Pt with OA knee admitted for TKR, on evaluation pt had leucopenia and thrombocyropenia, with ph smear showing normocytic nirmochromic cells with eosinophila, ct abdomen showed massive spleenomegaly of 20mm
massive splenomegaly leukopenia thrombocytopenia eosinophilia normocytic normochromic anemia differential diagnosis
massive splenomegaly leukopenia thrombocytopenia eosinophilia differential diagnosis
Clinical Analysis: OA Knee Patient with Unexpected Hematological Findings
Clarification on Spleen Size
Putting the Picture Together
- Leukopenia + thrombocytopenia (cytopenia in 2 cell lines)
- Normocytic normochromic RBCs on peripheral smear
- Eosinophilia
- Massive splenomegaly (20cm)
Top Differential Diagnoses
1. Visceral Leishmaniasis (Kala-azar) - Most Likely
- Classic triad: massive splenomegaly + pancytopenia + fever/weight loss
- Eosinophilia can coexist, though the Leishmania parasite classically suppresses eosinophils (so its presence may indicate a concurrent helminthic co-infection, which is common in endemic areas)
- Hypersplenism causes leukopenia and thrombocytopenia
- Normocytic anemia from hemodilution and bone marrow infiltration
- Key question: travel history to endemic regions (Indian subcontinent, East Africa, Mediterranean, Brazil)?
2. Schistosomiasis (Hepatosplenic form)
- A very strong candidate given the eosinophilia (parasitic worm = eosinophilia par excellence)
- Hepatosplenic schistosomiasis causes portal hypertension → massive splenomegaly → hypersplenism → leukopenia + thrombocytopenia
- Eosinophilia is a hallmark of the tissue-invasive phase and chronic infection
- Normocytic normochromic anemia from hypersplenism
3. Hyperreactive Malarial Splenomegaly (Tropical Splenomegaly Syndrome)
- Massive splenomegaly in chronic/repeated malaria exposure
- Leukopenia, thrombocytopenia from hypersplenism
- Eosinophilia may be present if there is co-infection
- Anemia is typically normocytic normochromic
4. Primary Myelofibrosis / Myeloproliferative Neoplasm
- Causes massive splenomegaly (extramedullary hematopoiesis)
- Leukopenia + thrombocytopenia when marrow is replaced
- Smear should show teardrop cells (dacrocytes) and leukoerythroblastic picture - absence of these makes this less likely
- Eosinophilia can occur in some myeloproliferative disorders (e.g., CML with eosinophilia)
5. Chronic Myeloid Leukemia (CML)
- Massive splenomegaly is characteristic
- WBC is usually high (not low) - so leukopenia argues against CML unless accelerated/blast phase
- Eosinophilia/basophilia is typical
6. Portal Hypertension (Cirrhosis)
- Common cause of congestive splenomegaly with hypersplenism
- Leukopenia + thrombocytopenia are well-recognized
- Would expect other stigmata (jaundice, ascites, spider naevi, elevated LFTs)
- Does NOT explain eosinophilia
7. Felty Syndrome
- Triad: RA + neutropenia + splenomegaly
- Patient has OA (not RA), so less likely - but worth noting if joints are actually inflammatory
Mechanism of Cytopenias in Hypersplenism
"Massive spleens are capable of sequestering up to 90% of peripheral platelets, 65% of granulocytes, and 30% of RBCs. Splenomegaly can also cause pancytopenia via hemodilution."
Workup Recommended Before TKR
- Catastrophic intraoperative hemorrhage from thrombocytopenia
- Septic complications from leukopenia
- Missing a potentially life-threatening systemic disease
| Investigation | Purpose |
|---|---|
| Peripheral smear review | Look for parasites (malaria), teardrop cells, blast cells, microfilaria |
| Bone marrow biopsy/aspirate | Infiltrative disease, leishmaniasis amastigotes, myelofibrosis |
| LFTs + coagulation screen | Portal hypertension, liver disease |
| Serology: Leishmania rK39 antigen/PCR | Visceral leishmaniasis |
| Stool O&P, schistosomal antibodies/antigen | Schistosomiasis |
| Thick/thin blood film x3 | Malaria |
| BCR-ABL, JAK2 mutation | CML, myeloproliferative neoplasm |
| LDH, uric acid | Lymphoma, hematologic malignancy |
| HIV, EBV, CMV serology | Infectious causes |
| Platelet count trend | Quantify severity of thrombocytopenia |
Bottom Line
- Frameworks for Internal Medicine, p. 366
- Harrison's Principles of Internal Medicine 22E, p. 2758
Why not hyperspleenism cause pancytopenia
Hypersplenism DOES Cause Pancytopenia
What is Hypersplenism?
"Hypersplenism is characterized by splenomegaly and one or more peripheral cytopenias in the setting of normo- or hypercellular bone marrow. When hypersplenism is the sole driver of pancytopenia, splenectomy is often curative."
How Does the Enlarged Spleen Cause Pancytopenia?
| Mechanism | Effect |
|---|---|
| Sequestration | Spleen traps circulating blood cells - up to 90% of platelets, 65% of granulocytes, 30% of RBCs |
| Premature destruction | Enlarged spleen destroys cells faster than the marrow can replace them |
| Hemodilution | Plasma volume expands in splenomegaly, diluting all cell lines |
Why I Distinguished Hypersplenism from the Primary Diagnosis
Underlying Disease (e.g. Leishmaniasis / Schistosomiasis)
↓
Massive Splenomegaly
↓
Hypersplenism
↓
Pancytopenia (leukopenia + thrombocytopenia + anemia)
Summary
-
Hypersplenism = YES, it causes the pancytopenia in this patient
-
The spleen sequesters WBCs, platelets, and RBCs explaining leukopenia, thrombocytopenia, and normocytic normochromic anemia
-
But hypersplenism is a syndrome secondary to an underlying disease - the workup must identify what is causing the massive spleen
-
The eosinophilia sits outside the hypersplenism explanation and is the pointer toward the underlying parasitic etiology
-
Frameworks for Internal Medicine, p. 366
Create a diagnostic algorithm for massive splenomegaly workup
A clean, professional medical diagnostic algorithm flowchart for "Massive Splenomegaly Workup" on a white background with dark navy and teal color scheme. The flowchart flows top to bottom with the following structure: TOP BOX (dark navy, white text): "MASSIVE SPLENOMEGALY (>15 cm)" with subtitle "Leukopenia + Thrombocytopenia = Hypersplenism" STEP 1 BOX (teal): "STEP 1: HISTORY & PHYSICAL EXAM" Four sub-boxes in a row below it: - "Travel to endemic area? (tropics, subtropics)" - "B symptoms? (fever, night sweats, weight loss)" - "Liver disease stigmata? (jaundice, ascites, spider nevi)" - "Joint disease / autoimmune features?" STEP 2 BOX (teal): "STEP 2: FIRST-LINE INVESTIGATIONS (Simultaneously)" Two columns: LEFT column (Blood Tests): - CBC with differential (confirm pancytopenia) - Peripheral blood smear (parasites, teardrop cells, blasts) - LFTs + coagulation profile - LDH + uric acid - ESR / CRP RIGHT column (Microbiology/Serology): - Thick & thin blood film x3 (Malaria) - Leishmania rK39 antigen / PCR - Schistosomal serology / stool O&P - HIV / EBV / CMV serology - Blood cultures (TB, Brucella, Typhoid) STEP 3 BOX (teal): "STEP 3: TARGETED WORKUP BASED ON CLUES" Four branch boxes (with arrows) based on smear findings: 1. Arrow labeled "Eosinophilia" → "Parasitic workup: Schistosomiasis serology, Stool O&P, Leishmania PCR, Tropical screen" 2. Arrow labeled "Teardrop cells + leukoerythroblastic" → "Myeloproliferative: JAK2, BCR-ABL, Bone marrow biopsy" 3. Arrow labeled "Lymphocytosis / Blasts" → "Haematological malignancy: Flow cytometry, CT chest/abdomen/pelvis, Bone marrow biopsy" 4. Arrow labeled "Liver disease signs" → "Portal HTN workup: Hepatitis B/C serology, Liver biopsy, Upper GI endoscopy" STEP 4 BOX (teal): "STEP 4: BONE MARROW BIOPSY / ASPIRATE" Text: "If diagnosis remains unclear after Steps 1-3 | Look for: Leishmania amastigotes, Myelofibrosis, Infiltrative disease, Malignancy" BOTTOM BOX (dark navy, white text): "MANAGEMENT PRINCIPLE" Text: "Treat underlying cause first | Hypersplenism resolves with treatment of primary disease | Splenectomy only if hypersplenism is sole driver and cause is corrected" Use clean directional arrows between all steps. Professional clinical flowchart style suitable for a medical textbook.
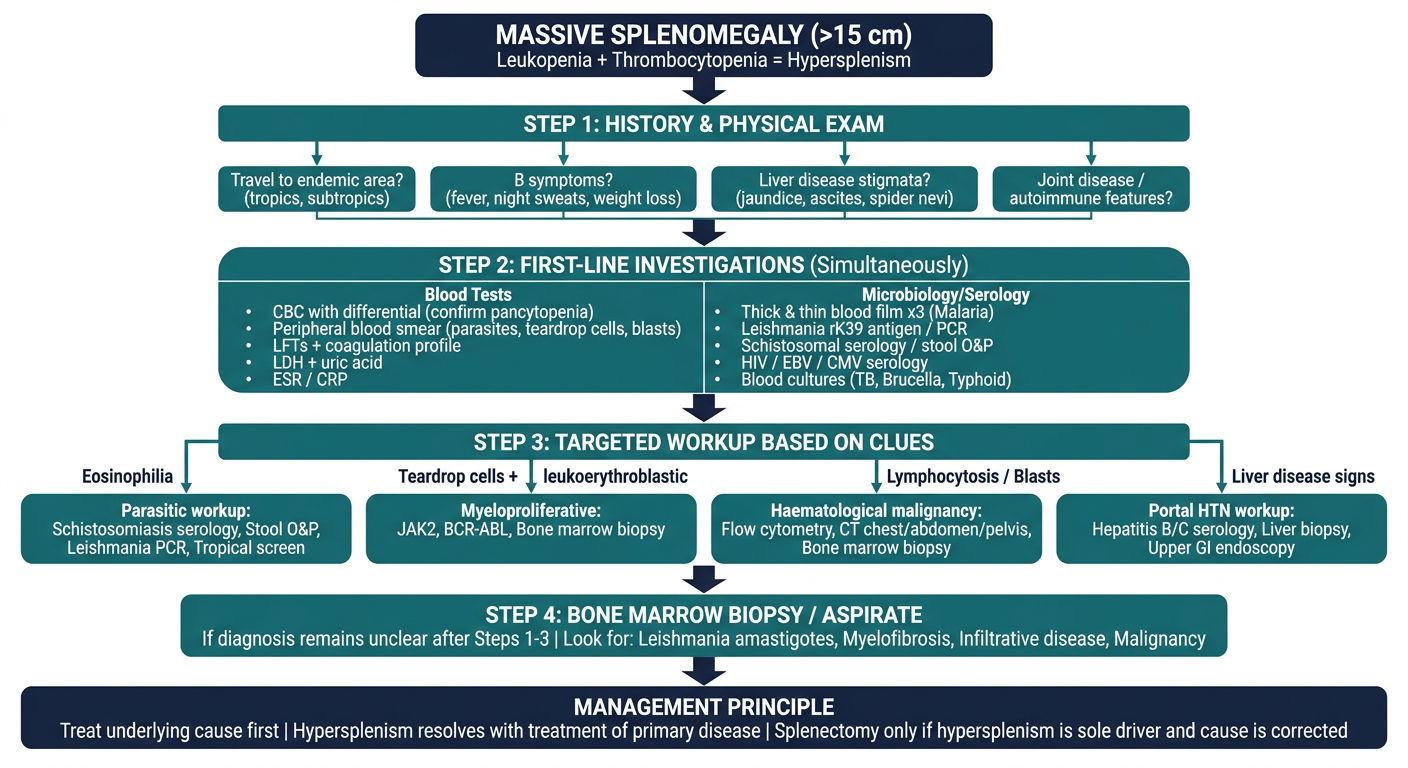
Step 1 - History & Exam (Before any tests)
- Travel history - tropical/subtropical → parasitic etiology first
- B symptoms (fever, weight loss, night sweats) → lymphoma or infectious
- Liver disease stigmata → portal hypertension / congestive splenomegaly
- Joint/autoimmune features → Felty syndrome, SLE
Step 2 - First-line investigations (all simultaneously)
Step 3 - Smear-guided branching
| Smear Finding | Pathway |
|---|---|
| Eosinophilia | Tropical/parasitic screen |
| Teardrop cells + leukoerythroblastic picture | Myeloproliferative (JAK2, BCR-ABL) |
| Lymphocytosis / blasts | Haematological malignancy |
| Normal smear + liver disease signs | Portal hypertension workup |
Step 4 - Bone marrow biopsy
Key principle
- Frameworks for Internal Medicine, p. 366-367
- Harrison's Principles of Internal Medicine 22E, p. 2758