Peyronie disease
Reading File
Finding Sources
Searching PubMed
Peyronie disease management treatment
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Peyronie's Disease (PD)
Definition
Peyronie's disease is an acquired, progressive connective-tissue disorder of the tunica albuginea of the penis. Also called plastic induration of the penis, it leads to penile pain, penile curvature or deformity, palpable fibrous plaques, and - in many cases - difficulty or inability to have penetrative intercourse. It significantly affects quality of life and psychological well-being in both patients and their partners.
- Smith and Tanagho's General Urology, 19th Ed., p. 557
- Bailey and Love's Short Practice of Surgery, 28th Ed., p. 1572
Epidemiology
- Prevalence estimated at 3-9% of the male population; true prevalence may be higher.
- Most common between ages 45-60, but 10% of patients are younger than 40 (including teenagers).
- More common in Caucasian men.
- Associated conditions:
- Type 2 diabetes mellitus: 8% of diabetics develop PD
- Radical prostatectomy: 16% incidence of post-op PD
- Dupuytren's contracture: up to 21% of those with DC also have PD (shared gene expression patterns for collagen degradation, ossification, and myofibroblast differentiation)
- Erectile dysfunction (ED): present in 20-50% of men with PD
- Anxiety, depression, and relationship disorders affect >50% of PD patients; notably, distress does not always correlate with degree of curvature.
Pathogenesis
The exact cause is unknown, but the leading hypothesis involves:
- Repetitive microtrauma to the erect penis during intercourse (or occasionally trauma to the flaccid penis)
- Microhemorrhage between layers of the tunica albuginea (delamination)
- Initiation of the wound-healing cascade with aberrant fibrous tissue deposition
- Formation of relatively inelastic fibrous plaques beneath the tunica
Additional contributing factors include: genetic predisposition, autoimmune mechanisms, and localized wound-healing aberrations. Trauma alone cannot explain the disease - in one study of 193 penile fracture patients, none developed PD - so a susceptibility cofactor is required.
Dorsal and ventral shear stresses during intercourse likely explain why plaques are more often found dorsally, causing the characteristic dorsal curvature (toward the abdomen).
- Campbell Walsh Wein Urology, 3-Volume Set, p. 2134
Natural History - Two Phases
| Phase | Timing | Features |
|---|---|---|
| Acute (Active/Inflammatory) | Onset to ~6-12 months | Penile pain (35-45% of patients), plaque growth, progressive deformity; pain typically resolves within 6 months in 90% |
| Chronic (Fibrotic/Stable) | After 6-12 months | Plaque and curvature stabilize; spontaneous improvement is rare |
Without treatment: curvature worsens in 30-50%, stabilizes in ~47%, and spontaneously improves in a minority. The disease typically progresses for 18-24 months before stabilizing.
- Bailey and Love's Short Practice of Surgery, 28th Ed., p. 1572
- Smith and Tanagho's General Urology, 19th Ed., p. 578
Clinical Features
- Penile deformity - most commonly dorsal curvature (toward the abdomen)
- Palpable fibrous plaque(s) in the tunica albuginea
- Pain on erection (especially in the acute phase)
- Erectile dysfunction - multifactorial (pain, functional disability from curvature, vascular disease causing flail penis, psychogenic)
- Rarely: calcified plaques (visible on imaging)
Diagnosis
- Primarily clinical - history and physical examination (palpable plaque)
- Patient-produced photography of a natural erection or erection obtained by vacuum device/intracavernosal vasoactive injection for objective curvature assessment
- Ultrasonography - highest sensitivity for plaque detection (both calcified and soft-tissue elements); Doppler duplex US also assesses penile vascular status
- MRI - useful in select cases (shows active vs. calcified plaque)
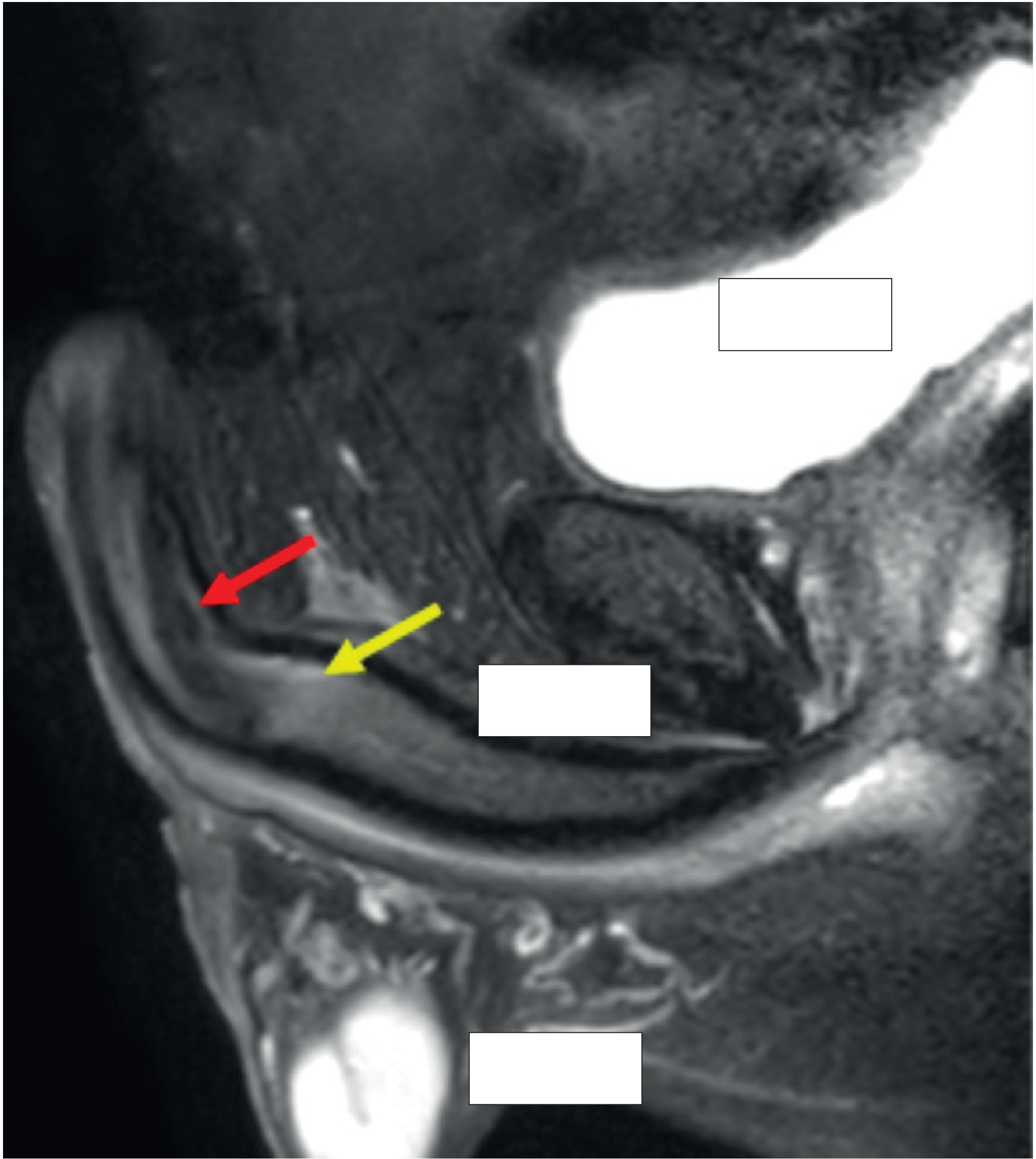
MRI in Peyronie's disease: yellow arrow = calcified plaque; red arrow = active disease on the dorsal wall of the penis. (Bailey and Love, 28th Ed.)
Treatment
General Principles
- Treatment selection depends on: stage of disease, presence of pain, severity/direction of curvature, penile length, and erectile status.
- Surgery is not indicated during the active phase; conservative/medical measures are used first.
- Surgical correction is reserved for the stable (chronic) phase when deformity prevents intercourse.
1. Nonsurgical / Medical Treatment (Active Phase)
Oral Therapy
- Pentoxifylline (first-line oral agent) - a nonspecific PDE inhibitor that inhibits TGF-beta 1-mediated inflammation, prevents type I collagen deposition, and increases nitric oxide. Used as part of multimodal therapy.
- Other agents tried (with mostly disappointing RCT evidence): colchicine, PDE5 inhibitors, vitamin E, potaba, tamoxifen, carnitine, coenzyme Q10, omega-3 fatty acids.
Intralesional Injection Therapy (three agents with RCT evidence)
| Agent | Mechanism | Outcomes | Adverse Effects |
|---|---|---|---|
| Collagenase clostridium histolyticum (CCH/Xiaflex) | Selectively degrades collagen types I and III; increases apoptosis of fibroblasts | 34% reduction in curvature (mean 17°) vs. 18% placebo; improved symptom bother | Contusions, ecchymosis, corporeal rupture (rare but serious) |
| Verapamil | Calcium-channel blocker; inhibits fibroblast proliferation, reduces ECM synthesis, increases collagenase activity | Reduces curvature and plaque-associated penile narrowing; improves quality of erection | Nausea, lightheadedness, penile pain, ecchymosis |
| Interferon alfa-2b | Decreases fibroblast proliferation; reduces collagen production; increases collagenase | 27% curvature decrease (13.5°) vs. 9% placebo | Flu-like symptoms, minor penile swelling/ecchymosis |
Collagenase CCH (Xiaflex) is the ONLY FDA-approved intralesional treatment for PD. It is restricted under a REMS program. Each treatment cycle = 2 injections 1-3 days apart; penile modeling begins 48 hours after the second injection. Minimum 6 weeks between cycles.
External Therapies
| Therapy | Notable Outcomes |
|---|---|
| Penile traction | Length increase 0.5-2.0 cm; curvature decrease ~20°; 85% overall satisfaction |
| Extracorporeal shockwave therapy (ESWT) | Improves pain and QoL; no curvature reduction |
| Electromotive drug administration (iontophoresis) | Verapamil + dexamethasone: curvature reduction 43° to 21°; verapamil alone: no benefit |
(Iontophoresis, topical therapies, ESWT, and radiation therapy are generally not recommended per evidence-based guidelines.)
2. Surgical Treatment (Stable Phase Only)
Indications: stable disease + deformity interfering with sexual intercourse (adequate erectile function required).
Option A - Plication (for adequate penile length)
- Nesbit technique or 16-dot technique
- The tunica albuginea is plicated on the side opposite to the maximum curvature
- Straightens the penis but slightly shortens it
Option B - Plaque Incision/Excision + Grafting
- Incision of the plaque + patch graft (e.g., bovine pericardial patch)
- Preferred when the penis is shorter or curvature is severe
- Corrects deformity without further shortening
Option C - Penile Prosthesis
- For patients with PD + significant ED
- Inflatable penile prosthesis + penile modeling over the device
Summary (Key Points)
- PD is a two-phase disease (active then stable)
- No effective treatment exists for the active phase - surgery is contraindicated until stabilization
- CCH (Xiaflex) is the only FDA-approved intralesional treatment
- Surgery (plication or graft) is offered in the stable phase for deformity that prevents intercourse
- Strong association with Dupuytren's contracture (fibromatosis)
- ED and psychological morbidity are common and should be actively addressed
Sources:
- Smith and Tanagho's General Urology, 19th Ed., pp. 557-605
- Bailey and Love's Short Practice of Surgery, 28th Ed., pp. 1572
- Campbell Walsh Wein Urology, 3-Volume Set, pp. 2134-2146
- Andrews' Diseases of the Skin, Clinical Dermatology
Recent evidence note: A 2025 systematic review (PMID 39186947) examined iontophoresis specifically for PD and found limited supportive data, consistent with current guidelines not recommending it. No major meta-analyses from 2024-2026 contradict the above management framework.
Help me with anatomy of penis in detail
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have all the key information needed for a comprehensive answer. Let me compile the full detailed anatomy of the penis.
Detailed Anatomy of the Penis
1. Overview and General Structure
The penis is composed of three cylindrical erectile bodies:
- Corpora cavernosa (paired, dorsal) - two cylinders of expansile vascular tissue extending from the pubic rami to the tip of the penis
- Corpus spongiosum (single, ventral) - encircles the urethra, runs from the perineal membrane to expand as the glans penis distally
All three bodies contain spongy vascular tissue capable of expanding to contain large volumes of blood.
2. Parts of the Penis
| Part | Description |
|---|---|
| Root (Radix) | Fixed part; comprises the bulb (corpus spongiosum) + two crura (corpora cavernosa); lies in superficial perineal pouch |
| Body (Shaft) | Free, mobile portion of the three corpora covered by fascia and skin |
| Glans penis | Expanded distal end of the corpus spongiosum; covered by the prepuce (foreskin) |
| Corona | Projecting rim of the glans |
| Coronal sulcus | Groove between the glans and the shaft |
| Frenulum | Fold of skin on the ventral aspect connecting the prepuce to the glans |
| Prepuce (Foreskin) | Fold of skin covering the glans; attached to the glans at the frenulum |
| External urethral meatus | Opening at the tip of the glans |
| Fossa navicularis | Widened terminal part of the urethra just inside the meatus |
3. Corpora Cavernosa
- Paired, dorsally located cylinders ensheathed by the tunica albuginea
- Proximal ends (crura) originate at the undersurface of the puboischial rami as two separate structures, then merge under the pubic arch
- Stay attached up to the glans penis
- Incomplete septum between the two corpora - allows blood to cross (important for erection physiology)
- Each corpus = a conglomeration of vascular sinusoids: larger in the center, smaller at the periphery
- Sinusoids are separated by smooth muscle trabeculae surrounded by elastic fibers, collagen, and loose areolar tissue
4. Corpus Spongiosum and Glans
| Feature | Corpus Spongiosum | Glans Penis |
|---|---|---|
| Tunica albuginea | Thin (circular layer only) | Absent |
| Main blood supply | Bulbar and spongiosal arteries | Dorsal artery |
| Venous occlusion during erection | No | No |
| Compressed by skeletal muscle | Yes (ischiocavernosus, bulbocavernosus) | No |
- The corpus spongiosum has larger sinusoids than the corpora cavernosa
- The glans lacks a tunica albuginea, so it functions as an arteriovenous fistula during erection (stays soft/compressible) - during rigid erection most venous channels are compressed, allowing engorgement
- The urethra runs eccentrically through the corpus spongiosum in the bulb, more centrally in the shaft, and widens in the glans as the fossa navicularis
5. Tunica Albuginea (Key Structure)
A bilayered fibrous sheath covering the corpora cavernosa providing flexibility, rigidity, and strength.
Layers:
- Outer layer: collagen bundles oriented longitudinally, extending from the glans to the proximal crura
- Inner layer: collagen bundles oriented circularly, supporting and containing the cavernous tissue
- Oblique fibers between the two layers
- Intracavernous pillars: radiating struts from the inner layer that augment the septum; absent between 5 o'clock and 7 o'clock positions (an area of relative weakness)
Thickness:
- Dorsal tunica: ~2.2 mm (thicker)
- Ventral tunica: ~0.8 mm (thinner - clinically relevant in penile fracture)
Principal constituent: Fibrillar collagen (type I + type III), with elastic fibers in an irregular latticed network. Elastin permits penile expansion during erection.
Emissary veins run between the inner and outer layers, piercing the outer bundles obliquely. During erection, expanding sinusoids compress these veins → venous outflow obstruction → tumescence (veno-occlusive mechanism).
6. Fascial Layers (Outer to Inner)
- Skin - thin, mobile, elastic
- Dartos fascia (= Colles fascia superiorly) - loose subcutaneous layer containing no fat; continuous with scrotal dartos
- Buck's fascia (deep penile fascia) - a strong, fibrous envelope that encloses the three corpora; also contains the deep dorsal vein, dorsal arteries, and dorsal nerves
- Tunica albuginea - directly covers each corpus
7. Ligaments
- Fundiform ligament: arises from Colles fascia; lateral, superficial; not adherent to tunica albuginea
- Suspensory ligament: arises from Buck's fascia; consists of two lateral bundles and one median bundle circumscribing the dorsal vein; attaches the tunica albuginea of the corpora to the pubic symphysis; provides support for the mobile portion of the penis. If severed (as in "penile elongation" surgery), the erect penis becomes unstable during penetration.
8. Arterial Supply
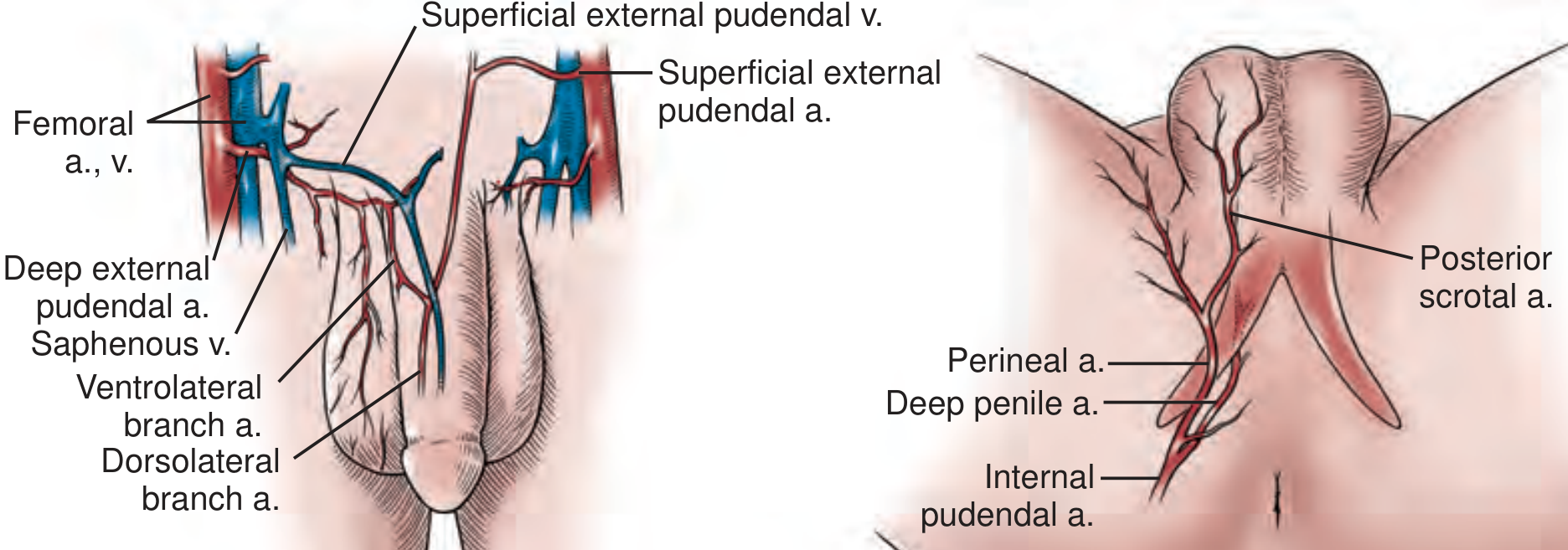
Primary source: Paired internal pudendal arteries (branches of the internal iliac arteries)
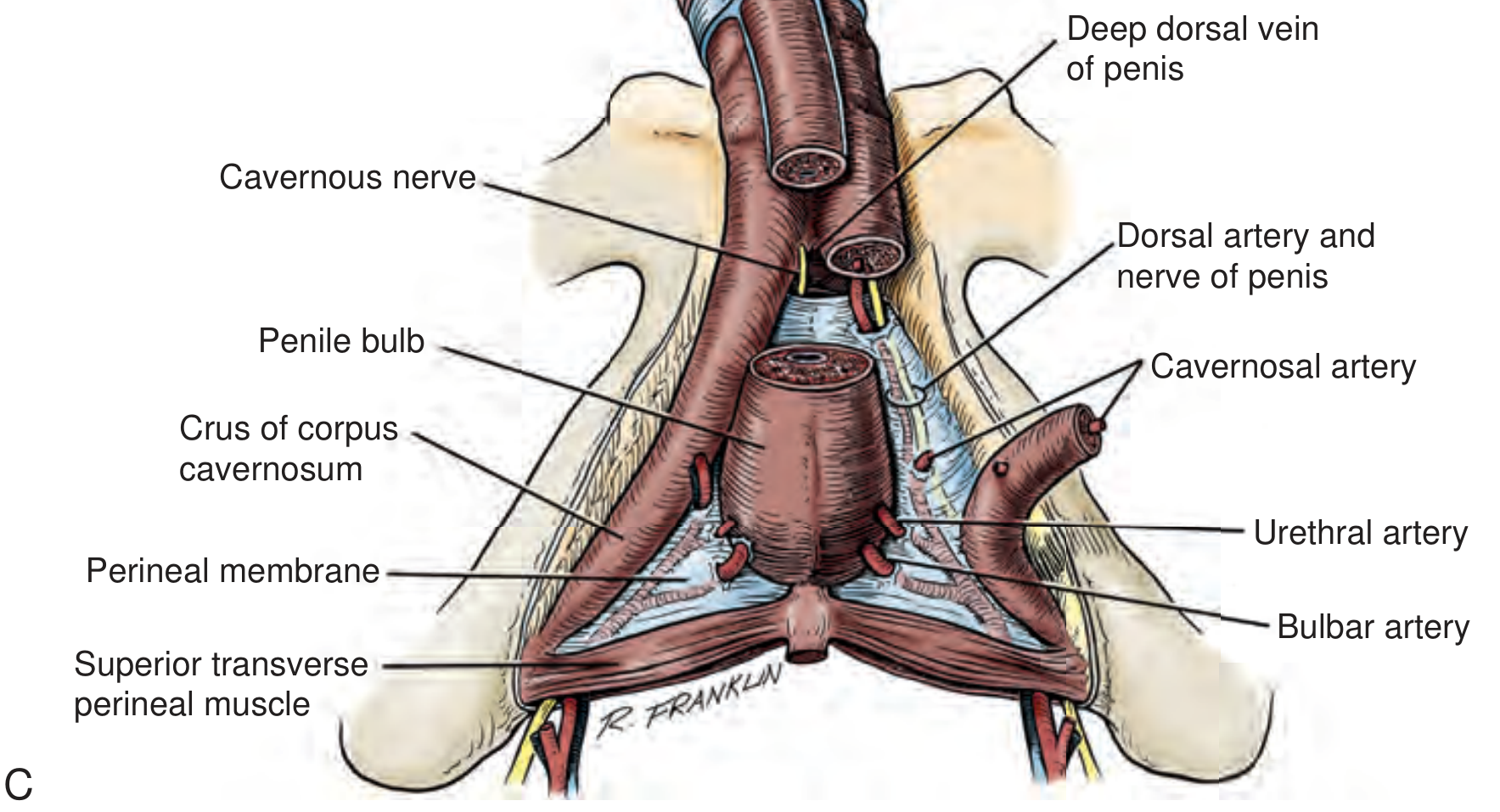
After giving off the perineal branch, the internal pudendal artery becomes the common penile artery, which travels along the medial margin of the inferior pubic ramus and divides into three terminal branches:
| Branch | Course & Territory |
|---|---|
| Cavernosal artery (deep artery) | Enters at the hilum of the penis; runs within each corpus cavernosum; gives off helicine arteries supplying the trabecular erectile tissue and sinusoids; tortuous + contracted when flaccid, dilated + straight during erection; main artery for tumescence of corpora cavernosa |
| Dorsal artery | Runs on the dorsum of the penis between the deep dorsal vein (medially) and the dorsal nerves (laterally); responsible for engorgement of the glans; also sends penetrating branches through the tunica to the cavernous arteries distally |
| Bulbourethral artery | Short, large-caliber; pierces Buck's fascia to enter the bulbospongiosus; supplies the penile bulb and corpus spongiosum |
Accessory supply:
- In ~1/3 of men, accessory arteries from the external iliac, obturator, vesical, or femoral arteries supply the penis
- ~70% of men have supply from both internal pudendal and accessory arteries
- Preservation of accessory pudendal arteries during radical prostatectomy is associated with faster recovery of sexual function
9. Venous Drainage
Three systems drain the penis:
a. Superficial System
- Superficial dorsal veins lie above Buck's fascia
- Drain penile skin and subcutaneous tissue
- Drain into the left saphenous vein (occasionally bilateral)
b. Intermediate System (within/beneath Buck's fascia)
- Emissary veins: arise from subtunical venous plexus; exit the erectile space obliquely through the tunica → drain into circumflex veins or the deep dorsal vein
- Circumflex veins: arise from the corpus spongiosum on the ventrum; travel around the lateral aspect of the corpora cavernosa; drain into the deep dorsal vein
- Deep dorsal vein: formed by 5-8 small veins at the glans forming the retrocoronal plexus; runs in the midline groove between the corpora; collects emissary and circumflex vein blood; passes beneath the pubis under the suspensory ligament → drains into the periprostatic (preprostatic) plexus
c. Deep System
- Cavernosal veins: drain the proximal crura; run deep and medial to the cavernosal arteries → drain into the internal pudendal vein
- Crural veins: arise in the intracrural space; drain into the deep dorsal vein or periprostatic plexus
10. Nerve Supply
The penis has both autonomic (sympathetic + parasympathetic) and somatic (sensory + motor) innervation.
Autonomic Innervation
- Parasympathetic (S2-S4) - via pelvic nerves → pelvic plexus → cavernous nerves; responsible for erection (vasodilation, smooth muscle relaxation)
- Sympathetic (T11-L2) - via hypogastric nerves → pelvic plexus → cavernous nerves; responsible for detumescence, emission, and ejaculation
- The cavernous nerves (autonomic) travel along the posterolateral surface of the prostate in neurovascular bundles, pierce the urogenital diaphragm, and enter the corpora at the hilum - these are the nerves at risk during radical prostatectomy
Somatic Innervation
- Dorsal nerve of the penis (branch of pudendal nerve, S2-S4):
- Sensory: skin, glans, prepuce
- Motor: ischiocavernosus and bulbocavernosus muscles (compress the crura and bulb to raise intracavernosal pressure during rigid erection)
- The dorsal nerve runs laterally to the dorsal artery on the dorsum of the penis, within Buck's fascia
Erection - Neural Summary:
- Parasympathetic activation → cavernous nerves → relaxation of helicine arteries and sinusoidal smooth muscle → increased arterial inflow
- Expanding sinusoids compress emissary veins (veno-occlusion) → blood trapping → tumescence
- Ischiocavernosus muscle contraction (somatic, S2-S4) → compresses proximal corpora → intracavernosal pressure exceeds systolic BP → rigid erection
11. Muscles Associated with the Penis
| Muscle | Attachment | Function |
|---|---|---|
| Ischiocavernosus | Ischial tuberosity → crus | Compresses the crus; creates rigid erection phase; assists in venous occlusion |
| Bulbospongiosus | Perineal body → corpus spongiosum/dorsal aponeurosis | Compresses the penile bulb; aids ejaculation; assists in erection of corpus spongiosum |
| External urethral sphincter | Surrounds membranous urethra | Voluntary control of micturition |
12. Urethra in the Penis
The penile (spongy) urethra runs through the corpus spongiosum:
- Bulbous urethra: urethra is eccentrically placed in the corpus spongiosum proximally
- Penile (pendulous) urethra: more centrally placed
- Fossa navicularis: widened terminal dilation of the urethra just inside the glans; urethra is relatively ventrally placed here
- External meatus: narrowest part, at the tip of the glans
13. Clinical Correlates
| Anatomy | Clinical Relevance |
|---|---|
| Ventral tunica thinner (0.8 mm), absent pillars at 5-7 o'clock | Penile fracture most common ventrally |
| Emissary vein compression during erection | Basis of veno-occlusive mechanism; failure → venogenic ED |
| Cavernous nerves lateral to prostate | At risk during radical prostatectomy → post-op ED |
| Suspensory ligament supports erection stability | Severing it (penile elongation) → unstable erection |
| Accessory pudendal arteries in ~1/3 of men | Must be preserved during pelvic surgery |
| Glans lacks tunica albuginea | Stays compressible during erection (protective role) |
| Tunica albuginea bilayer compresses emissary veins | Peyronie's plaques disrupt this → deformity |
Sources:
- Campbell Walsh Wein Urology, 3-Volume Set, pp. 1972-1976 (Functional & Surgical Anatomy)
- Smith and Tanagho's General Urology, 19th Ed., pp. 557, 620, 5225-5228
- Bailey and Love's Short Practice of Surgery, 28th Ed., p. 1572
This is a shared conversation. Sign in to Orris to start your own chat.