Using millers, morgan and barasch anaesthesiology books teach me from basic to advance about - Exercise stress tests and cardio pulmonary exercise tests
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have comprehensive content from all three textbooks. Let me compile the complete, structured teaching answer.
Exercise Stress Tests (EST) and Cardiopulmonary Exercise Tests (CPET)
A Comprehensive Teaching Guide from Miller's Anesthesia (10e), Barash Clinical Anesthesia (9e), and Morgan & Mikhail's Clinical Anesthesiology (7e)
PART 1 - FOUNDATIONS: Why We Test Exercise Capacity
The Core Concept: Functional Capacity and METs
Before any test is ordered, the anesthesiologist must understand what is being measured. Functional capacity is the body's ability to meet the metabolic demands of physical activity. It is expressed in metabolic equivalents of task (METs), where 1 MET = resting oxygen consumption = 3.5 mL/kg/min.
| MET Level | Activity Examples | Clinical Meaning |
|---|---|---|
| 1 MET | Sitting quietly | Baseline |
| 2-3 METs | Walking slowly on level ground | Poor capacity |
| 4 METs | Climbing one flight of stairs, light housework | Minimum threshold for most surgery |
| 5-7 METs | Cycling, dancing, doubles tennis | Moderate capacity |
| >10 METs | Swimming, singles tennis, vigorous sports | Excellent capacity |
"Functional capacity is typically quantified using the metabolic equivalent of task (MET), where one MET is approximately the rate of energy consumption at rest (3.5 mL/kg/min)."
- Miller's Anesthesia 10e, p. 3835
Why Functional Capacity Matters Perioperatively
Poor preoperative functional capacity is one of the strongest and most consistent predictors of perioperative morbidity and mortality. Miller's 10e summarizes the evidence base:
- Poor exercise capacity and cardiopulmonary disease have a bidirectional relationship: lack of exercise increases risk of cardiopulmonary disease, but existing disease also prevents exercise
- Multiple large studies showed association between difficulty performing ADLs and increased risk of postoperative mortality, cardiovascular complications, and pulmonary complications
- Only one-fifth of American adults meet federal aerobic activity guidelines - suboptimal functional capacity is the norm, not the exception
The Problem with Clinical Assessment Alone
The usual clinical approach - asking patients about activity in an unstructured interview - is unreliable. Miller's 10e (p. 3835) cites a key multicenter prospective cohort study (~1400 patients) showing:
- Anesthesiologists' subjective assessment had only 19% sensitivity and 95% specificity for identifying patients unable to attain ≥4 METs on formal exercise testing
- Subjective assessment did not meaningfully improve prediction of postoperative mortality/morbidity
This is why objective exercise testing exists.
PART 2 - EXERCISE STRESS TESTING (EST)
What is an Exercise ECG Stress Test?
The exercise ECG stress test (also called treadmill test or graded exercise test) is the most traditional, most cost-effective, and least invasive method for evaluating patients with suspected coronary artery disease (CAD).
"The exercise ECG stress test has been the traditional method for evaluating patients with suspected CAD. It represents the most cost-effective and least invasive method for detecting ischemia, with a sensitivity of 70% to 80% and a specificity of 60% to 75% for identifying CAD."
- Barash Clinical Anesthesia 9e, p. 1769
How the Test is Performed
- Patient exercises on a treadmill or stationary bike, incrementally increasing workload
- Continuous ECG monitoring throughout
- Target endpoint: achieve 85% of maximum predicted heart rate (formula: 220 minus age)
- The test is "adequate" only when this heart rate target is achieved
Indications and Patient Selection
Who should have an exercise ECG stress test? (Miller's 10e, p. 3890-3891):
- Patients capable of exercising and likely to achieve adequate heart rate response
- Patients with a relatively normal baseline ECG (no LBBB, no LVH with strain pattern)
- Provides dual information: diagnosis of IHD AND objective measurement of functional capacity
When imaging must supplement or replace ECG monitoring:
- Significant ECG abnormalities (Left Bundle Branch Block, LVH with strain) - these interfere with electrocardiographic ischemia detection
- Note: Exercise myocardial perfusion imaging can still give false positives in LBBB due to septal perfusion defects even without ischemia
When Exercise is Not Possible - Pharmacologic Stress Tests
When a patient cannot exercise or cannot achieve adequate heart rate (pacemaker, significant bradycardia, high-dose beta-blockers), pharmacologic stress modalities replace exercise:
| Agent | Mechanism | Contraindications/Cautions |
|---|---|---|
| Dobutamine | Increases contractility, HR, and BP (mimics exercise) | Pacemakers, aortic aneurysms, cerebral aneurysms, poorly controlled HTN |
| Adenosine / Dipyridamole | Coronary vasodilation (flow heterogeneity) | Theophylline (blocks effect), severe stenotic valvular disease (dangerous preload reduction) |
| Regadenoson | Coronary vasodilation | Same as adenosine/dipyridamole |
Ischemia Monitoring Methods - The Three Options
Once a stress modality is chosen, ischemia can be detected by three methods:
1. ECG - simple, non-imaging
- Detects ST-segment changes (ischemia)
- Requires normal baseline ECG
2. Stress Echocardiography (with exercise or dobutamine)
- Assesses wall motion abnormalities at rest AND under stress
- Resting abnormalities = scar from prior MI
- New inducible wall motion abnormalities = ischemia from stenotic coronaries
- Prognostic performance: positive LR 4.1, negative LR 0.2 for postoperative death/MI (meta-analysis)
- Patients at greatest risk demonstrate wall motion abnormalities at low heart rates
2. Nuclear Myocardial Perfusion Imaging (MPI) - with thallium-201, technetium-99m, or rubidium-82
- Detects ischemia by comparing radioisotope uptake at rest vs. stress
- Fixed defects at rest = prior MI
- Reversible defects = ischemia
- Prognostic: positive LR 1.8, negative LR 0.4 (slightly less accurate than echo)
- Risk is highest when reversible defects exceed >20% of the myocardium
Diagnostic Performance Summary (Miller's 10e, p. 3892-3893)
| Test | Sensitivity | Specificity | Positive LR | Negative LR |
|---|---|---|---|---|
| Exercise ECG | 70-80% | 60-75% | 2.4 | 0.4 |
| Stress Echocardiography | Higher | Higher | 4.1 | 0.2 |
| Myocardial Perfusion Imaging | Moderate | Moderate | 1.8 | 0.4 |
- A normal DSE or MPI supports a high negative predictive value for perioperative MI/cardiac death
- Moderate to large areas of ischemia = increased risk
Interpreting a Positive Stress Test
A positive exercise stress test alerts the anesthesiologist that the patient is at risk for ischemia associated with elevated heart rate (e.g., during induction, laryngoscopy, emergence). The greatest risk is in patients who develop ischemia after only mild exercise - this indicates severe, flow-limiting coronary disease at low myocardial oxygen demand.
What Follows a High-Risk Stress Test Result?
Patients with high-risk findings may progress to:
- CT Coronary Angiography (CTCA) - noninvasive, good sensitivity for detecting significant stenosis; best as a follow-up to stress testing rather than first-line
- Invasive Coronary Angiography - gold standard for diagnosing IHD; may be followed by revascularization
- Both are complementary: perioperative risk is highest in patients with both severe (≥70%) stenosis AND severe stress-induced ischemia in corresponding territories
PART 3 - PREOPERATIVE CARDIAC TESTING ALGORITHM
The ACC/AHA 2014 Framework (Barash 9e, p. 1764 + Miller's 10e)
The decision to order cardiac stress testing follows a structured algorithm:
Step 1: Evaluate urgency of surgery. If emergency, proceed without testing.
Step 2: Has the patient had recent coronary evaluation or revascularization? If yes, generally proceed.
Step 3: Identify active cardiac conditions (unstable angina, decompensated HF, severe arrhythmia, severe valvular disease). These require management before elective surgery.
Step 4: Assess surgery-specific risk (high-risk: vascular, intrathoracic, intraperitoneal). Low-risk procedures generally don't require further testing.
Step 5: Assess functional capacity. If ≥4 METs without symptoms - generally proceed without further testing.
Step 6: If <4 METs or unknown capacity AND elevated surgical risk: consider noninvasive stress testing only if the result will change management.
"Most importantly, no preoperative cardiovascular testing should be performed if the results will not change perioperative management."
- Barash 9e, p. 1764
Who Gets Pharmacologic Stress Testing? (Barash 9e)
- High-risk patients who cannot exercise or have contraindications to exercise (e.g., claudication from peripheral artery disease)
- Poor or indeterminate functional capacity (<4 METs)
- Only if results will change management
PART 4 - CARDIOPULMONARY EXERCISE TESTING (CPET)
What is CPET?
CPET is the most sophisticated and comprehensive method of assessing functional capacity. It is distinctly different from a standard exercise stress test.
"Cardiopulmonary exercise testing (CPET) is an integrated and dynamic test which evaluates patients' functional capacity and characterizes the contribution of the respiratory, cardiovascular, and musculoskeletal system in its limitation."
- Miller's Anesthesia 10e (Pulmonary section), p. 1307
What CPET Measures - The Setup
During CPET the patient undergoes brief incremental exercise (treadmill or cycle ergometer) while being continuously monitored for:
| Parameter | What it Reflects |
|---|---|
| ECG (12-lead) | Cardiac rhythm, ischemia |
| Pulse oximetry | Oxygenation |
| Respiratory rate | Ventilatory drive |
| Exhaled gases (O₂ and CO₂) | Metabolic and ventilatory coupling |
| Airflow and volume | Ventilatory mechanics |
This gives CPET a unique advantage: it simultaneously interrogates cardiac, pulmonary, and musculoskeletal systems and shows which one is the limiting factor.
The Three Key CPET Parameters
1. VO₂max (Maximal Oxygen Consumption)
Definition: The highest VO₂ value reached at maximum tolerated exercise. It is the broadest indicator of overall cardiorespiratory functional capacity.
Why it matters: Reflects the integrated delivery and utilization of oxygen across the entire cardiorespiratory chain (lungs → circulation → muscles).
Thresholds (Miller's 10e, p. 1307):
- VO₂max <15 mL/kg/min = increased risk of postoperative pulmonary complications (general surgery)
- VO₂max <10 mL/kg/min = high perioperative risk, particularly for thoracic surgery (Morgan & Mikhail 7e, p. 1039)
- VO₂max >20 mL/kg/min = not associated with significant increase in perioperative mortality or morbidity (Morgan & Mikhail 7e)
- VO₂max 10-20 mL/kg/min = intermediate/moderate risk
2. Anaerobic Threshold (AT)
Definition: The VO₂ value above which VCO₂ increases disproportionately to VO₂, because increasing anaerobic metabolism produces excess CO₂ from bicarbonate buffering of lactic acid. This is also called the ventilatory threshold or lactate threshold.
Physiological basis: When oxygen delivery becomes insufficient for cellular aerobic metabolism, cells switch to anaerobic glycolysis, producing lactic acid. The buffering of this acid by bicarbonate releases extra CO₂, causing VCO₂ to rise faster than VO₂ - this "V-slope" breakpoint is the AT.
Why it is valuable: The AT represents sustainable exercise capacity - the level below which exercise can be maintained without accumulating lactate. It is measurable even when the patient cannot reach maximal effort (submaximal test).
Threshold (Miller's 10e, p. 1307-1308):
- AT <10 mL/kg/min = increased risk for postoperative complications
3. VE/VCO₂ Slope (Ventilatory Efficiency)
Definition: The ratio of minute ventilation (VE) to CO₂ output (VCO₂). It measures the efficiency of gas exchange and reflects ventilation-perfusion (V/Q) matching and dead space ventilation.
Key point: VE/VCO₂ has been shown to predict postoperative pulmonary complications more accurately than VO₂max alone.
Threshold (Miller's 10e, p. 1308):
- VE/VCO₂ slope >35 = high-risk patients (identifies inefficient ventilation, high dead space)
CPET vs. Exercise ECG Stress Test: The Key Difference
| Feature | Exercise ECG Stress Test | CPET |
|---|---|---|
| Primary purpose | Detect myocardial ischemia | Quantify functional/cardiorespiratory capacity |
| Monitoring | ECG ± imaging | ECG + gas exchange + ventilometry |
| Key output | Ischemic ECG changes / wall motion | VO₂max, AT, VE/VCO₂ |
| System interrogated | Cardiovascular (ischemia focus) | Cardiovascular + Pulmonary + Musculoskeletal |
| Identifies limiting system | No | Yes |
| Setting | Cardiology, preop assessment | Specialized CPET lab |
PART 5 - THE "SIMPLE" EXERCISE TESTS (Stair Climbing, 6MWT)
Before ordering formal CPET, simpler exercise tests can stratify risk and decide who needs CPET.
Stair Climbing
The easiest and most clinically available test. Morgan & Mikhail 7e (p. 1039) states:
- Ability to climb 2-3 flights of stairs = decreased mortality and morbidity
- Unable to climb <2 flights = increased perioperative risk
- Standard height for "one flight" = 10 feet (3 metres)
For thoracic surgery specifically (Miller's 10e, p. 7076): "the ability to climb 2 flights of stairs without stopping is a minimum to be considered for pulmonary resection evaluation."
Six-Minute Walk Test (6MWT)
"The most valid simple exercise test is the maximal distance that a patient can walk in 6 minutes."
- Miller's Anesthesia 10e, p. 7076
- Excellent correlation with VO₂max, requires no laboratory equipment
- In COPD patients: VO₂max (mL/kg/min) = 6MWT distance (metres) ÷ 30
- Example: 6MWT of 450 m → estimated VO₂max = 450/30 = 15 mL/kg/min
- 6MWT <400 m = increased risk of postoperative cardiopulmonary complications after lobectomy
Shuttle Walk Test (SWT)
- Used in the thoracic surgery algorithm (Morgan & Mikhail algorithm, Fig. 25-10)
- SWT <400 m - triggers formal CPET
PART 6 - APPLICATION TO THORACIC SURGERY (The "Three-Legged Stool")
This is where CPET is most rigorously applied in anesthesiology practice.
The Three-Legged Stool Concept (Miller's 10e, p. 7078)
Preoperative assessment for thoracotomy must evaluate all three legs. No single test is adequate alone:
| Leg | Assessment | Most Valid Test | High-Risk Threshold |
|---|---|---|---|
| Respiratory Mechanics | Will residual lung work post-resection? | ppoFEV₁ | <30-40% predicted |
| Parenchymal Function | Gas exchange capacity | ppoDLCO | <30-40% predicted |
| Cardiopulmonary Interaction | Exercise capacity | VO₂max (CPET) | <15 mL/kg/min |
Where:
- ppoFEV₁ = predicted postoperative FEV₁ = preop FEV₁ × (1 - % functional lung removed/100)
- ppoDLCO = same calculation for diffusion capacity
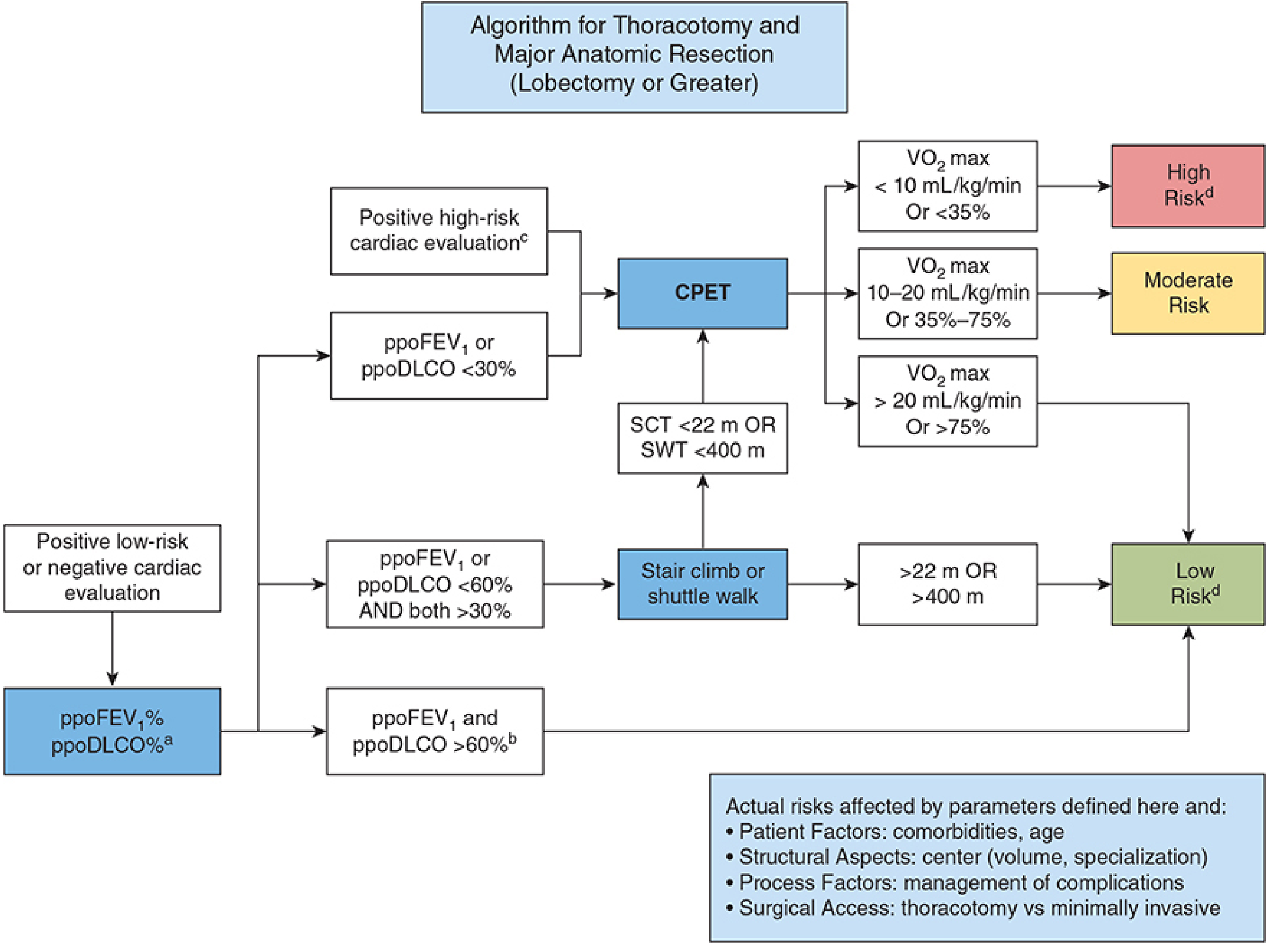
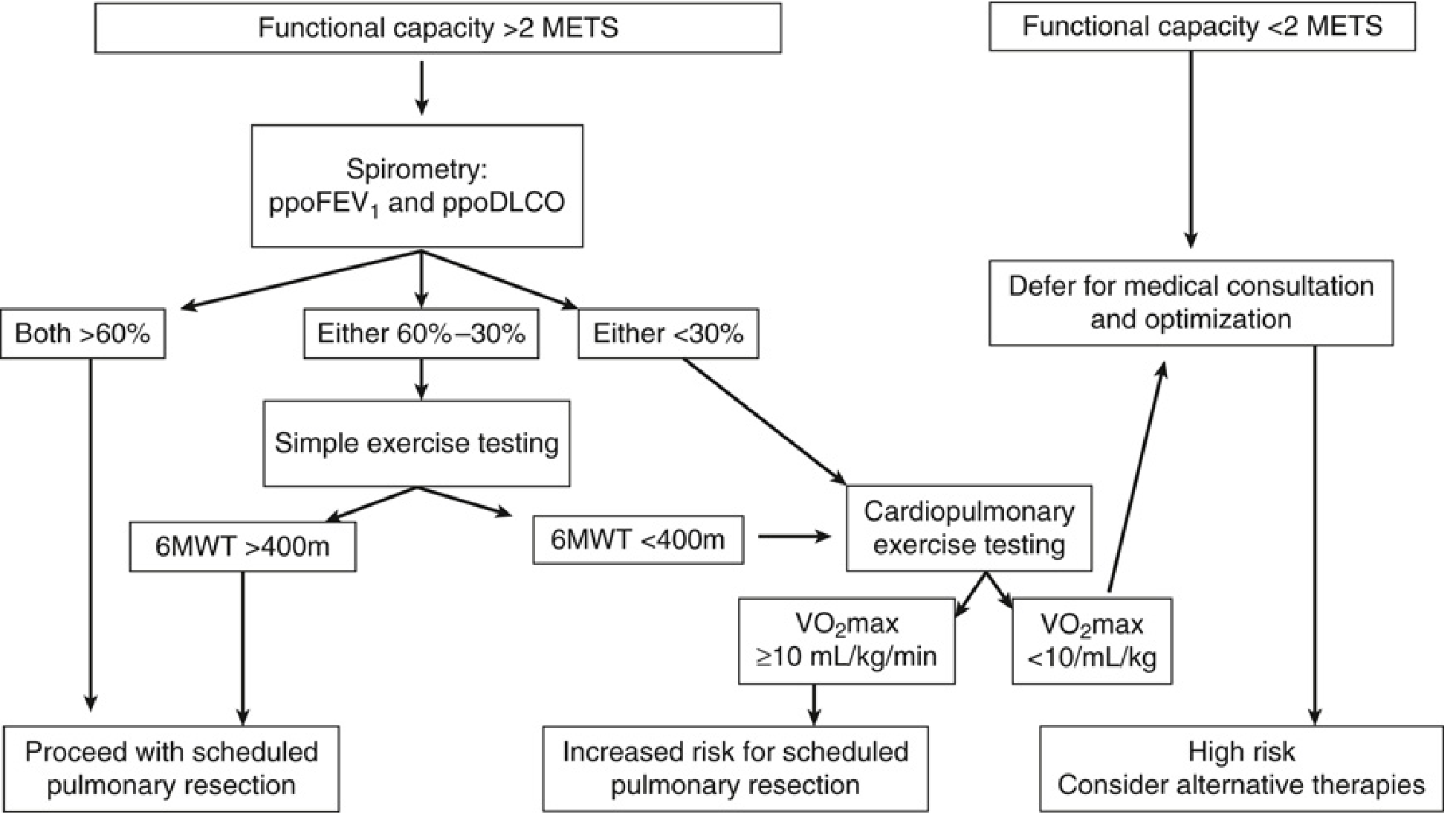
The Pre-Pulmonary Resection Algorithm
This is visualized in the flowchart from Morgan & Mikhail (Fig. 25-10) and Miller's (Fig. 49.2):
From Morgan & Mikhail 7e (p. 1038-1039):
- If ppoFEV₁ AND ppoDLCO both >60%: low risk - proceed
- If either is 60-30%: intermediate risk - perform simple exercise testing (stair climb, shuttle walk)
- If stair climb >22 m OR shuttle walk >400 m → low risk
- If below these thresholds → proceed to formal CPET
- If either is <30%: proceed directly to CPET
- If positive high-risk cardiac evaluation: proceed directly to CPET
CPET risk stratification for thoracic surgery:
- VO₂max >20 mL/kg/min (or >75% predicted) = Low Risk
- VO₂max 10-20 mL/kg/min (or 35-75% predicted) = Moderate Risk
- VO₂max <10 mL/kg/min (or <35% predicted) = High Risk - consider alternative therapies
VATS vs. Open Thoracotomy note (Miller's 10e, p. 7079): Minimally invasive techniques (VATS, robotic) have shifted risk thresholds. The ppoFEV₁ threshold for increased risk appears to have shifted from <40% for open thoracotomy to <30% for VATS.
PART 7 - VALIDATED QUESTIONNAIRES FOR FUNCTIONAL CAPACITY
When formal exercise testing is unavailable, validated questionnaires offer a standardized alternative to unstructured clinical assessment.
Duke Activity Status Index (DASI)
A validated questionnaire correlating with objective exercise capacity. Lower DASI scores are associated with increased postoperative complications.
MET-REPAIR Questionnaire
A newer validated tool specifically designed for perioperative cardiac risk assessment. Both DASI and MET-REPAIR are correlated with gold-standard measures of functional capacity (Miller's 10e, p. 3836).
Structured Interview Questions
Even without formal questionnaires, asking specific, consistent questions is superior to unstructured interviews:
- "Can you walk four blocks on level ground without stopping?" (inability = increased serious perioperative complications)
- "Can you climb two flights of stairs without stopping?" (inability = increased postoperative cardiac complications)
PART 8 - KEY NUMBERS TO REMEMBER (High-Yield Summary)
| Parameter | Threshold | Meaning |
|---|---|---|
| Functional capacity | <4 METs = poor; ≥4 METs = adequate | Guides need for cardiac stress testing |
| Exercise ECG sensitivity | 70-80% | For detecting CAD |
| Exercise ECG specificity | 60-75% | For detecting CAD |
| Stress echo positive LR | 4.1 | Better prognostic accuracy |
| 6MWT | <400 m = high risk | Triggers formal CPET (thoracic surgery) |
| Stair climb | <2 flights = high risk | Minimum for pulmonary resection consideration |
| VO₂max | <10 = high risk; 10-20 = moderate; >20 = low risk | CPET for thoracic surgery |
| VO₂max | <15 mL/kg/min | Increased postop pulmonary complications (general surgery) |
| Anaerobic Threshold | <10 mL/kg/min = increased risk | Perioperative complications |
| VE/VCO₂ | >35 = high risk | Predicts postop pulmonary complications |
| ppoFEV₁ | <30-40% = high risk (open); <30% = high risk (VATS) | Pre-thoracotomy assessment |
| ppoDLCO | <30-40% = high risk | Pre-thoracotomy gas exchange |
PART 9 - SPECIAL CONSIDERATION: The RCRI and When Testing Changes Management
The Revised Cardiac Risk Index (RCRI) assigns perioperative cardiac risk based on 6 clinical variables (Barash 9e, p. 1763):
- High-risk surgery
- History of ischemic heart disease
- History of congestive heart failure
- History of cerebrovascular disease
- Insulin-dependent diabetes
- Chronic kidney disease (creatinine >2 mg/dL)
| RCRI Score | Risk of Major Cardiac Complications |
|---|---|
| 0 | 0.4% |
| 1 | ~1% |
| 2 | ~2-3% |
| ≥3 | ~11% |
Exercise stress testing adds value on top of RCRI when it will change management. A reasonable contemporary approach (Miller's 10e) is to reserve stress testing largely for patients with high-risk results on preoperative cardiac biomarker testing (BNP/NT-proBNP, troponin).
Sources
- Miller's Anesthesia, 2-Volume Set, 10e - Chapters 28 (Preoperative Evaluation) and 49 (Thoracic Anesthesia), pp. 3834-3836, 3889-3894, 7074-7080
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e - Chapter 23 (Preoperative Assessment), pp. 1763-1769
- Morgan & Mikhail's Clinical Anesthesiology, 7e - Chapter 25 (Thoracic Anesthesia / Pulmonary section), pp. 1038-1040
This is a shared conversation. Sign in to Orris to start your own chat.