What is hypertension which class of drugs are used as primary treatment in hypertension Which combination of drugs should be avoided concordantly in hypertension What is hypertensive emergency Write step wise management and mechanism of the above condition In which type of hypertension arteriolar dialotors are used and why
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching PubMed
hypertension management antihypertensive therapy guidelines
I now have all the material needed for a comprehensive, well-referenced answer. Let me compile it.
Hypertension: Complete Clinical Review
1. What is Hypertension?
Hypertension is diagnosed when systolic blood pressure (SBP) exceeds 130 mm Hg or diastolic blood pressure (DBP) exceeds 80 mm Hg (ACC/AHA 2017 guideline). It is a chronic condition driven by increased cardiac output and/or increased systemic vascular resistance.
Classification (ACC/AHA 2017):
| Stage | SBP (mm Hg) | DBP (mm Hg) |
|---|---|---|
| Elevated (prehypertension) | 120-129 | < 80 |
| Stage 1 | 130-139 | 80-89 |
| Stage 2 | ≥ 140 | ≥ 90 |
| Hypertensive crisis | > 180 | > 120 |
Types:
- Primary (essential) hypertension - no identifiable cause; accounts for ~90-95% of cases
- Secondary hypertension - identifiable cause (renal artery stenosis, pheochromocytoma, primary aldosteronism, etc.). Suspect secondary causes if hypertension develops after age 50 or is resistant to treatment.
2. Drug Classes Used as Primary (First-Line) Treatment
Current guidelines recommend four major drug classes for initial therapy:
A. Thiazide-Type Diuretics
Examples: Hydrochlorothiazide, chlorthalidone, indapamide
Mechanism: Inhibit the Na⁺/Cl⁻ cotransporter in the distal convoluted tubule → increase renal sodium and water excretion → reduce blood volume → lower preload and BP. With chronic use, they also reduce peripheral vascular resistance.
Preferred in: African American patients, elderly, volume-dependent hypertension.
B. Calcium Channel Blockers (CCBs)
Examples: Amlodipine (dihydropyridine), verapamil, diltiazem
Mechanism: Block L-type voltage-gated calcium channels in vascular smooth muscle and cardiac muscle → reduce intracellular Ca²⁺ → vasodilation → decreased peripheral vascular resistance.
- Dihydropyridines (amlodipine) act mainly on vessels
- Non-dihydropyridines (verapamil/diltiazem) also reduce heart rate and contractility
Preferred in: African American patients, elderly, angina, isolated systolic hypertension.
C. ACE Inhibitors (ACEIs)
Examples: Lisinopril, enalapril, captopril, ramipril
Mechanism: Block ACE → prevent conversion of angiotensin I to angiotensin II (a potent vasoconstrictor) → decrease peripheral vascular resistance. Also prevent ACE-mediated breakdown of bradykinin → enhanced vasodilation via NO and prostacyclin release. Reduces both preload and afterload.
Preferred in: Diabetes, CKD, heart failure, post-MI, proteinuria.
Key adverse effects: Dry cough (up to 10%, due to bradykinin accumulation), angioedema (rare but serious), hyperkalemia, teratogenic (contraindicated in pregnancy).
D. Angiotensin Receptor Blockers (ARBs)
Examples: Losartan, valsartan, olmesartan, telmisartan
Mechanism: Block AT₁ receptors for angiotensin II → vasodilation, reduced aldosterone secretion, decreased sodium/water retention. Same benefit as ACEIs but without bradykinin accumulation, so no cough.
Preferred in: Same as ACEIs; also used when patient cannot tolerate ACEI due to cough.
Summary Table - First-Line Choices by Population
| Population | Preferred Drug |
|---|---|
| General (non-Black) | Thiazide, ACEI, ARB, or CCB |
| Black patients | Thiazide or CCB |
| Diabetes | ACEI or ARB |
| CKD with proteinuria | ACEI or ARB |
| Heart failure | ACEI/ARB + beta-blocker + diuretic |
| Post-MI | Beta-blocker + ACEI |
(Source: Lippincott Illustrated Reviews: Pharmacology, Figure 8.5)
3. Drug Combinations to AVOID in Hypertension
⛔ ACE Inhibitor + ARB (Dual RAAS Blockade)
This is the most important combination to avoid.
Both drugs block the renin-angiotensin-aldosterone system. Combining them offers no additional cardiovascular benefit but significantly increases the risk of:
- Hyperkalemia (life-threatening)
- Acute kidney injury
- Hypotension The ONTARGET trial confirmed this combination causes harm.
⛔ ACE Inhibitor + ARB + Aldosterone Antagonist (Triple RAAS Block)
Even more dangerous - causes severe hyperkalemia and renal failure.
⛔ Beta-Blocker + Verapamil or Diltiazem (Non-Dihydropyridine CCB)
Both drugs independently reduce heart rate and AV conduction. Together they can cause:
- Severe bradycardia
- High-degree AV block
- Cardiac arrest
⛔ Two Beta-Blockers
No additional benefit; increases adverse effects.
⛔ Potassium-Sparing Diuretic + ACE Inhibitor/ARB
Combination raises potassium to dangerous levels (hyperkalemia risk), especially in patients with CKD or diabetes.
Key principle from Lippincott Pharmacology:
"Resistant hypertension... includes use of drugs with similar mechanisms of action" as a cause of failure and risk.
4. Hypertensive Emergency
Definition
A hypertensive emergency is a life-threatening situation characterized by:
- SBP > 180 mm Hg OR DBP > 120 mm Hg
- WITH evidence of impending or progressive target organ damage (TOD)
Distinguished from Hypertensive Urgency, where BP is equally elevated but there is no acute target organ damage. Urgency can be treated more gradually (within 24-48 hours, usually oral medications).
Target Organs Involved in Hypertensive Emergency
| System | Manifestation |
|---|---|
| Brain | Hypertensive encephalopathy, hemorrhagic stroke, ischemic stroke |
| Heart | Acute coronary syndrome, acute LV failure/pulmonary edema |
| Aorta | Aortic dissection |
| Kidney | Acute renal failure, microangiopathy |
| Eye | Severe retinopathy, papilledema |
| Obstetric | Eclampsia |
5. Stepwise Management of Hypertensive Emergency
Step 1: Immediate Assessment
- Confirm BP in both arms (rule out aortic dissection if differential)
- Rapid history: duration, medications, compliance, symptoms
- Identify the type of TOD: neurological exam, ECG, chest X-ray, urinalysis, renal function, CBC
Step 2: Admit to ICU/Critical Care
- Continuous BP monitoring (intra-arterial line if available)
- IV access, cardiac monitoring, pulse oximetry
Step 3: Determine the BP Reduction Target and Speed
- General rule: Reduce MAP by no more than 20-25% in the first 1-2 hours
- Then gradually normalize BP over 24-48 hours
- Exception - Rapid lowering needed in: aortic dissection, acute pulmonary edema, eclampsia, pheochromocytoma crisis
⚠️ Too rapid a reduction can be as harmful as the hypertension itself - can precipitate cerebral, coronary, or renal ischemia.
Step 4: Choose IV Drug Based on the Type of TOD
| Condition | Drug of Choice | Alternative | Contraindicated |
|---|---|---|---|
| CNS disorder / Encephalopathy | Sodium nitroprusside | Labetalol | - |
| Intracranial hemorrhage | Sodium nitroprusside | Labetalol | - |
| Acute ischemic stroke | Labetalol | Nicardipine | - |
| Acute coronary syndrome / Unstable angina | Nitroglycerin | Labetalol, nitroprusside | - |
| Acute LV failure / Pulmonary edema | Enalaprilat | Nitroglycerin | Labetalol |
| Aortic dissection | Esmolol | Nitroprusside + propranolol | Hydralazine |
| Eclampsia | Magnesium sulfate | Hydralazine | - |
| Pheochromocytoma | Phentolamine | - | Beta-blockers alone (causes paradoxical hypertension) |
(Source: Swanson's Family Medicine Review; Goldman-Cecil Medicine)
Step 5: IV Drug Mechanisms
| Drug | Mechanism |
|---|---|
| Sodium nitroprusside | Releases nitric oxide → activates guanylyl cyclase → ↑ cGMP → smooth muscle relaxation → dilates both arterioles AND veins. Immediate onset, 1-2 min offset. Monitor for cyanide toxicity. |
| Labetalol | Combined α₁ and β (β₁ + β₂) adrenergic blocker → reduces heart rate, contractility, and peripheral vascular resistance. Onset 5-10 min. Preferred in ischemic stroke (preserves cerebral blood flow). |
| Nicardipine | L-type CCB (dihydropyridine) → arteriolar vasodilation → reduces afterload. Onset 5-15 min, offset 30-40 min (faster offset than labetalol - easier to titrate). |
| Nitroglycerin | Releases NO → venodilation (mainly) at low doses, arteriolar dilation at high doses → reduces preload predominantly. Preferred in cardiac ischemia. |
| Esmolol | Ultra-short acting selective β₁-blocker → slows heart rate, reduces contractility, slows AV conduction. First choice in aortic dissection. |
| Hydralazine | Direct arteriolar vasodilator (mechanism unclear; may involve NO pathway) → reduces afterload. Used in eclampsia. |
| Phentolamine | Non-selective α-adrenergic blocker → blocks catecholamine-mediated vasoconstriction. Drug of choice in pheochromocytoma. |
| Fenoldopam | Dopamine D₁ receptor agonist → renal and peripheral vasodilation. Useful when renal protection is needed. |
| Clevidipine | Short-acting dihydropyridine CCB → rapid arteriolar dilation. Onset 2-3 min, offset 5-15 min. |
Step 6: Transition to Oral Therapy
- Once BP is controlled with IV agents, begin oral combination therapy
- Standard oral combination: CCB or thiazide diuretic plus ACEI or ARB
- Consider IV furosemide (20-40 mg) to counter fluid expansion caused by profound vasodilation
Hypertensive Emergency Algorithm
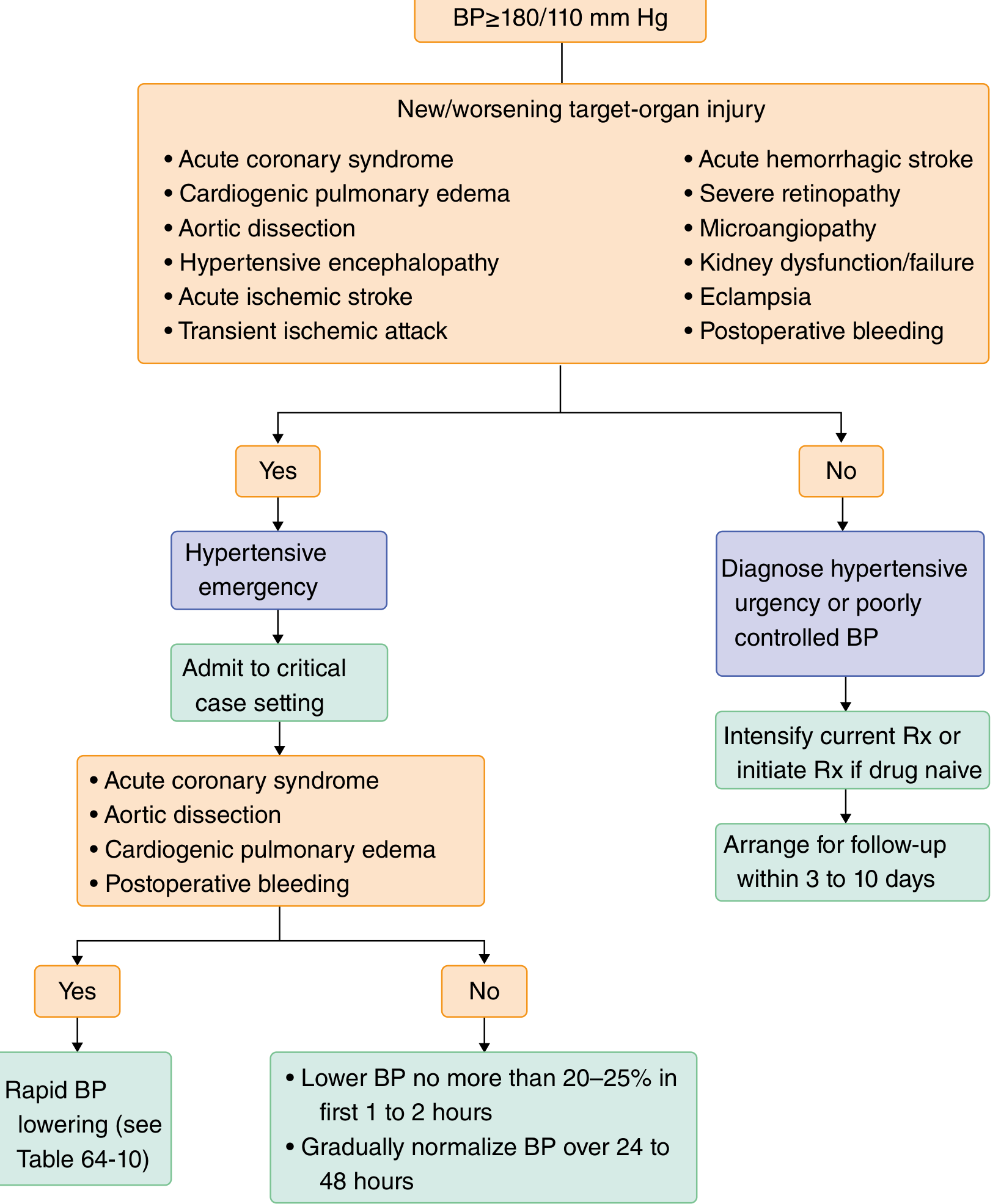
(Goldman-Cecil Medicine, Table 64-2 / Algorithm 4.5)
6. In Which Type of Hypertension Are Arteriolar Dilators Used - and Why?
Arteriolar dilators (hydralazine, minoxidil) are used in:
A. Severe / Refractory Hypertension (Resistant Hypertension)
Why: When 3-drug regimens fail to control BP, arteriolar dilators are added as 4th-line agents. They act directly on smooth muscle of arterioles to cause vasodilation, powerfully reducing peripheral vascular resistance (afterload).
B. Hypertensive Emergency with Specific Conditions
- Hydralazine is the drug of choice in eclampsia (safe in pregnancy)
- Minoxidil is used in severe resistant hypertension refractory to other drugs
C. Hypertension with Renal Failure
- Minoxidil is often used in hypertension complicated by chronic kidney disease when other agents are insufficient
Why these drugs are NOT used as monotherapy (first-line):
Arteriolar dilators cause a reflex sympathetic activation response:
- Vasodilation → fall in BP
- Baroreceptors sense drop in BP → reflex increase in sympathetic outflow
- Result: tachycardia, increased renin release, sodium/water retention (secondary hyperaldosteronism)
This is why they are always combined with a beta-blocker (to blunt reflex tachycardia) and a diuretic (to prevent fluid retention). This 3-drug combination is the classic "triple therapy" for resistant hypertension.
Hydralazine specifically causes: Headache, flushing, nausea, palpitations, and with chronic high-dose use - drug-induced lupus (anti-histone antibodies, more in slow acetylators).
Quick Reference Summary
| Topic | Key Point |
|---|---|
| Definition | SBP >130 or DBP >80 mm Hg (ACC/AHA) |
| First-line drugs | Thiazide, ACEI, ARB, CCB |
| Combination to AVOID | ACEI + ARB (dual RAAS blockade) |
| Also avoid | Beta-blocker + verapamil/diltiazem |
| Emergency vs. Urgency | Emergency = TOD present; requires IV treatment in ICU |
| BP reduction goal in emergency | Max 20-25% reduction in first 1-2 hours |
| Best drug in aortic dissection | Esmolol (beta-blocker) - hydralazine is contraindicated |
| Best drug in eclampsia | MgSO₄ or hydralazine |
| Best drug in pheochromocytoma | Phentolamine (alpha-blocker) - beta-blockers alone are contraindicated |
| Arteriolar dilators used in | Resistant/refractory hypertension, eclampsia, hypertension with CKD |
| Why not first-line | Cause reflex tachycardia and fluid retention - must be combined with beta-blocker + diuretic |
Sources: Lippincott Illustrated Reviews: Pharmacology, Goldman-Cecil Medicine (International Edition), Swanson's Family Medicine Review, 2nd ed.
This is a shared conversation. Sign in to Orris to start your own chat.