Explain 10 ecg changes with pictures
Reading File
Finding Sources
Searching Images
ECG electrocardiogram changes patterns
Finding Sources
Searching Images
ST elevation myocardial infarction STEMI ECG
Searching Images
atrial fibrillation ECG irregularly irregular rhythm
Searching Images
ventricular fibrillation tachycardia ECG wide complex
Searching Images
heart block complete AV block third degree ECG
Searching Images
prolonged QT interval ECG Wolff-Parkinson-White delta wave
Searching Images
left bundle branch block right bundle branch block ECG
Searching Images
hyperkalemia peaked T waves ECG electrolyte changes
Searching Images
pericarditis diffuse ST elevation saddle-shaped ECG
Searching Images
left ventricular hypertrophy Sokolow-Lyon ECG criteria voltage
Here are 10 key ECG changes explained with images:
1. ST-Elevation Myocardial Infarction (STEMI)

What it is: Acute transmural myocardial injury causing convex (tombstone) ST-segment elevation ≥1 mm in ≥2 contiguous leads (≥2 mm in V1–V3).
ECG features:
- Convex/tombstone ST elevation in the territory of the occluded artery
- Reciprocal ST depression in opposing leads (e.g., inferior STEMI → ST depression in aVL)
- Hyperacute T waves early on; pathological Q waves develop later (indicating necrosis)
- Lead localization: Anterior (V1–V4) = LAD; Inferior (II, III, aVF) = RCA; Lateral (I, aVL, V5–V6) = LCx
2. Atrial Fibrillation (AF)
What it is: Chaotic, disorganized atrial electrical activity with irregular ventricular conduction. The most common sustained cardiac arrhythmia.
ECG features:
- Absent P waves — replaced by fine fibrillatory (f) waves, best seen in V1 and lead II
- Irregularly irregular R-R intervals — the hallmark
- Narrow QRS (unless aberrant conduction or bundle branch block co-exists)
- Rate can be slow, normal, or rapid depending on AV nodal conduction
3. Complete (Third-Degree) AV Block

What it is: Total failure of conduction through the AV node — the atria and ventricles beat completely independently.
ECG features:
- AV dissociation — P waves and QRS complexes march through each other with no fixed PR relationship
- Regular P-P intervals (faster atrial rate) and regular R-R intervals (slower escape rate)
- Wide QRS (>120 ms) if escape focus is ventricular; narrow QRS if junctional escape
- Requires urgent pacemaker implantation
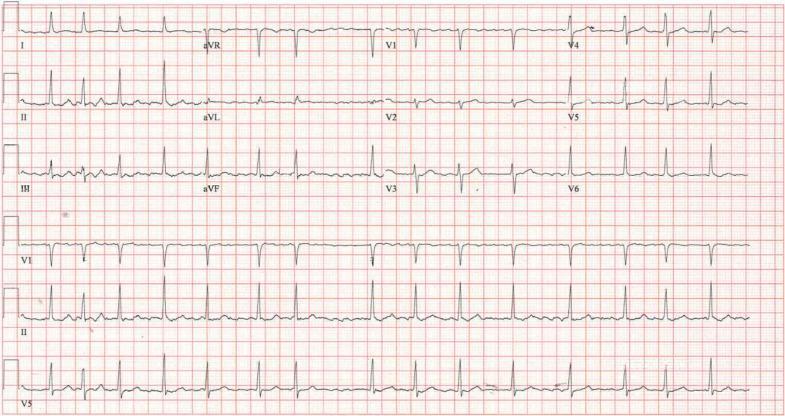
4. Wolff-Parkinson-White (WPW) Syndrome
What it is: An accessory pathway (Bundle of Kent) bypasses the AV node, causing ventricular pre-excitation.
ECG features (classic triad):
- Short PR interval (<120 ms) — conduction bypasses the AV node delay
- Delta wave — slurred upstroke at the start of the QRS complex
- Wide QRS (>120 ms) — fusion of normal + accessory pathway conduction
- Secondary ST-T changes discordant to QRS direction
- Can precipitate life-threatening AF with rapid ventricular response
5. Left Bundle Branch Block (LBBB)
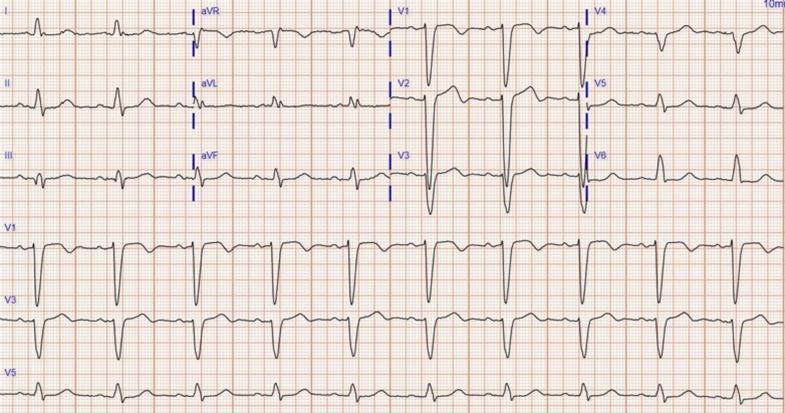
What it is: Failure of the left bundle branch causes abnormal, slow left ventricular depolarization via cell-to-cell spread.
ECG features (WiLLiaM):
- Wide QRS (≥120 ms)
- Dominant R wave (broad, monophasic, notched) in lateral leads I, aVL, V5–V6
- QS or rS complex in V1 (predominantly negative)
- Discordant ST-T changes — ST and T wave point opposite to QRS direction
- New LBBB + chest pain = presumed STEMI equivalent (Sgarbossa criteria apply)
6. Right Bundle Branch Block (RBBB)
What it is: Failure of the right bundle branch delays right ventricular depolarization.
ECG features (RaBBiT):
- Wide QRS (≥120 ms)
- rSR' ("rabbit ears") pattern in V1 — the classic finding
- Wide, slurred S waves in I, aVL, V5–V6
- T-wave inversion in V1–V3 (secondary repolarization change)
- Can be a normal variant or indicate pulmonary embolism, RV strain, or cardiac disease
7. Torsades de Pointes (Polymorphic VT)
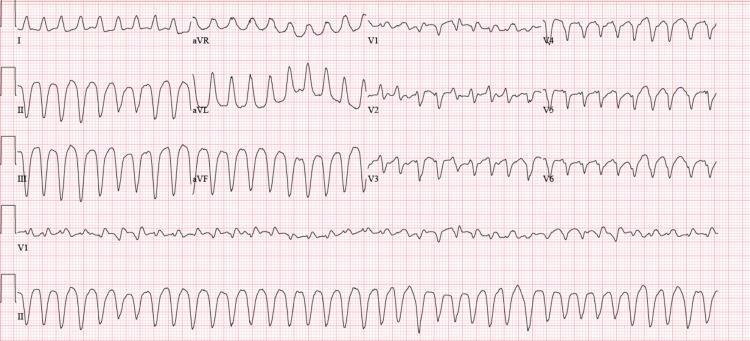
What it is: A potentially lethal polymorphic ventricular tachycardia associated with prolonged QT interval. The QRS complexes appear to "twist" around the isoelectric baseline.
ECG features:
- Wide, rapidly changing QRS morphology — amplitude and axis shift cyclically
- "Twisting of the points" — complexes appear to rotate around the baseline
- Often initiated by a "short-long-short" RR interval sequence
- Triggered by QT-prolonging drugs, electrolyte disturbances (hypokalemia, hypomagnesemia)
- Can degenerate into ventricular fibrillation → cardiac arrest
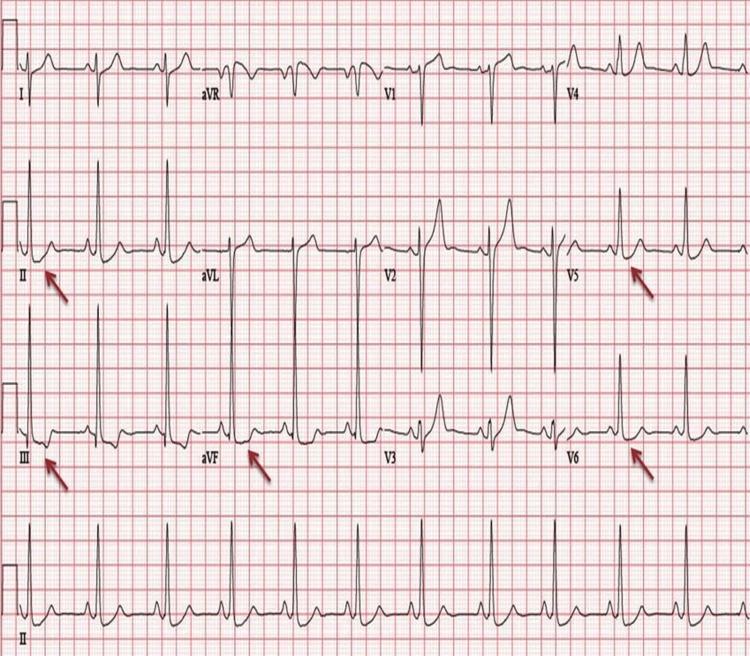
8. Hyperkalemia

What it is: Elevated serum potassium (K⁺ >5.5 mEq/L) progressively disrupts cardiac membrane potential.
ECG changes are sequential with rising K⁺:
| K⁺ Level | ECG Change |
|---|---|
| 5.5–6.5 | Tall, peaked ("tented") T waves — narrow base, symmetric |
| 6.5–7.5 | PR prolongation + P wave flattening/loss |
| 7.5–9.0 | QRS widening → sine wave pattern |
| >9.0 | Ventricular fibrillation / asystole |
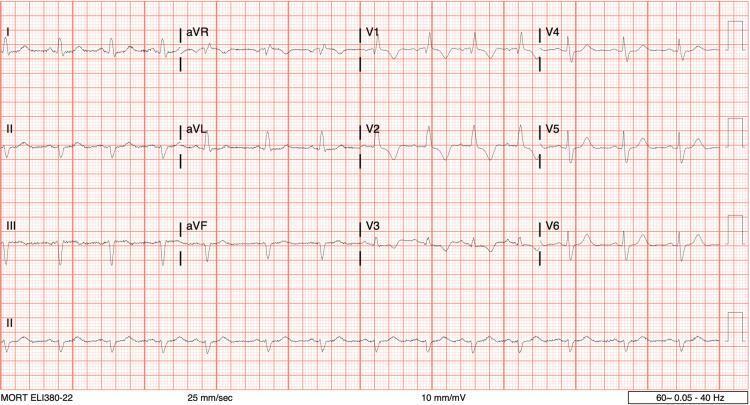
9. Acute Pericarditis

What it is: Inflammation of the pericardium causing diffuse myocardial epicardial irritation.
ECG features (4 stages):
- Stage 1 (acute): Diffuse concave ("saddle-shaped") ST elevation in nearly all leads (except aVR and V1) + PR depression (pathognomonic) + PR elevation in aVR
- Spodick's sign: Downsloping TP segment
- Stage 2: ST normalizes, T waves flatten
- Stage 3: T wave inversion
- Stage 4: ECG returns to normal
- Key distinction from STEMI: diffuse (not territorial), concave morphology, PR depression, no reciprocal ST changes
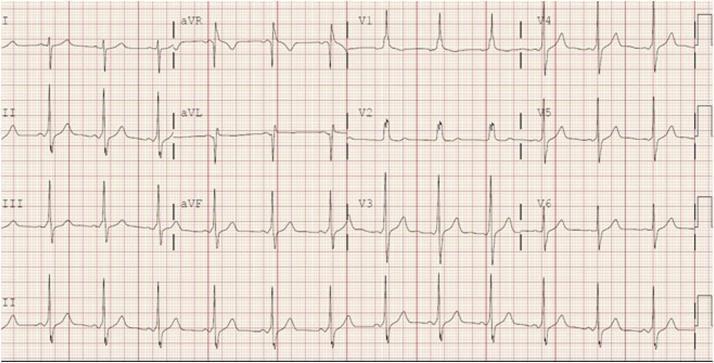
10. Left Ventricular Hypertrophy (LVH)
What it is: Increased LV muscle mass (from hypertension, aortic stenosis, HCM) generates exaggerated electrical voltages.
ECG features:
- Sokolow-Lyon criteria: S in V1 + R in V5 or V6 ≥35 mm
- Cornell criteria: R in aVL + S in V3 >28 mm (men) or >20 mm (women)
- "Strain pattern": ST depression + T-wave inversion in lateral leads (I, aVL, V5–V6) — indicates pressure/volume overload
- Left axis deviation
- Broad, notched P wave (P mitrale) if left atrial enlargement coexists
Quick Reference Summary
| # | ECG Change | Key Finding |
|---|---|---|
| 1 | STEMI | Convex ST elevation, reciprocal depression, Q waves |
| 2 | Atrial Fibrillation | Absent P waves, irregularly irregular |
| 3 | Complete Heart Block | AV dissociation, P & QRS independent |
| 4 | WPW | Short PR, delta wave, wide QRS |
| 5 | LBBB | Wide QRS, monophasic R in V5–V6, QS in V1 |
| 6 | RBBB | rSR' in V1, wide S in I/V6 |
| 7 | Torsades de Pointes | Twisting polymorphic VT, long QT |
| 8 | Hyperkalemia | Peaked T waves → wide QRS → sine wave |
| 9 | Acute Pericarditis | Diffuse saddle ST elevation, PR depression |
| 10 | LVH | High voltage, lateral strain pattern |
This is a shared conversation. Sign in to Orris to start your own chat.