10 mark answer for anatomical dead space and its relevance in anaesthesia
Reading File
Finding Sources
Finding Sources
Searching the Web
anatomical dead space anaesthesia significance respiratory physiology
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive content from multiple authoritative sources. Let me compose the full 10-mark answer.
Anatomical Dead Space and Its Relevance in Anaesthesia
Definition
Anatomical dead space (VDanat) refers to the volume of gas occupying the conducting airways - the nose, mouth, pharynx, larynx, trachea, bronchi, and bronchioles down to the terminal bronchioles - that does NOT participate in gas exchange. In healthy young adult males, this approximates 150 mL (~2.2 mL/kg body weight), and is slightly less in females due to smaller airway dimensions. It constitutes roughly 30% of a normal tidal volume of 500 mL.
- Guyton and Hall Textbook of Medical Physiology, p.499
- Barash Clinical Anesthesia 9e, p.1126
Types of Dead Space
| Type | Definition | Normal Value |
|---|---|---|
| Anatomical dead space | Volume of conducting airways | ~150 mL |
| Alveolar dead space | Ventilated alveoli with absent/reduced perfusion | ~0 mL in healthy lungs |
| Physiological dead space | Anatomical + alveolar dead space | ~150 mL (healthy); can be ≥1-2 L in disease |
| Apparatus dead space | Dead volume added by anaesthetic equipment (mask, ETT connectors, HME filters, Y-piece) | Variable |
Physiological dead space = Anatomical dead space + Alveolar dead space
- Guyton and Hall, p.499
- Barash Clinical Anesthesia 9e, p.1126
Measurement
1. Fowler's Single-Breath Nitrogen Washout Method (Anatomical Dead Space)
The subject breathes in a single breath of 100% O2 after equilibration on room air (alveolar N2 75%). On expiration, the first gas exhaled (phase I) has zero N2~ (from conducting airways). A sharp rise then occurs (phase II) followed by a plateau (phase III = alveolar gas). By drawing a vertical line through the S-shaped curve such that areas above and below are equal:
VD= (Gray area / [Gray + Pink area]) × VE
Example: If gray area = 30 cm², pink area = 70 cm², VE = 500 mL → VD = (30/100) × 500 = 150 mL
- Guyton and Hall, p.498-499
2. Bohr / Enghoff Equation (Physiological Dead Space)
The Enghoff modification of the Bohr equation is the standard clinical method:
VD/VT= (PaCO2- PeCO2) / PaCO2
Where PaCO2 = arterial CO2 partial pressure and PeCO2 = mixed expired CO2 partial pressure.
- Normal V
D/VTratio: ~0.33 in spontaneous breathing; up to 0.5 during positive-pressure ventilation - Barash Clinical Anesthesia 9e, p.1126
Effect on Alveolar Ventilation
Alveolar ventilation (V̇A) - the volume of fresh gas reaching alveoli per minute - is the clinically relevant quantity, not minute ventilation:
V̇A= Respiratory Rate × (VT− VD)
With VT = 500 mL, VD = 150 mL, Rate = 12 breaths/min:
V̇A = 12 × (500 − 150) = 4200 mL/min
Any increase in dead space without a compensatory increase in tidal volume or respiratory rate directly reduces alveolar ventilation, causing hypercapnia and hypoxaemia. This is a cornerstone concept in anaesthetic respiratory management.
- Guyton and Hall, p.499-500
- Miller's Anesthesia 10e, p.1239
Factors Affecting Anatomical Dead Space in Anaesthesia
| Factor | Effect on Dead Space | Mechanism |
|---|---|---|
| Endotracheal intubation | Decreases (~75 mL saved) | Bypasses upper airway (nose, pharynx, larynx) |
| Tracheostomy | Decreases significantly | Bypasses upper airways; important in children |
| Face mask / LMA | Increases | Adds apparatus dead space |
| HME (heat-moisture exchangers) | Increases | Can add >60 mL apparatus dead space |
| Supine/prone positioning | Slight decrease | Gravity reduces FRC, changes airway geometry |
| Neck extension | Increases (10-15 mL) | Lengthens pharyngeal space |
| Inhalational agents (e.g., isoflurane) | Increases | Bronchodilation enlarges conducting airway volume |
| Low tidal volume ventilation | Apparent increase | Reduced penetration into alveolar zone, more mixing in conducting airways |
| Positive-pressure ventilation (IPPV) | Alveolar dead space increases | V/Q mismatch, reduced cardiac output |
- StatPearls - Anatomy, Anatomic Dead Space (NCBI)
- Morgan & Mikhail Clinical Anaesthesiology 7e, p.98
Relevance in Anaesthesia Practice
1. Circuit Design and Apparatus Dead Space
In a circle system, apparatus dead space is limited to the area distal to the Y-piece (where fresh and expired gases meet), regardless of corrugated tube length. In Mapleson circuits, the tube length does NOT add to dead space but affects compliance. Minimising apparatus dead space is critical in paediatric anaesthesia where the ratio of apparatus dead space to tidal volume is proportionally much larger. Some paediatric masks have specially designed shapes to reduce apparatus dead space.
- Morgan & Mikhail, p.98
2. Endotracheal Intubation
Inserting an ETT bypasses the upper airway, reducing anatomical dead space by approximately 70-75 mL. This is beneficial and partially compensates for any apparatus dead space from the breathing circuit. However, the ETT connector and humidifier (HME) can add back 30-60 mL or more of apparatus dead space. This is especially significant in neonates and small infants.
3. PaCO2 - EtCO2 Gradient (Capnography)
In healthy individuals, end-tidal CO2 (EtCO2) closely approximates PaCO2, with a gradient of 2-5 mmHg. Anatomical dead space dilutes alveolar gas with CO2~-free conducting airway gas, which is why PeCO2 is always less than PaCO2. An increased PaCO2 - EtCO2 gradient signals increased physiological dead space (e.g. pulmonary embolism, reduced cardiac output, PEEP-induced overdistension).
4. Volume Capnography
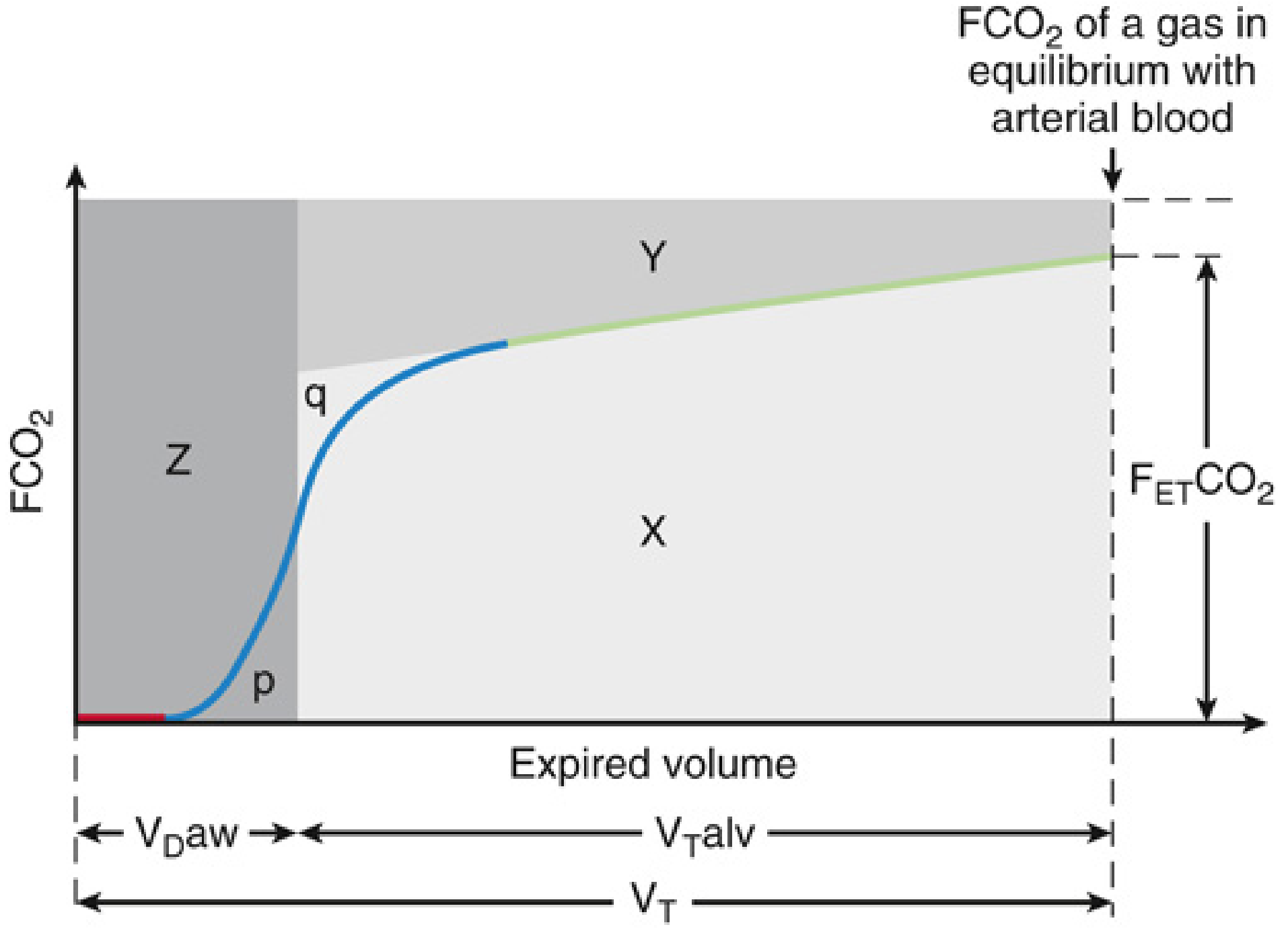
The volume capnogram (FCO2 vs. expired volume) has three phases:
- Phase I (Zone Z): CO
2-free gas - anatomical dead space - Phase II: Rising CO
2- mixed gas (transitional zone) - Phase III (Zone X): Plateau - pure alveolar gas
Area Z = wasted ventilation from anatomical dead space; Area Y = wasted ventilation from alveolar dead space. Together (Y+Z) = total physiological dead space. This allows non-invasive, breath-by-breath dead space monitoring.
- Miller's Anesthesia 10e, p.5498-5500
5. Ventilator Settings
During IPPV, the anaesthetist must account for dead space when setting tidal volume and rate:
- V
D/VTcan reach 0.5 in mechanically ventilated patients - Low tidal volume ventilation (lung-protective strategies) can increase the proportion of each breath wasted as dead space, requiring an increased respiratory rate to maintain adequate alveolar ventilation and normocapnia
- High PEEP and pulmonary hypoperfusion increase alveolar dead space - tracked by V
D/VTratio
6. Tracheostomy
One of the indications for tracheostomy is reduction of anatomical dead space, particularly relevant in patients with borderline ventilatory reserve, neuromuscular disease, or those being weaned from mechanical ventilation. The reduction (up to 50% of anatomical dead space) can substantially reduce the work of breathing.
- Scott-Brown's Otorhinolaryngology, p.5441
7. Clinical Conditions Relevant to Anaesthesia
| Condition | Dead Space Effect | Clinical Implication |
|---|---|---|
| Pulmonary embolism | Increases alveolar dead space | Sudden fall in EtCO |
| ARDS | Increased V | Prognostic marker; V |
| Cardiac arrest | Massive increase in dead space | Complete loss of EtCO |
| COPD | Increased anatomical and alveolar dead space | Higher minute ventilation requirements |
| One-lung ventilation | Increases alveolar dead space | Careful V |
Summary
Anatomical dead space is a fixed but modifiable component of every breath that represents wasted ventilation. In anaesthesia, it is relevant in:
- Circuit and equipment design - minimising apparatus dead space
- ETT and tracheostomy - both reduce anatomical dead space
- Ventilator management - setting appropriate V
Tand RR, especially in lung-protective ventilation - Capnographic monitoring - interpreting EtCO
2and VD/VTratio - Paediatric anaesthesia - proportionally higher impact of apparatus dead space
- Detecting intraoperative emergencies - PE, cardiac arrest, circuit disconnection
Understanding dead space is fundamental to optimising gas exchange, interpreting capnographic waveforms, and safe ventilator management in every anaesthetic.
Key references used:
- Guyton & Hall Textbook of Medical Physiology (p.498-500)
- Barash Clinical Anesthesia 9e (p.1126)
- Miller's Anesthesia 10e (p.5498-5500, p.1238-1240)
- Morgan & Mikhail Clinical Anaesthesiology 7e (p.98)
- StatPearls - Anatomy, Anatomic Dead Space
This is a shared conversation. Sign in to Orris to start your own chat.