Pain in the head
Reading File
Asking for Preferences
Asking for Preferences
Finding Sources
Finding Sources
Searching PubMed
"migraine"[MeSH Terms] AND "treatment"[MeSH Terms]
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is the full treatment guide for migraine:
Migraine Treatment & Management
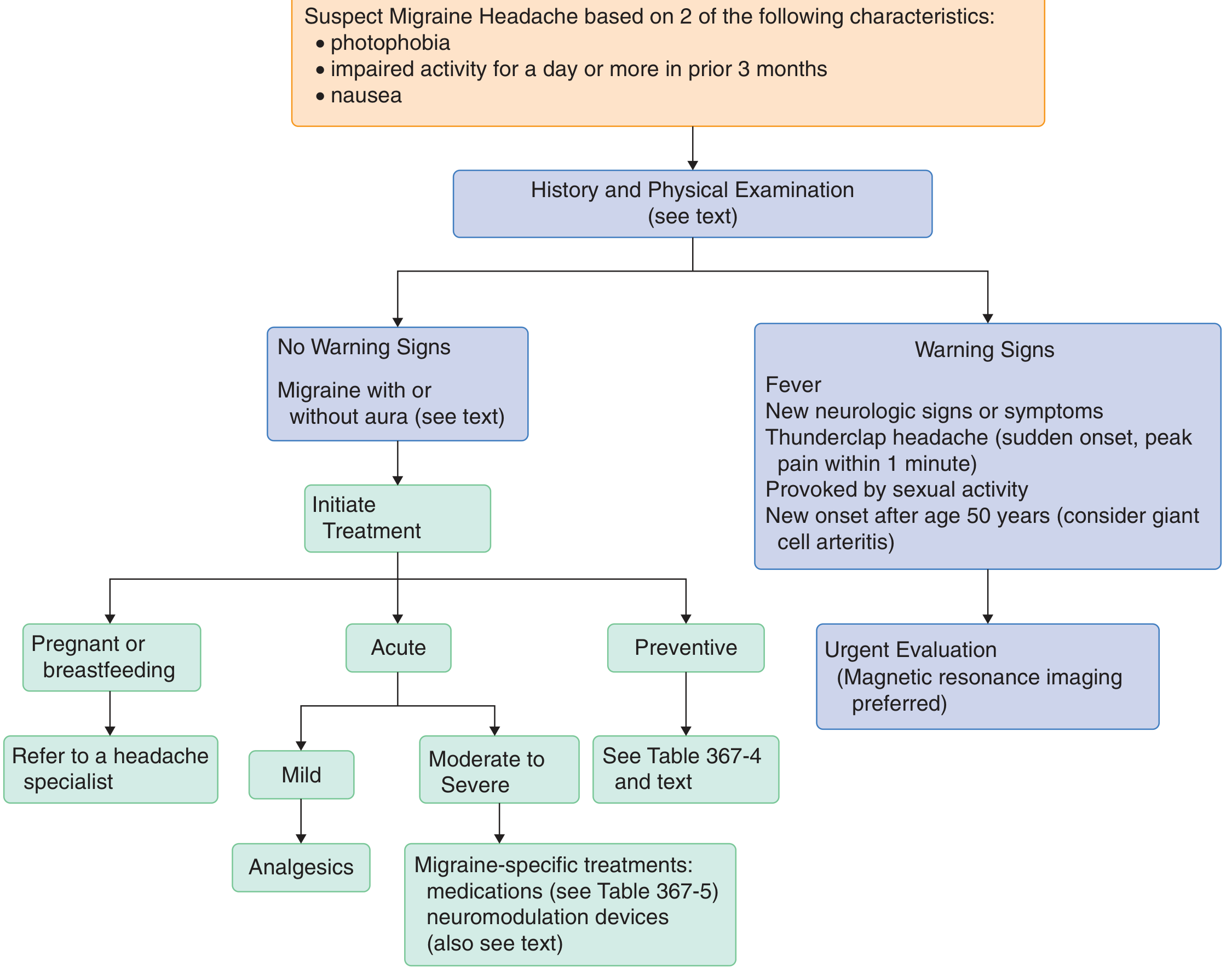
First: Suspect Migraine If 2 of These Are Present
- Photophobia
- Nausea
- Impaired activity for a day or more in the prior 3 months
If warning signs are present (fever, new neurologic signs, thunderclap headache, onset after age 50, headache triggered by sexual activity), stop and arrange urgent MRI evaluation before treating as migraine.
Acute (Symptomatic) Treatment
Treatment should begin as early as possible - ideally during the aura if one is recognized, not after pain starts. Prompt treatment significantly improves outcomes.
Mild Attacks - Non-Specific Analgesics
| Drug | Dose |
|---|---|
| Acetaminophen | 650-1000 mg |
| Aspirin | 250-1000 mg |
| Ibuprofen | 400-600 mg |
| Naproxen | 500-825 mg |
| Diclofenac | 50 mg |
- Caffeine added to analgesics aids absorption, induces vasoconstriction, and reduces serotonergic brainstem firing
- Rest in a dark, quiet room with an ice pack can augment relief
- Isometheptene mucate combinations (with acetaminophen + dichloralphenazone) are well-tolerated and do not worsen nausea
Moderate to Severe Attacks - Migraine-Specific Drugs
1. Triptans (5-HT1B/1D agonists) - First-Line
Effective in ~70% of patients. They work by causing vasoconstriction and blocking release of proinflammatory neuropeptides (substance P, CGRP) from the trigeminal system.
| Triptan | Oral Dose | Notes |
|---|---|---|
| Sumatriptan | 25-100 mg | Prototype; also SC (6 mg) and intranasal (20 mg) available |
| Rizatriptan | 5-10 mg | Faster onset |
| Eletriptan | 20-40 mg | Good oral efficacy |
| Almotriptan | 12.5 mg | |
| Zolmitriptan | 2.5-5 mg | Oral or nasal spray |
| Naratriptan | 1-2.5 mg | Slower onset, longer duration |
| Frovatriptan | 2.5 mg | Longest half-life (>24 h) - good for menstrual migraine |
- Subcutaneous sumatriptan: onset ~20 minutes; oral: 1-2 hours
- If headache recurs within 24-48 hours, a second dose is usually effective
- Try more than one triptan before concluding failure - individual response varies
- Contraindications: uncontrolled hypertension, ischemic heart disease, Prinzmetal angina, significant CAD risk factors (requires cardiac evaluation first)
2. Ergot Alkaloids
- Dihydroergotamine (DHE): 1-2 mg intranasally or 1 mg SC/IV; effective for severe attacks; requires an antiemetic (e.g., promethazine 25 mg) before IV use
- Ergotamine tartrate: 2 mg sublingually or 1-2 mg orally - useful early in an attack; watch for nausea and peripheral vasoconstriction
3. Lasmiditan (Ditan - 5-HT1F agonist)
- 50-200 mg orally
- Does not cause vasoconstriction - safe for patients with cardiovascular contraindications to triptans
- Important: sedating - no driving for at least 90 minutes (possibly up to 8 hours) after use
4. CGRP Receptor Antagonists (Gepants)
- Rimegepant: 75 mg orally
- Ubrogepant: 50-100 mg orally
- Provide ~10% absolute increase in 2-hour pain freedom vs. placebo; minimal side effects; no vasoconstriction
Very Severe / Refractory Attacks (Clinic/ER Setting)
- DHE 1 mg SC or 0.5-1 mg IV (with antiemetic)
- Ketorolac: 60 mg IM or 30 mg IV
- Prochlorperazine: 10-25 mg IM or 10 mg IV (over 5 minutes)
- Metoclopramide: 10 mg IV
- Opioids: last resort only - risk of medication-overuse headache with chronic use; meperidine is not effective
Noninvasive Neuromodulation (Newer Approaches)
FDA-approved devices include:
- Transcranial magnetic stimulation
- Vagus nerve stimulation
- Trigeminal nerve stimulation
- Remote electrical neuromodulation (smartphone-controlled)
Avoid in patients with cardiac pacemakers.
Preventive (Prophylactic) Treatment
When to start prevention: Headaches interfering with activities on 3+ days/month, or when headaches are severe, prolonged, or not responding to acute therapy. Generally consider if attacks occur 1-2 days/week.
First-Line Preventive Agents
| Class | Drug | Notes |
|---|---|---|
| Beta-blockers | Propranolol, metoprolol | Well established |
| Tricyclic antidepressants | Amitriptyline | Especially useful with comorbid depression/insomnia |
| Anticonvulsants | Valproate, Topiramate | Effective; teratogenic risk with valproate |
| Calcium channel blockers | Verapamil | Useful, especially cluster overlap |
| NSAIDs | Naproxen | Short-term menstrual migraine prevention |
CGRP Antibodies (Monoclonal - Newer Biologics)
| Drug | Dose |
|---|---|
| Erenumab | 70-140 mg SC monthly |
| Fremanezumab | 225 mg SC monthly OR 675 mg quarterly |
| Eptinezumab | 100-300 mg IV every 12 weeks |
| Galcanezumab | 240 mg loading, then 120 mg SC monthly |
Small-Molecule CGRP Inhibitors (Oral Preventives)
- Rimegepant: 75 mg orally every other day
- Atogepant: 10-60 mg orally once daily
Other Preventive Options
- OnabotulinumtoxinA (Botox): FDA-approved for chronic migraine (15+ headache days/month)
- Cyproheptadine: 4-20 mg (especially useful in children)
- Phenelzine (MAO inhibitor): 30-60 mg - reserved for refractory cases
- Acupuncture and biofeedback: evidence supports both
Lifestyle & Non-Pharmacological Measures
- Maintain regular sleep, meals, and hydration
- Avoid known triggers: nitrites (processed meats), MSG, tyramine-rich foods (aged cheese, red wine, chocolate), strong smells
- Omega-3-rich / low omega-6 diet may reduce attack frequency
- Stress management: cognitive behavioral therapy, relaxation training, biofeedback, hypnosis
Special Populations
- Pregnant patients: Acetaminophen is first-line; isometheptene + dichloralphenazone combination for moderate attacks; metoclopramide + diphenhydramine for nausea (superior to codeine); noninvasive neuromodulation is especially attractive
- Triptans and ergotamines are generally avoided in pregnancy
Key Principle: Avoid Medication Overuse
Frequent use of analgesics (especially opioids, but also triptans and NSAIDs) can cause medication overuse headache (MOH) - a chronic daily headache pattern. Patients must be counseled on frequency limits for acute treatments.
Sources: Goldman-Cecil Medicine, p. 3815 | Bradley and Daroff's Neurology in Clinical Practice, p. 2479 | Lippincott Illustrated Reviews Pharmacology, p. 1322 | Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.