


1779121571570278309420560076682.jpg
+2 more
Explain visually
Reading File
Searching Images
aminoglycoside mechanism of action ribosome protein synthesis
Searching Images
aminoglycoside transport bacterial cell membrane
Loading Image
Here is a full visual breakdown of Chapter 54 — Aminoglycoside Antibiotics:
🦠 What Are Aminoglycosides?
Natural and semi-synthetic antibiotics with polybasic amino groups linked to aminosugar residues. All produced by soil actinomycetes.
| Category | Members |
|---|---|
| Systemic | Streptomycin, Gentamicin, Kanamycin, Tobramycin, Amikacin, Sisomicin, Netilmicin, Paromomycin |
| Topical | Neomycin, Framycetin |
⚙️ Mechanism of Action — Two Steps
Step 1 — Entry into the bacterial cell (multistep transport)
Outer coat (porin channels)
↓
Periplasmic space
↓ ← carrier-mediated, linked to electron transport chain
Cytoplasmic membrane ← Energy-Dependent Phase I (EDP₁)
↓
Inside cell
Why anaerobes are resistant: The carrier system is oxygen-dependent. Without O₂, the membrane is not polarized → drug can't get in. This also explains why abscesses (low O₂) reduce efficacy.
Why alkaline pH helps: Aminoglycosides are ~20× more active at alkaline pH. β-lactams and vancomycin (cell-wall agents) enhance entry by disrupting the outer barrier.
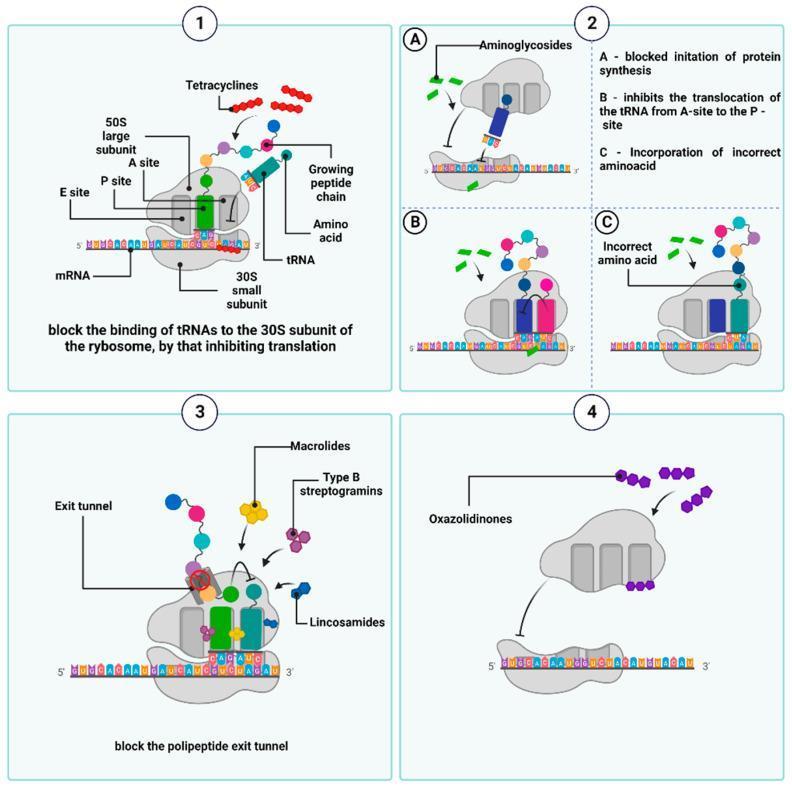
Step 2 — Ribosome binding → Protein synthesis inhibition
Aminoglycosides bind 30S ribosome (streptomycin) and also 50S subunit & 30S–50S interface (other members):
| Effect | Consequence |
|---|---|
| A Block initiation complex | Protein synthesis never starts |
| B Inhibit tRNA translocation (A→P site) | Elongation stops |
| C Distort mRNA codon recognition | Wrong amino acids incorporated → defective/toxic proteins |
These defective proteins insert into the cell membrane → membrane becomes permeable → ions, amino acids, proteins leak out → cell death (bactericidal, not just static).
This also triggers EDP₂ (Energy-Dependent Phase II) — more drug enters, reinforcing the lethal cycle.
🛡️ Mechanism of Resistance
3 Mechanisms:
1. Modifying enzymes (most important)
├─ Phosphorylate, adenylate, or acetylate the drug
├─ Modified drug can't bind ribosomes
└─ Encoded in plasmids → spread between bacteria
2. Ribosomal mutation
└─ Reduced affinity of ribosomal proteins → partial resistance
3. Decreased transport
├─ Outer coat porin channels become less permeable
└─ Active transport interfered → drug can't reach ribosome
Cross-resistance among aminoglycosides is variable (depends on which enzymes are present).
☠️ Shared Toxicities
Table 54.1 — Comparative Toxicity
| Drug | Vestibular Toxicity | Cochlear Toxicity | Nephrotoxicity |
|---|---|---|---|
| Streptomycin | ++ (high) | ± (low) | + |
| Gentamicin | ++ (high) | + | + |
| Kanamycin | + | ++ (high) | ++ |
| Tobramycin | +± | + | ++ |
| Amikacin | + | +± | +± |
| Sisomicin | +± | + | +± |
| Netilmicin | +± | + | +± |
1. 🔊 Ototoxicity (most important adverse effect)
Drug concentrates in labyrinthine fluid → slowly removed when plasma falls
↑ Plasma trough > threshold → concentration-dependent toxicity
For Gentamicin:
Trough > 2 μg/ml → vestibular damage (concentration-dependent)
Target trough < 1 μg/ml to avoid toxicity
Cochlear damage:
- Starts at base (high frequencies) → spreads to apex (low frequencies)
- Tinnitus → progressive hearing loss
- Sensory cells do NOT regenerate → damage is permanent
- Kanamycin & Amikacin = worst cochlear toxicity
Vestibular damage:
- Headache → nausea → dizziness → nystagmus → vertigo → ataxia
- Stop drug: enters chronic phase (6–10 weeks asymptomatic lying down, difficulty walking)
- Recovery over 1–2 years — often incomplete; elderly recover poorly
- Streptomycin & Gentamicin = worst vestibular toxicity
2. 🫘 Nephrotoxicity
Drug → high concentration in renal cortex (proximal tubules)
↓
Tubular damage → ↓ urinary concentrating power
↓
↓ GFR, nitrogen retention, albuminuria, casts
↓
↓ Drug clearance → ↑ blood levels → ↑ ototoxicity
- Single daily dosing causes less nephrotoxicity than thrice-daily dosing
- Worse in: elderly, pre-existing kidney disease
- If drug is stopped promptly → reversible
- Streptomycin = least nephrotoxic
3. 🧠 Neuromuscular Blockade
All aminoglycosides reduce ACh release at motor nerve endings by:
- Blocking synaptic vesicle fusion with terminal membrane (antagonize Ca²⁺)
- Reducing muscle end-plate sensitivity to ACh
Clinically silent usually, but apnoea and fatalities can occur if drug is put into peritoneal/pleural cavity after surgery (especially with curare-type muscle relaxants). Partially reversed by IV calcium salt. Myasthenic weakness is worsened.
⚠️ Precautions & Interactions
| Precaution | Reason |
|---|---|
| Avoid in pregnancy | Foetal ototoxicity |
| Avoid with NSAIDs, amphotericin B, vancomycin, cyclosporine, cisplatin | Additive nephrotoxicity |
| Caution with vancomycin, minocycline, furosemide | Potentially additive ototoxicity |
| Caution in patients >60 yrs or kidney disease | Reduced clearance, higher toxicity risk |
🔑 Common Properties (Memory Summary)
S-I-B-B-A-P-C-N-O
- Sulfate salts — highly water-soluble, stable for months
- Ionize in solution — not absorbed orally; no CNS/CSF penetration
- Bactericidal — more active at alkaline pH
- Bacteria targeted — aerobic gram-negative bacilli (not anaerobes)
- All excreted unchanged by glomerular filtration
- Partial cross-resistance only
- Concentration-distributed extracellularly only
- Narrow margin of safety
- Ototoxicity + nephrotoxicity in all members
This is a shared conversation. Sign in to Orris to start your own chat.