give me 10 images on ecg findings in mi
Reading File
Finding Sources
Searching Images
ECG findings in myocardial infarction ST elevation
Searching Images
ECG NSTEMI Q waves T wave inversion myocardial infarction
I now have 10 high-quality ECG images covering a wide range of MI findings. Here they are:
ECG Findings in Myocardial Infarction — 10 Images
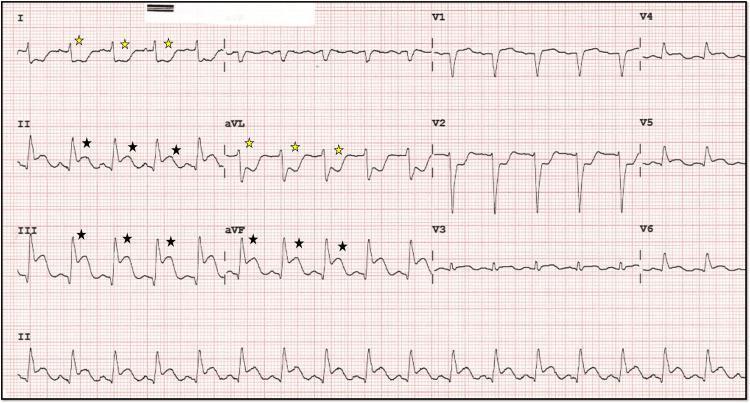
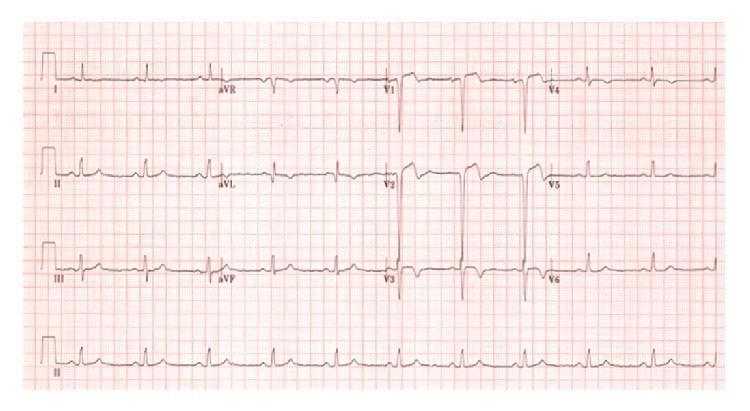
1. Acute Inferior STEMI — "Shark Fin" Morphology
Leads II, III, aVF — ST elevation with shark-fin fusion of QRS/ST/T. Reciprocal depression in I, aVL. Posterior involvement suggested by V1–V3 depression.
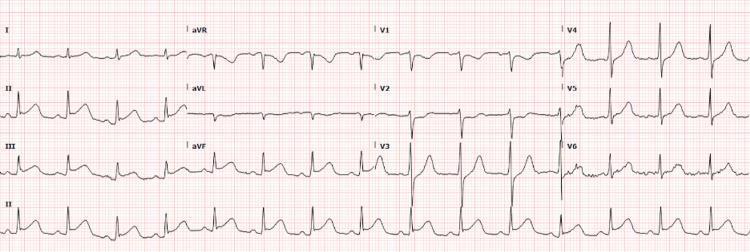
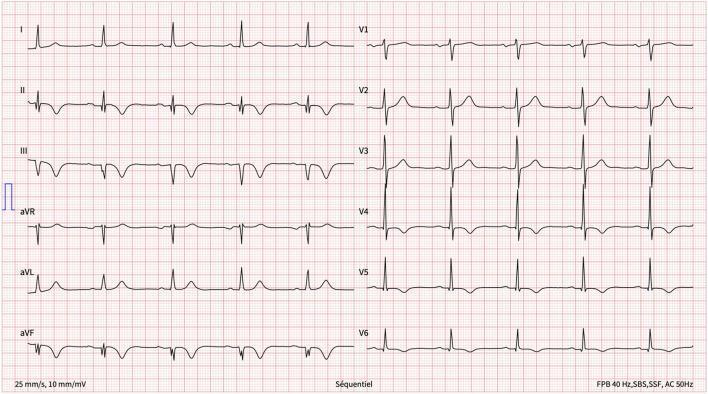
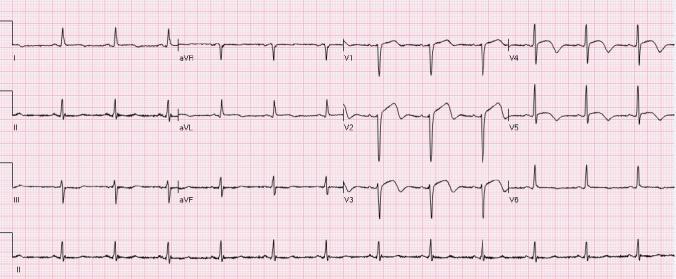
2. Acute Anterior STEMI — LAD Occlusion
Prominent ST elevation across V1–V6, most marked in V2–V4. Mild elevation in I, II, III, aVF. Classic pattern of left anterior descending (LAD) territory occlusion.

3. Anterolateral STEMI — LAD with Lateral Extension
ST elevation in V1–V6 + I + aVL (hyperacute T waves). Reciprocal ST depression in inferior leads II, III, aVF. Indicates proximal LAD occlusion involving diagonal branches.
4. Inferior STEMI — Tombstone Morphology
"Tombstone" ST elevation in II, III, aVF with deep reciprocal depression in V1–V3 and aVL. Sinus tachycardia with rightward axis, suggesting RCA or LCx occlusion.
5. Inferolateral STEMI with Sinus Bradycardia
ST elevation in II, III, aVF + V5–V6 with hyperacute T waves. Reciprocal depression in V1–V4 and aVL. Sinus bradycardia (~45–50 bpm) — typical of RCA-territory STEMI with vagal response.
6. Evolving Anteroseptal MI — Pathological Q Waves + T Inversion
Pathological Q waves in V1–V2, ST elevation in V1–V3, and deep T-wave inversions in I, aVL, V2–V4. Classic progression from acute STEMI toward subacute/evolving phase in LAD territory.
7. Subacute Inferior MI — Q Waves + Symmetric T Inversion
Pathological Q waves with deep symmetric T-wave inversions in II, III, aVF. Lateral extension to V5–V6. Consistent with evolving/subacute inferior-lateral MI (e.g., post-SCAD or late-presenting STEMI).
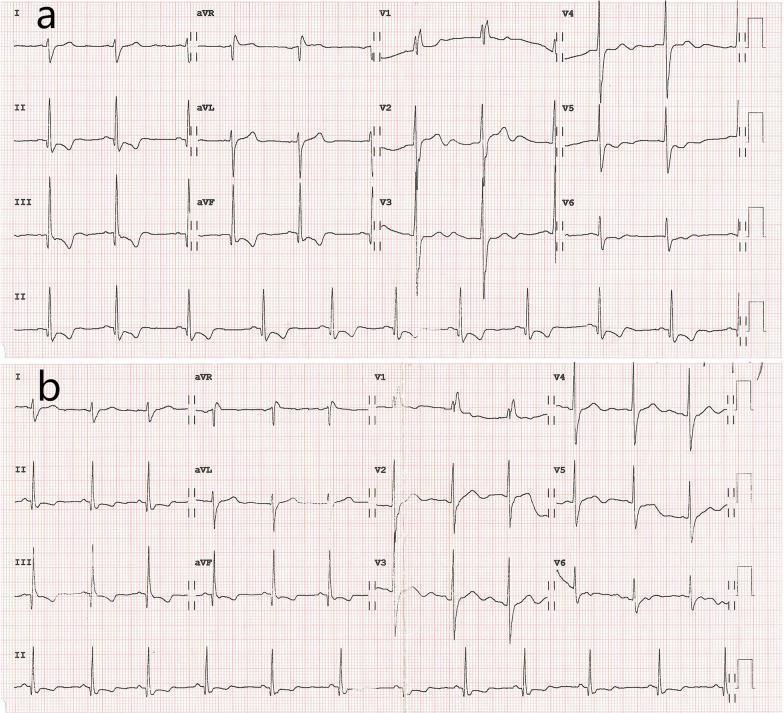
8. Old Inferior MI + RBBB — Before & After Stenting
Panel (a): Pathological Q waves in II, III, aVF + ST depression + T inversion + RBBB (rSR' in V1). Panel (b): Post-stenting with resolution of ischemic changes — Q waves and RBBB persist as permanent markers.
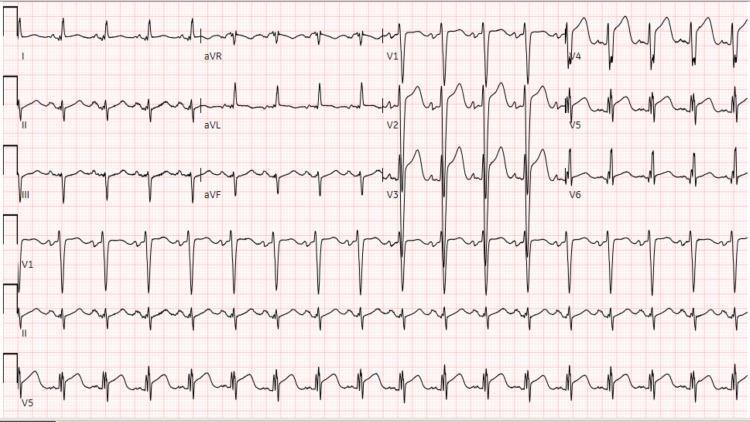
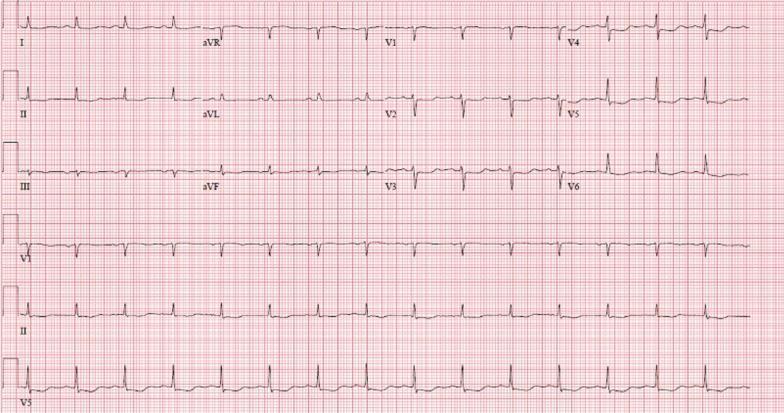
9. NSTEMI — Diffuse ST Depression with aVR Elevation
Sinus tachycardia. Diffuse horizontal/downsloping ST depression in I, aVL, V4–V6, II, III, aVF. Reciprocal ST elevation in aVR — hallmark of global subendocardial ischemia or left main/proximal LAD disease.
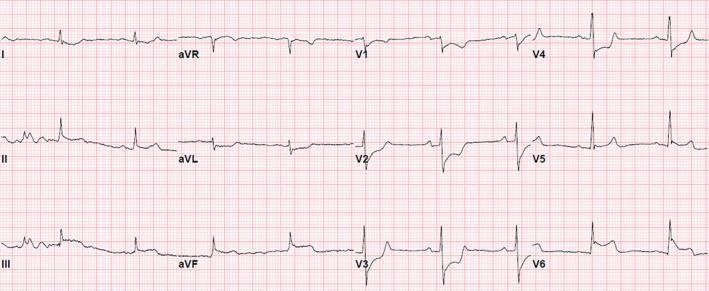
10. Wellens' Syndrome — Spontaneously Reperfused STEMI
Resolving ST elevation in V2–V5 with deep terminal T-wave inversions — the "Wellens' pattern." No pathological Q waves. This is a critical pre-infarction warning of proximal LAD critical stenosis requiring urgent intervention.
Quick Reference: ECG Findings by MI Type
| Type | Key Finding | Leads Affected |
|---|---|---|
| Anterior STEMI | ST elevation | V1–V4 |
| Anterolateral STEMI | ST elevation + lateral | V1–V6, I, aVL |
| Inferior STEMI | ST elevation | II, III, aVF |
| Inferolateral STEMI | ST elevation | II, III, aVF, V5–V6 |
| NSTEMI | ST depression ± T inversion | Diffuse / aVR elevation |
| Evolving MI | Pathological Q waves + T inversion | Territory-specific |
| Wellens' Syndrome | Biphasic/deep T inversion | V2–V5 |
| Posterior MI | Tall R + ST depression | V1–V3 (mirror image) |
can you create a ppt for this. iclude all images
Reading File
Reading File
Running Command
mkdir -p /home/daytona/workspace/ecg-mi-ppt && node /home/daytona/skills/shared/…
Writing File
~/ecg-mi-ppt/create_ppt.js
const pptxgen = require("pptxgenjs");
const fs = require("fs");
const images = JSON.parse(fs.readFileSync("/home/daytona/workspace/ecg-mi-ppt/images.json", "utf8"));
// Color palette — dark cardiology theme
const BG_DARK = "0A1628"; // deep navy
const BG_CARD = "112240"; // slightly lighter navy for cards
const ACCENT = "E63946"; // ECG red
const ACCENT2 = "457B9D"; // calm blue
const WHITE = "FFFFFF";
const LIGHT_GRAY = "A8B2C1";
const GOLD = "F4A261";
const slides_data = [
{
title: "Acute Inferior STEMI",
subtitle: "\"Shark Fin\" Morphology",
territory: "RCA / LCx Territory",
leads: "Leads II, III, aVF",
points: [
"ST elevation with tombstone / shark-fin fusion of QRS–ST–T",
"Reciprocal ST depression in I and aVL",
"V1–V3 depression suggests posterior wall involvement",
"ST elevation in III > II points to RCA occlusion"
],
imgIndex: 0
},
{
title: "Acute Anterior STEMI",
subtitle: "LAD Occlusion — Classic Pattern",
territory: "LAD Territory",
leads: "Leads V1 – V4",
points: [
"Prominent ST elevation across V1–V6 (most marked V2–V4)",
"Mild ST elevation also in I, II, III, aVF",
"Loss of R-wave progression in anterior leads",
"Reciprocal depression may appear in inferior leads"
],
imgIndex: 1
},
{
title: "Anterolateral STEMI",
subtitle: "Proximal LAD with Diagonal Branch Involvement",
territory: "LAD (proximal) Territory",
leads: "Leads V1–V6, I, aVL",
points: [
"ST elevation in V1–V6 + I + aVL — hyperacute T waves",
"Reciprocal ST depression in inferior leads II, III, aVF",
"Diagonal branch occlusion adds high lateral involvement",
"Largest zone of LAD territory at risk"
],
imgIndex: 2
},
{
title: "Inferior STEMI",
subtitle: "Tombstone Morphology",
territory: "RCA Territory",
leads: "Leads II, III, aVF",
points: [
"Massive convex ST elevation — \"tombstone\" appearance",
"Deep reciprocal depression in V1–V3 and aVL",
"Sinus tachycardia with rightward axis deviation",
"Consider RV infarction: check right-sided leads (V4R)"
],
imgIndex: 3
},
{
title: "Inferolateral STEMI",
subtitle: "Sinus Bradycardia — Vagal Response",
territory: "RCA or LCx Territory",
leads: "Leads II, III, aVF + V5–V6",
points: [
"ST elevation in inferior + lateral leads (V5–V6)",
"Hyperacute T waves with reciprocal depression in V1–V4, aVL",
"Sinus bradycardia (~45–50 bpm) — vagal RCA response",
"LCx: inferior > lateral; RCA: lateral > inferior"
],
imgIndex: 4
},
{
title: "Evolving Anteroseptal MI",
subtitle: "Pathological Q Waves + T Inversion",
territory: "LAD (Septal) Territory",
leads: "Leads V1–V4, I, aVL",
points: [
"Pathological Q waves in V1–V2 (transmural necrosis)",
"Residual ST elevation in V1–V3",
"Deep T-wave inversions I, aVL, V2–V4",
"Represents progression: acute → subacute phase of anterior MI"
],
imgIndex: 5
},
{
title: "Subacute Inferior MI",
subtitle: "Evolving Q Waves + Symmetric T Inversion",
territory: "Inferior Wall (RCA / SCAD)",
leads: "Leads II, III, aVF, V5–V6",
points: [
"Pathological Q waves with symmetric T-wave inversions in II, III, aVF",
"T inversion extending to lateral leads V5–V6",
"Typical of late-presenting STEMI or post-SCAD",
"No ongoing ST elevation — hours to days after event"
],
imgIndex: 6
},
{
title: "Old Inferior MI + RBBB",
subtitle: "Pre and Post Coronary Stenting",
territory: "Inferior Wall — Chronic",
leads: "Leads II, III, aVF + V1 (RBBB)",
points: [
"Pathological Q waves in II, III, aVF — permanent infarct scar",
"RBBB: widened QRS + rSR' pattern in V1",
"Pre-stenting: ST depression + T inversion (ongoing ischemia)",
"Post-stenting: ischemic changes resolve; Q waves + RBBB persist"
],
imgIndex: 7
},
{
title: "NSTEMI",
subtitle: "Diffuse ST Depression — Global Subendocardial Ischemia",
territory: "Diffuse / Left Main – Proximal LAD",
leads: "I, aVL, V4–V6, II, III, aVF + aVR elevation",
points: [
"Diffuse horizontal/downsloping ST depression across multiple leads",
"Reciprocal ST elevation in aVR — hallmark of global ischemia",
"Suggests left main or proximal LAD occlusion",
"No ST elevation — troponin elevation confirms NSTEMI"
],
imgIndex: 8
},
{
title: "Wellens' Syndrome",
subtitle: "Spontaneously Reperfused LAD — Critical Pre-Infarction Warning",
territory: "Proximal LAD Territory",
leads: "Leads V2 – V5",
points: [
"Resolving ST elevation with deep terminal T-wave inversions (Type B)",
"No pathological Q waves — myocardium still viable",
"Pain-free at presentation — patient may appear stable",
"URGENT: catheterization needed; stress test is CONTRAINDICATED"
],
imgIndex: 9
}
];
let pres = new pptxgen();
pres.layout = "LAYOUT_16x9";
pres.title = "ECG Findings in Myocardial Infarction";
pres.author = "Orris Medical";
// ─── TITLE SLIDE ───────────────────────────────────────────────────────────
{
let s = pres.addSlide();
// Background
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: "100%", h: "100%", fill: { color: BG_DARK } });
// Red accent bar left
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 0.12, h: "100%", fill: { color: ACCENT } });
// ECG-style decorative line (horizontal squiggle simulation with thin rect)
s.addShape(pres.ShapeType.rect, { x: 0.25, y: 2.7, w: 9.5, h: 0.03, fill: { color: ACCENT }, line: { color: ACCENT } });
// Title
s.addText("ECG FINDINGS IN", {
x: 0.5, y: 1.1, w: 9, h: 0.7,
fontSize: 22, bold: true, color: LIGHT_GRAY,
charSpacing: 8, align: "center", fontFace: "Arial"
});
s.addText("MYOCARDIAL INFARCTION", {
x: 0.5, y: 1.7, w: 9, h: 1.0,
fontSize: 38, bold: true, color: WHITE,
charSpacing: 4, align: "center", fontFace: "Arial"
});
// Subtitle
s.addText("A Visual Guide to STEMI, NSTEMI & Evolving MI Patterns", {
x: 0.5, y: 2.85, w: 9, h: 0.5,
fontSize: 15, color: ACCENT2, align: "center", italic: true, fontFace: "Arial"
});
// Bottom bar
s.addShape(pres.ShapeType.rect, { x: 0, y: 5.2, w: "100%", h: 0.425, fill: { color: ACCENT } });
s.addText("10 Illustrative ECG Cases | Emergency Cardiology Education", {
x: 0.5, y: 5.22, w: 9, h: 0.38,
fontSize: 12, color: WHITE, align: "center", bold: true, fontFace: "Arial"
});
// Small tags
const tags = ["STEMI", "NSTEMI", "Q WAVES", "T INVERSION", "WELLENS'", "RECIPROCAL CHANGES"];
tags.forEach((tag, i) => {
const col = i < 3 ? 0 : 3;
const row = i % 3;
s.addShape(pres.ShapeType.roundRect, {
x: 0.55 + col * 1.65, y: 3.55 + row * 0.45, w: 1.5, h: 0.33,
fill: { color: BG_CARD }, line: { color: ACCENT2, w: 1 },
rectRadius: 0.05
});
s.addText(tag, {
x: 0.55 + col * 1.65, y: 3.55 + row * 0.45, w: 1.5, h: 0.33,
fontSize: 9, color: ACCENT2, align: "center", bold: true, fontFace: "Arial", margin: 0
});
});
}
// ─── CONTENT SLIDES ────────────────────────────────────────────────────────
slides_data.forEach((d, idx) => {
let s = pres.addSlide();
const img = images[d.imgIndex];
// Background
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: "100%", h: "100%", fill: { color: BG_DARK } });
// Left accent bar
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 0.08, h: "100%", fill: { color: ACCENT } });
// Header bar
s.addShape(pres.ShapeType.rect, { x: 0.08, y: 0, w: 9.92, h: 0.85, fill: { color: BG_CARD } });
// Slide number badge
s.addShape(pres.ShapeType.ellipse, { x: 0.12, y: 0.1, w: 0.6, h: 0.6, fill: { color: ACCENT } });
s.addText(`${idx + 1}`, {
x: 0.12, y: 0.1, w: 0.6, h: 0.6,
fontSize: 16, bold: true, color: WHITE, align: "center", valign: "middle", margin: 0, fontFace: "Arial"
});
// Title
s.addText(d.title, {
x: 0.85, y: 0.08, w: 7.0, h: 0.42,
fontSize: 20, bold: true, color: WHITE, fontFace: "Arial", margin: 0
});
s.addText(d.subtitle, {
x: 0.85, y: 0.48, w: 7.0, h: 0.3,
fontSize: 12, color: ACCENT2, italic: true, fontFace: "Arial", margin: 0
});
// Territory badge (top right)
s.addShape(pres.ShapeType.roundRect, {
x: 7.95, y: 0.1, w: 1.9, h: 0.62,
fill: { color: ACCENT }, line: { color: ACCENT }, rectRadius: 0.08
});
s.addText(d.territory, {
x: 7.95, y: 0.1, w: 1.9, h: 0.62,
fontSize: 8.5, color: WHITE, align: "center", valign: "middle", bold: true, fontFace: "Arial", margin: 2
});
// ── ECG IMAGE (left panel) ──
if (img && img.base64 && !img.error) {
s.addImage({
data: img.base64,
x: 0.15, y: 0.95, w: 5.6, h: 3.5
});
}
// Image border
s.addShape(pres.ShapeType.rect, {
x: 0.15, y: 0.95, w: 5.6, h: 3.5,
fill: { type: "none" }, line: { color: ACCENT2, w: 1.5 }
});
// ── RIGHT PANEL ──
// Leads box
s.addShape(pres.ShapeType.roundRect, {
x: 5.9, y: 0.95, w: 3.95, h: 0.55,
fill: { color: BG_CARD }, line: { color: GOLD, w: 1.5 }, rectRadius: 0.06
});
s.addText([
{ text: "KEY LEADS: ", options: { bold: true, color: GOLD } },
{ text: d.leads, options: { color: WHITE } }
], {
x: 5.9, y: 0.95, w: 3.95, h: 0.55,
fontSize: 10, fontFace: "Arial", valign: "middle", margin: 6
});
// Key findings header
s.addText("KEY ECG FINDINGS", {
x: 5.9, y: 1.62, w: 3.95, h: 0.3,
fontSize: 10, bold: true, color: ACCENT, charSpacing: 2, fontFace: "Arial", margin: 0
});
// Bullet points
d.points.forEach((pt, i) => {
// bullet dot
s.addShape(pres.ShapeType.ellipse, {
x: 5.9, y: 2.02 + i * 0.58, w: 0.12, h: 0.12,
fill: { color: ACCENT2 }
});
s.addText(pt, {
x: 6.1, y: 1.94 + i * 0.58, w: 3.7, h: 0.52,
fontSize: 10.5, color: LIGHT_GRAY, fontFace: "Arial",
valign: "middle", wrap: true, margin: 0
});
});
// Bottom caption bar
s.addShape(pres.ShapeType.rect, { x: 0.08, y: 4.55, w: 9.92, h: 1.075, fill: { color: BG_CARD } });
s.addShape(pres.ShapeType.rect, { x: 0.08, y: 4.55, w: 9.92, h: 0.03, fill: { color: ACCENT2 } });
s.addText("Clinical Significance", {
x: 0.25, y: 4.6, w: 2.2, h: 0.3,
fontSize: 9, bold: true, color: ACCENT2, fontFace: "Arial", margin: 0
});
const clinicalNotes = [
"Immediate reperfusion if onset <12h. Assess for RV infarct with V4R.",
"Largest anterior territory. High mortality — door-to-balloon <90 min.",
"Proximal LAD occlusion. Consider Sgarbossa criteria if LBBB present.",
"Beware RV infarct — avoid nitrates; fluid-resuscitate if hypotensive.",
"Sinus bradycardia: atropine if symptomatic. Screen for posterior STEMI.",
"Evolving MI — Q waves indicate irreversible necrosis. Assess for VF risk.",
"Subacute phase: risk stratify with echo for wall motion abnormality.",
"RBBB post-MI raises mortality. Temporary pacing if bifascicular block.",
"aVR elevation = left main equivalent. Urgent angio for cardiogenic shock.",
"CONTRAINDICATED: stress test. Admit for urgent cath — high re-occlusion risk."
];
s.addText(clinicalNotes[idx], {
x: 0.25, y: 4.9, w: 9.5, h: 0.65,
fontSize: 11, color: WHITE, fontFace: "Arial", wrap: true, margin: 0
});
});
// ─── SUMMARY SLIDE ──────────────────────────────────────────────────────────
{
let s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: "100%", h: "100%", fill: { color: BG_DARK } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 0.08, h: "100%", fill: { color: ACCENT } });
s.addShape(pres.ShapeType.rect, { x: 0.08, y: 0, w: 9.92, h: 0.75, fill: { color: BG_CARD } });
s.addText("QUICK REFERENCE SUMMARY", {
x: 0.25, y: 0.1, w: 9.5, h: 0.55,
fontSize: 20, bold: true, color: WHITE, charSpacing: 4, align: "center", fontFace: "Arial"
});
const tableData = [
[
{ text: "MI Type", options: { bold: true, color: WHITE } },
{ text: "Key ECG Finding", options: { bold: true, color: WHITE } },
{ text: "Leads Affected", options: { bold: true, color: WHITE } },
{ text: "Artery", options: { bold: true, color: WHITE } }
],
["Anterior STEMI", "ST elevation, loss of R wave", "V1–V4", "LAD"],
["Anterolateral STEMI", "ST elevation + lateral changes", "V1–V6, I, aVL", "Proximal LAD"],
["Inferior STEMI", "ST elevation, tombstone / shark fin", "II, III, aVF", "RCA"],
["Inferolateral STEMI", "ST elevation inferior + lateral", "II, III, aVF, V5–V6", "RCA / LCx"],
["Evolving Anterior MI", "Pathological Q waves + T inversion", "V1–V4", "LAD (subacute)"],
["Subacute Inferior MI", "Q waves + symmetric T inversion", "II, III, aVF", "RCA (evolving)"],
["Old MI + RBBB", "Persistent Q waves, rSR' in V1", "II, III, aVF + V1", "RCA (chronic)"],
["NSTEMI", "Diffuse ST depression, aVR elevation", "Diffuse + aVR", "LM / LAD"],
["Wellens' Syndrome", "Deep T inversion, no Q waves", "V2–V5", "Proximal LAD"]
];
s.addTable(tableData, {
x: 0.15, y: 0.85, w: 9.7, h: 4.55,
fontSize: 9.5,
fontFace: "Arial",
align: "left",
valign: "middle",
color: LIGHT_GRAY,
fill: { color: BG_CARD },
border: { type: "solid", color: "1E3A5F", pt: 0.5 },
rowH: 0.44,
firstRowAsHeader: true,
autoPage: false,
colW: [1.9, 2.8, 2.3, 1.7],
});
}
pres.writeFile({ fileName: "/home/daytona/workspace/ecg-mi-ppt/ECG_Findings_in_MI.pptx" })
.then(() => console.log("PPT created successfully"))
.catch(e => { console.error(e); process.exit(1); });
Running Command
cd /home/daytona/workspace/ecg-mi-ppt && node create_ppt.js
Running Command
ls -lh /home/daytona/workspace/ecg-mi-ppt/ECG_Findings_in_MI.pptx
Your presentation is ready! 🫀
ECG Findings in MI
Presentation · PPTX
What's inside (12 slides total):
| Slide | Content |
|---|---|
| 1 | Title slide — dark cardiology theme with topic tags |
| 2–11 | One slide per ECG case — each with the full ECG image, key leads badge, territory label, 4 bullet findings, and a clinical significance note |
| 12 | Summary reference table — all 9 MI types with key findings, leads & culprit artery |
Design highlights:
- Deep navy background with ECG-red accent — clinical, high-contrast
- Each slide: ECG image on the left (large), key findings panel on the right
- Gold "KEY LEADS" badge, territory badge, slide number, and clinical note footer on every content slide
This is a shared conversation. Sign in to Orris to start your own chat.