Role of imaging in paranasal sinus disease according to standard ENT textbook
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
I now have comprehensive content from the textbooks. Let me compile the full, well-structured answer based on Grainger & Allison's Diagnostic Radiology (the dedicated radiology textbook) and Scott-Brown's Otorhinolaryngology (the standard ENT reference).
Role of Imaging in Paranasal Sinus Disease
Based on Grainger & Allison's Diagnostic Radiology, Scott-Brown's Otorhinolaryngology Head & Neck Surgery, and Cummings Otolaryngology Head and Neck Surgery
1. Imaging Modalities Overview
Plain Radiography
Plain X-rays of the paranasal sinuses (Waters' view, Caldwell view, lateral) were historically the first-line investigation. They can show mucosal thickening, opacification, and air-fluid levels in the maxillary and frontal sinuses. However, plain films have largely been superseded by CT because they cannot visualise the ethmoid cells or osteomeatal unit reliably, and they miss significant pathology.
Computed Tomography (CT)
CT is the investigation of choice for paranasal sinus disease. It provides excellent bony detail and can be performed at low dose given the inherent contrast between air and bone in the sinonasal region. CT should be reconstructed in axial, coronal, and sagittal planes in both bony and soft-tissue windows.
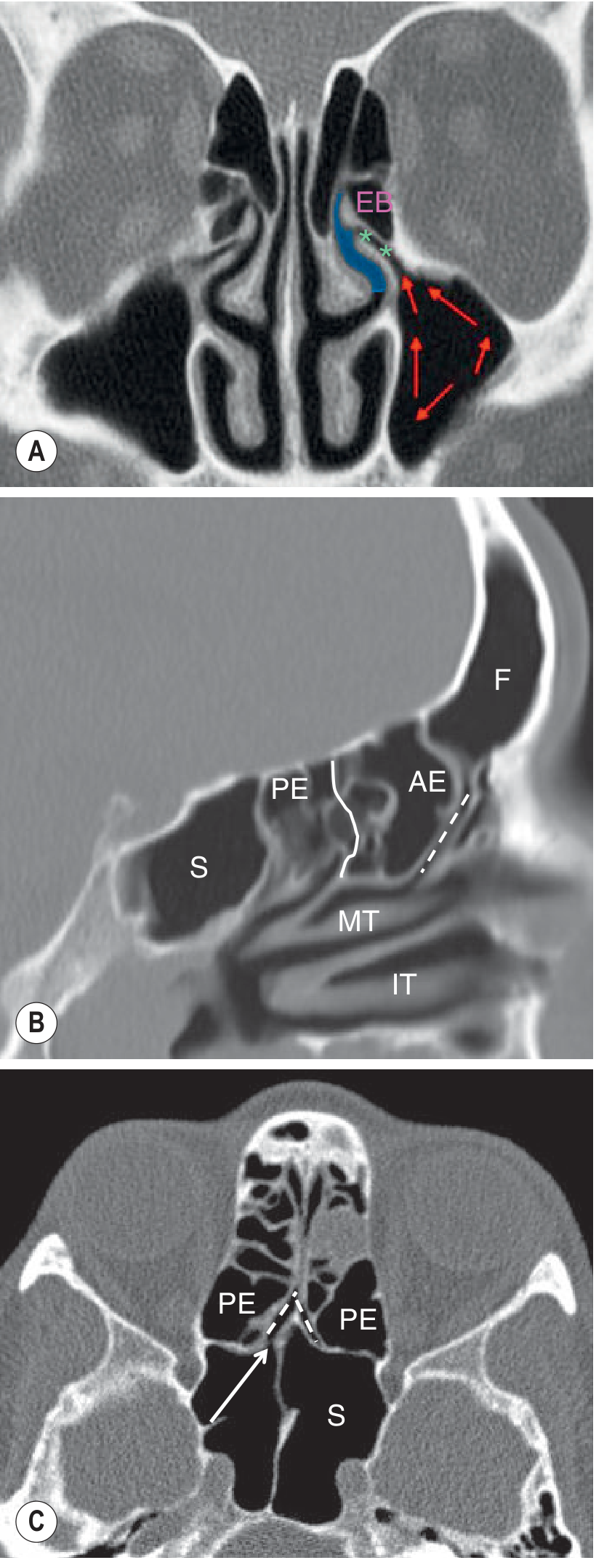
- The coronal plane is best for assessing the anterior osteomeatal unit (OMU)
- The sagittal plane best demonstrates the frontal sinus drainage pathway
- The axial plane is optimal for the sphenoethmoidal recess
Cone beam CT (CBCT) is increasingly used as an alternative to conventional CT - it offers similar anatomical detail at lower radiation dose and is suitable in the outpatient or surgical navigation setting.
Magnetic Resonance Imaging (MRI)
MRI is a problem-solver rather than a first-line tool. It does not show bony detail as well as CT but offers superior soft-tissue contrast. Its main roles include:
- Differentiating tumour from inflammatory/secretion-filled sinus
- Assessing tumour extent, particularly orbital and intracranial spread
- Characterising fungal disease (signal characteristics of concretions)
- Excluding non-sinonasal causes of anosmia (e.g., subfrontal meningioma, olfactory neuroblastoma)
- Evaluating recurrent disease post-surgery (e.g., recurrent inverted papilloma)
Grainger & Allison's Diagnostic Radiology, p. 1601
2. Indications for Imaging
CT or CBCT is indicated when:
- The patient has failed medical treatment for rhinosinusitis
- Functional Endoscopic Sinus Surgery (FESS) is being considered - CT acts as the "road map"
- Acute complications are suspected - orbital cellulitis, subperiosteal abscess, intracranial extension
- A mucocele is suspected
- A neoplastic lesion is suspected
MRI is indicated additionally when:
- Soft-tissue tumour characterisation is needed
- Orbital or intracranial extension needs to be accurately mapped
- Invasive fungal sinusitis is suspected in immunocompromised patients
- CT findings are equivocal between tumour and secretions
3. What to Assess on CT in Rhinosinusitis
A systematic radiological assessment of a sinus CT should include:
1. Anatomical variants that may predispose to disease or complicate surgery:
- Deviated nasal septum and septal spur
- Concha bullosa (pneumatised middle turbinate) or paradoxical turbinate turn - both can narrow the middle meatus
- Hypoplasia or enlargement of structures (maxillary antrum, frontal sinus, ethmoidal bulla)
- Anomalous air cells: frontoethmoidal, sphenoethmoidal, and infraorbital (Haller) cells
2. Extent of disease in relation to mucociliary pathways:
- Does antral inflammation reach the ostium, infundibulum, or middle meatus?
- Is the whole osteomeatal unit involved?
- Does frontal or sphenoid sinus disease extend to the sinus opening or beyond?
- Are there fluid levels or bubbly secretions (suggesting an acute component)?
3. Bony changes:
- Bony thickening suggesting chronicity
- Bony erosion or destruction suggesting a more aggressive process (tumour, invasive fungal disease)
4. Dental disease:
- Radicular cysts or periapical infection may cause reactive maxillary antral inflammation - the underlying dental cause must be identified
5. Complications:
- Orbital extension (subperiosteal abscess, orbital cellulitis)
- Intracranial extension (rare)
6. Post-nasal space assessment
7. Previous surgery: extent of prior FESS, any residual anatomical barriers
8. Soft-tissue window review: to identify fungal disease (high-attenuation concretions), desiccated secretions, tumour, and pathology extending into the pre/post-antral space, pterygopalatine fossa (PPF), or orbit - especially important in immunocompromised patients at risk of invasive fungal sinusitis.
Grainger & Allison's Diagnostic Radiology, p. 1601-1602
4. Specific Conditions and Their Imaging Features
Rhinosinusitis
- CT/CBCT: mucosal thickening, opacification, air-fluid levels (acute), bony thickening (chronic)
- MRI: T2 high-signal mucosal thickening; fluid levels clearly demonstrated
Nasal Polyposis
- CT: bilateral soft-tissue density filling the nasal cavity and sinuses, with widening of the middle meati; may show remodelling of bony walls
- MRI: post-gadolinium T1 images show peripheral mucosal enhancement distinguishing polyps from retained secretions; can delineate extent to frontal, ethmoidal, and maxillary sinuses
Mucocele
- An expanding mucus-filled sinus with thinned/dehiscent walls. CT shows a homogeneous soft-tissue density lesion expanding and remodelling the sinus walls; most common in the frontal and ethmoidal sinuses.
- MRI: signal varies with protein content of secretions; T1 and T2 can both be high signal.
Fungal Sinusitis
CT features:
- Non-invasive (fungal ball/mycetoma): high-attenuation central concretions within a sinus (typically maxillary), with or without calcification. Use soft-tissue window settings (~2000 HU window width, centred at -250 HU) to accentuate this.
- Allergic Fungal Rhinosinusitis (AFRS): heterogeneous high-attenuation material ("double density" sign), sinus expansion, possible lamina papyracea erosion and intracranial extension in severe cases
MRI features of fungal sinusitis:
- T1: central hypointensity with peripheral enhancement
- T2: central hypointensity or signal void (due to heavy metals - iron, magnesium, manganese - and calcium within fungal concretions)
- IV gadolinium: can assess uncertain cases or orbital/intracranial complications
Scott-Brown's Otorhinolaryngology, p. 1098
Osteoma
- CT: well-defined, sessile or pedunculated, high-density bony lesion
- Most common in the frontal sinus (80%), followed by ethmoid (20%); rarely maxillary or sphenoid
- Usually an incidental finding; surgery is considered if >50% of sinus volume is occupied or if drainage is compromised
Inverted Papilloma
- CT: middle meatal soft-tissue mass, usually unilateral; characteristic lobulated outline; 10% show calcification at the site of attachment; bony thickening of the sinus wall at the attachment site
- MRI: characteristic convoluted cerebriform pattern on T2-weighted imaging
- CT is usually satisfactory for primary assessment; MRI is reserved mainly for assessing recurrence post-surgery
- The site of bony attachment must be identified as subperiosteal resection is required to prevent recurrence
Juvenile Angiofibroma
- CT: soft-tissue mass originating at the sphenopalatine foramen; characteristic widening of the pterygopalatine fossa (PPF); erosion of the medial pterygoid plate and vidian canal aperture; erosion of the adjacent skull base
- A nasal mass with widened PPF in an adolescent male is pathognomonic
- Contrast-enhanced MRI is complementary to CT for accurate pre-surgical delineation and embolisation planning
Sinonasal Malignancy
- CT: bony erosion (e.g., lamina papyracea) suggests aggressive disease
- MRI: superior for defining soft-tissue extent; can distinguish preserved orbital periosteum (meaning orbital contents are not invaded) from actual orbital fat/muscle invasion - this distinction is critical for surgical planning
- Both CT and MRI should be used together for staging
5. CT as the Surgical Road Map for FESS
Before FESS, CT is mandatory. It serves as the surgeon's road map and must be reviewed systematically to:
- Confirm the extent and distribution of disease
- Identify all relevant anatomical variants
- Identify any high-risk anatomy: position of the skull base (especially a low or asymmetric cribriform plate), course of the internal carotid artery (dehiscent within the sphenoid), position and dehiscence of the optic nerve, variations in the Onodi cell
- Plan the extent of surgery required (e.g., whether uncinate process removal alone will suffice, or whether a full OMU procedure, frontal recess surgery, or sphenoidal opening is needed)
- Identify intraorbital extension of ethmoidal cells (Haller cells) that may complicate antrostomy
Intraoperative image-guided navigation (using the preoperative CT as a reference) is increasingly used in complex revision cases.
Summary Table
| Modality | Primary Role | Limitations |
|---|---|---|
| Plain X-ray | Historical first-line; detects maxillary/frontal opacification | Cannot visualise OMU or ethmoid; largely obsolete |
| CT (low-dose) | Investigation of choice; pre-FESS road map; anatomical variants; complications | Radiation; poor soft-tissue differentiation |
| CBCT | Lower dose alternative; surgical navigation | Less widely available |
| MRI | Tumour vs inflammation; fungal characterisation; orbital/intracranial extension | No bony detail; susceptibility artefact; longer scan time |
Sources: Grainger & Allison's Diagnostic Radiology (pp. 1601-1606); Scott-Brown's Otorhinolaryngology Head & Neck Surgery - Vol 1 (pp. 1097-1098); Cummings Otolaryngology Head and Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.