Ground glass appearance of mastoid suggestive of fibrous dysplasia explain more
Reading File
Finding Sources
Finding Sources
Searching PubMed
"fibrous dysplasia" AND mastoid
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Searching the Web
fibrous dysplasia mastoid ground glass CT appearance radiology
I now have comprehensive information to give a thorough answer. Let me compile everything.
Ground Glass Appearance of the Mastoid in Fibrous Dysplasia
What Is Fibrous Dysplasia?
Fibrous dysplasia (FD) is a benign fibro-osseous skeletal disorder in which normal cancellous bone is replaced by a fibrous stroma containing irregularly arranged spicules of woven bone. It results from a postzygotic activating mutation in the GNAS gene, which encodes the alpha-subunit of the stimulatory G protein (Gs-alpha). This leads to elevated cyclic AMP, impaired osteoblast differentiation, and the deposition of immature fibro-osseous tissue instead of mature lamellar bone.
Three forms exist:
- Monostotic (single bone) - most common (~70% of temporal bone cases)
- Polyostotic (multiple bones) - ~23% of temporal bone cases
- McCune-Albright syndrome - polyostotic FD + café-au-lait spots + precocious puberty - ~7% of temporal bone cases
Why Does Ground Glass Appear Radiographically?
The ground glass appearance is the pathognomonic radiographic sign of fibrous dysplasia and has a direct histopathological basis:
"A variable amount of irregularly arranged spicules of woven bone causes the ground-glass radiographic changes." - Cummings Otolaryngology, p. 2916
The mechanism is:
- Normal medullary bone is replaced by fibrovascular stroma
- Within this stroma, immature woven bone spicules form in a random, disorganized, whorled pattern - they lack the Haversian system of mature lamellar bone
- These tiny spicules are too small and poorly mineralized to appear as discrete trabeculae on imaging
- Instead, they create a diffuse, intermediate-density "haze" - the hallmark ground glass matrix
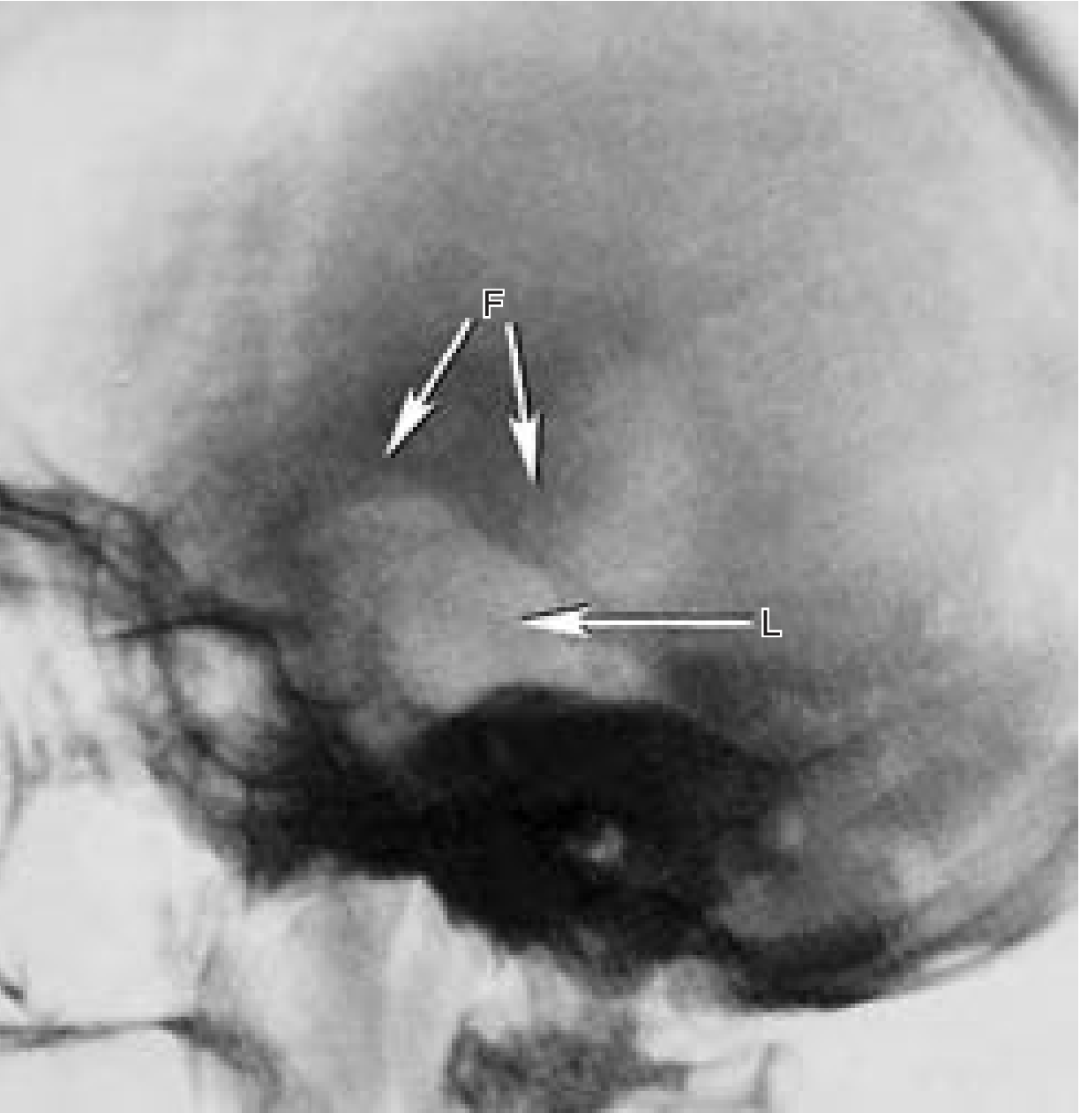
Lateral skull X-ray - fibrous dysplasia showing lytic (L) and fibrous (F) phases, with spicules of new bone creating the ground glass appearance:
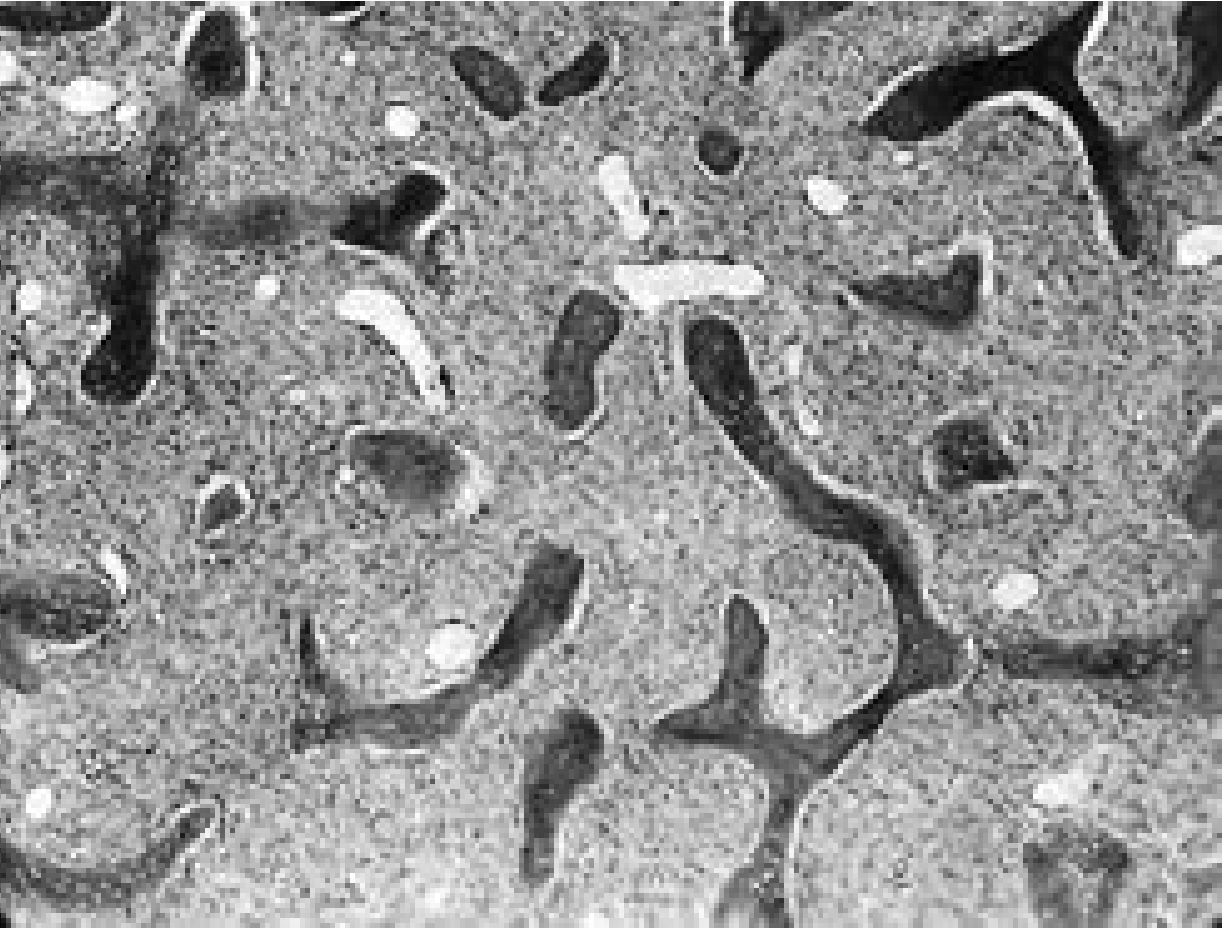
Histopathology - the irregularly arranged spicules of woven bone in a fibrovascular stroma showing the whorled pattern (x64 magnification):
Imaging Characteristics on CT (Most Useful Modality)
CT is the imaging of choice for temporal bone/mastoid FD. Three distinct patterns are recognized:
| Pattern | CT Appearance | Frequency |
|---|---|---|
| Ground glass | Homogeneous intermediate density, diffuse haze | Most common (~56%) |
| Dense/Sclerotic | Uniformly hyperdense, "ivory" bone | ~23% |
| Lytic/Cystic | Radiolucent areas with sclerotic rim | ~21% |
Key CT features of the ground glass pattern:
- Asymmetric homogeneous density that blends into normal bone
- Cortical thinning with smooth endosteal scalloping
- Bone expansion - the classic "expansile" lesion
- A "rind sign" (thin sclerotic rim) at the periphery supports benign, slow-growing FD
- No aggressive features - no cortical disruption, no periosteal reaction, no soft-tissue mass
- Attenuation values on CT are typically 70-130 HU, higher than fibrous tissue but lower than dense bone
Mastoid and Temporal Bone - Specific Presentation
The temporal bone is involved in roughly 100 reported cases of FD. Key features specific to mastoid involvement:
Clinical presentation:
- Painless, slowly progressive swelling of the mastoid or squama (this is the typical starting point)
- Age of onset: second or third decade of life - helps distinguish from exostoses
- At surgery: vascular, soft, spongy, gritty consistency - characteristic feel
Consequences of mastoid/EAC involvement:
- External auditory canal stenosis (~80% of cases) - the most common manifestation; progressive narrowing causes conductive hearing loss
- Can be mistaken for exostoses on exam (FD differs by its age of onset and vascularity)
- External canal cholesteatoma - keratin debris trapped medial to a stenotic canal
- Middle ear/ossicular involvement - additional conductive hearing loss
- Eustachian tube obstruction - conductive hearing loss
- Facial nerve palsy - from erosion of the fallopian canal (occasional)
- SNHL + vertigo - from otic capsule erosion (occasional)
- Glomus tympanicum mimic - isolated mesotympanic lesion may present as a reddish pulsatile mass with tinnitus
Differential Diagnosis of Ground Glass Mastoid
| Condition | Distinguishing Features |
|---|---|
| Fibrous dysplasia | Ground glass matrix, no aggressive features, young patient, expands bone |
| Paget's disease | Cotton wool density, older patient (>40 yr), elevated ALP |
| Otosclerosis | Halo sign around cochlea, no expansion, different clinical syndrome |
| Cholesteatoma | Lytic, soft tissue mass, erosive, no matrix mineralization |
| Exostoses | Hard, sessile, bilateral, diver history, not vascular at surgery |
| Glomus tumor | Soft tissue enhancing mass, permeative pattern ("moth-eaten") |
Pathophysiology Summary
GNAS mutation (Gs-alpha)
↓
↑ cAMP in osteoprogenitor cells
↓
Abnormal osteoblast differentiation
↓
Immature mesenchymal osteoblastic precursors proliferate
↓
Normal medullary bone replaced by fibrovascular stroma
↓
Woven bone spicules form in whorled, disorganized pattern
↓
Ground glass appearance on imaging
Management
- Conservative if asymptomatic - observe with long-term follow-up
- Bisphosphonate therapy (e.g., pamidronate) - for pain and to slow progression
- Surgery is limited to:
- Biopsy (if diagnosis uncertain)
- Canalplasty + meatoplasty for EAC stenosis - note: restenosis from regrowth is common
- A canal-wall-down mastoidectomy with wide canalplasty and skin grafting gives better long-term canal patency than simple canalplasty
- Radiotherapy is contraindicated - significantly increases risk of sarcomatous transformation
- Sarcomatous transformation rate: ~0.4% overall; more common if irradiated
Sources:
- Cummings Otolaryngology Head and Neck Surgery, pp. 2916-2917 (Fibrous Dysplasia and Otologic Manifestations)
- Schwartz's Principles of Surgery, 11th ed. (McCune-Albright/ground glass CT)
- Grainger & Allison's Diagnostic Radiology (ground glass matrix on CT)
- AJR: Fibrous Dysplasia at Skull Base
- CT Imaging of Craniofacial FD
This is a shared conversation. Sign in to Orris to start your own chat.