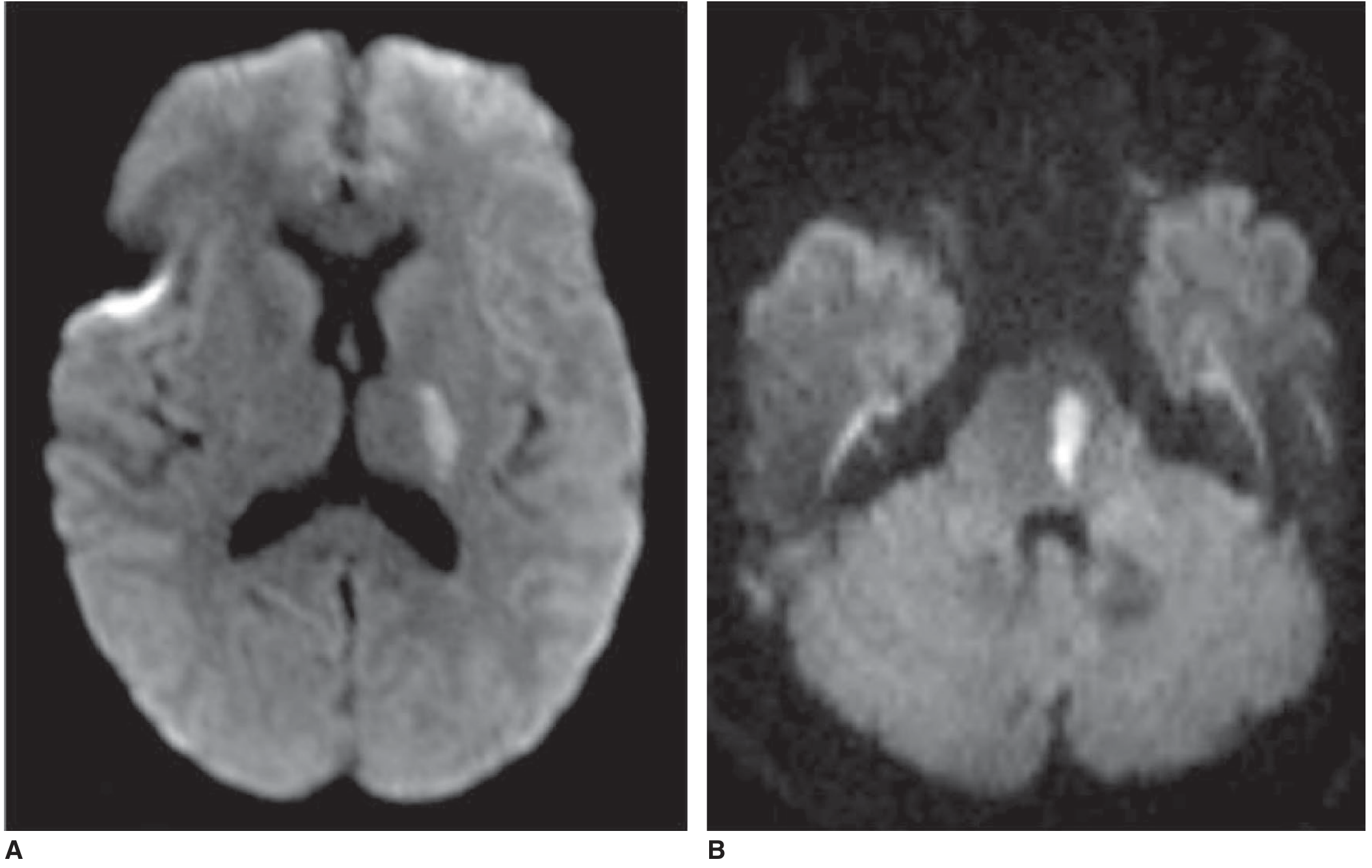
- MRI/DWI - most sensitive for acute ischemic stroke; diffusion restriction visible within minutes
- CT Perfusion / MRI Perfusion - identifies penumbra vs. infarct core (used for extended window eligibility)
Scoring Tools
- NIHSS (NIH Stroke Scale) - quantifies stroke severity (0-42); used to determine tPA eligibility and monitor progression
- Glasgow Coma Scale (GCS) - for ICH; serial exams detect hemorrhage expansion
- ICH Score - predicts mortality in hemorrhagic stroke
Management
Acute Ischemic Stroke - "Time is Brain"
Modern treatment approaches:
1. General Measures (All patients)
- Airway, breathing, circulation - ABC approach
- Supplemental O₂ if needed; avoid hyperthermia (worsens outcome); mild hypothermia is protective
- Cardiac monitoring for ≥48 hours (ECG + troponin on admission - 3-20% have concomitant myocardial ischemia)
- Blood pressure: optimal range post-stroke ~160-200 mmHg systolic; avoid over-treatment (impairs penumbra perfusion)
- Aspiration precautions - NPO until formal swallow evaluation; head-of-bed >30°
- Admission to a dedicated stroke unit - reduces mortality, hospital stay, and nursing-home discharge
- DVT prophylaxis
2. Reperfusion Strategies
| Therapy | Window | Indication |
|---|---|---|
| IV Alteplase (tPA) | ≤4.5 hours from onset | No contraindications (hemorrhage excluded by CT) |
| IV Tenecteplase | ≤4.5 hours | Alternative to alteplase (similar efficacy in trials) |
| Endovascular thrombectomy (EVT) | ≤6 hours (can extend to 24h with imaging mismatch) | Large vessel occlusion on CTA (distal ICA, proximal MCA) |
| Extended window EVT | 6-24 hours | Advanced imaging shows penumbra-infarct mismatch (DAWN/DEFUSE-3 criteria) |
If a patient wakes up with stroke symptoms ("wake-up stroke"), perfusion-diffusion mismatch on MRI determines eligibility rather than the clock.
3. Anticoagulation
- Heparin (UFH/LMWH): No proven benefit in reducing morbidity or mortality in most acute ischemic strokes (IST and FISS trials)
- May be considered for: cerebral venous thrombosis, small cardioembolic infarcts with intracardiac thrombus
- Not recommended if septic embolism suspected
4. Cytoprotective / Anti-inflammatory strategies - currently investigational; combined approaches are the future
Acute Hemorrhagic Stroke
- Reverse anticoagulation immediately (Vitamin K, PCC, FFP, protamine as appropriate)
- BP control: Lower rapidly in hypertensive ICH to reduce hematoma expansion
- Monitor ICP; neurosurgical consultation for cerebellar hemorrhage >3 cm, hydrocephalus, or deteriorating patient
- Serial neurological exams and imaging for expansion monitoring
- Avoid early care limitations - prognosis is uncertain in acute ICH
Secondary Prevention
| Strategy | Details |
|---|---|
| Antiplatelets | Aspirin 81-325 mg/day; clopidogrel for aspirin-intolerant patients |
| Anticoagulation | Warfarin or DOACs (rivaroxaban, apixaban) for AF-related stroke |
| Statins | For all atherosclerotic stroke regardless of LDL |
| BP control | Target <130/80 mmHg long-term |
| Carotid endarterectomy (CEA) | For symptomatic stenosis 70-99% (NASCET criteria) |
| Carotid stenting (CAS) | Alternative to CEA in selected patients |
| Intracranial stenting | For recurrent stroke despite optimal medical therapy with significant stenosis |
| Lifestyle | Smoking cessation, weight control, exercise, diabetes control |
After a stroke, recurrence risk is ~4% at 90 days, 5% at 1 year, and an additional 6% between years 1-5.
Transient Ischemic Attack (TIA)
A TIA is a focal neurological deficit resolving within 24 hours (most resolve within 1 hour) without infarction on imaging. It is a medical emergency - the risk of stroke after TIA is highest in the first 48-72 hours. Any TIA within 72 hours of symptom onset should be admitted to hospital for urgent evaluation and treatment.
Prognosis
- Stroke mortality in the US has declined by 75% since the late 1960s due to improved management and risk factor control
- Early rehabilitation begun within 24-48 hours improves functional outcomes
- Predictors of poor outcome in ICH: low GCS on arrival, large hematoma volume, intraventricular blood extension
- Globally, age-standardized stroke mortality decreased by 36.2% from 1990 to 2016
Sources:
- Bradley and Daroff's Neurology in Clinical Practice, Chapters 47, 65
- Rosen's Emergency Medicine, Chapter 87
- Adams and Victor's Principles of Neurology, 12th Ed., Chapter on Cerebrovascular Disease
- Neuroanatomy Through Clinical Cases, 3rd Ed., Table 10.4
I am a physiotherapist, can you help me with PT management?
Finding Sources
Searching PubMed
"stroke rehabilitation" AND "physical therapy"
Finding Sources
Searching PubMed
"stroke" AND "motor rehabilitation" AND "exercise"
Finding Sources
Searching PubMed
"stroke" AND "gait training" AND "balance"
Reading Article
PMID: 40401760
Reading Article
PMID: 39932103
Reading File
Reading File
Reading Article
PMID: 39406459
Reading Article
PMID: 38413134
Reading File
Finding Sources
This is a shared conversation. Sign in to Orris to start your own chat.