blood supply of the heart
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough breakdown of the blood supply of the heart, drawn from multiple authoritative textbooks (Guyton & Hall, Medical Physiology, Morgan & Mikhail's Clinical Anesthesiology, and Barash's Clinical Anesthesia).
Blood Supply of the Heart
Overview
The entire blood supply to the myocardium derives from the right coronary artery (RCA) and the left coronary artery (LCA), which originate at the root of the aorta just behind the cusps of the aortic valves. Despite the heart representing less than 0.5% of total body weight, it receives approximately 5% of resting cardiac output (~225 mL/min). The main coronary arteries lie on the epicardial surface; smaller branches penetrate into the muscle mass. Only the innermost ~0.1 mm of the endocardium can be nourished directly from intracavitary blood - the rest depends entirely on the coronary circulation.
- Guyton and Hall Textbook of Medical Physiology
- Medical Physiology (Boron & Boulpaep)
Arterial Supply
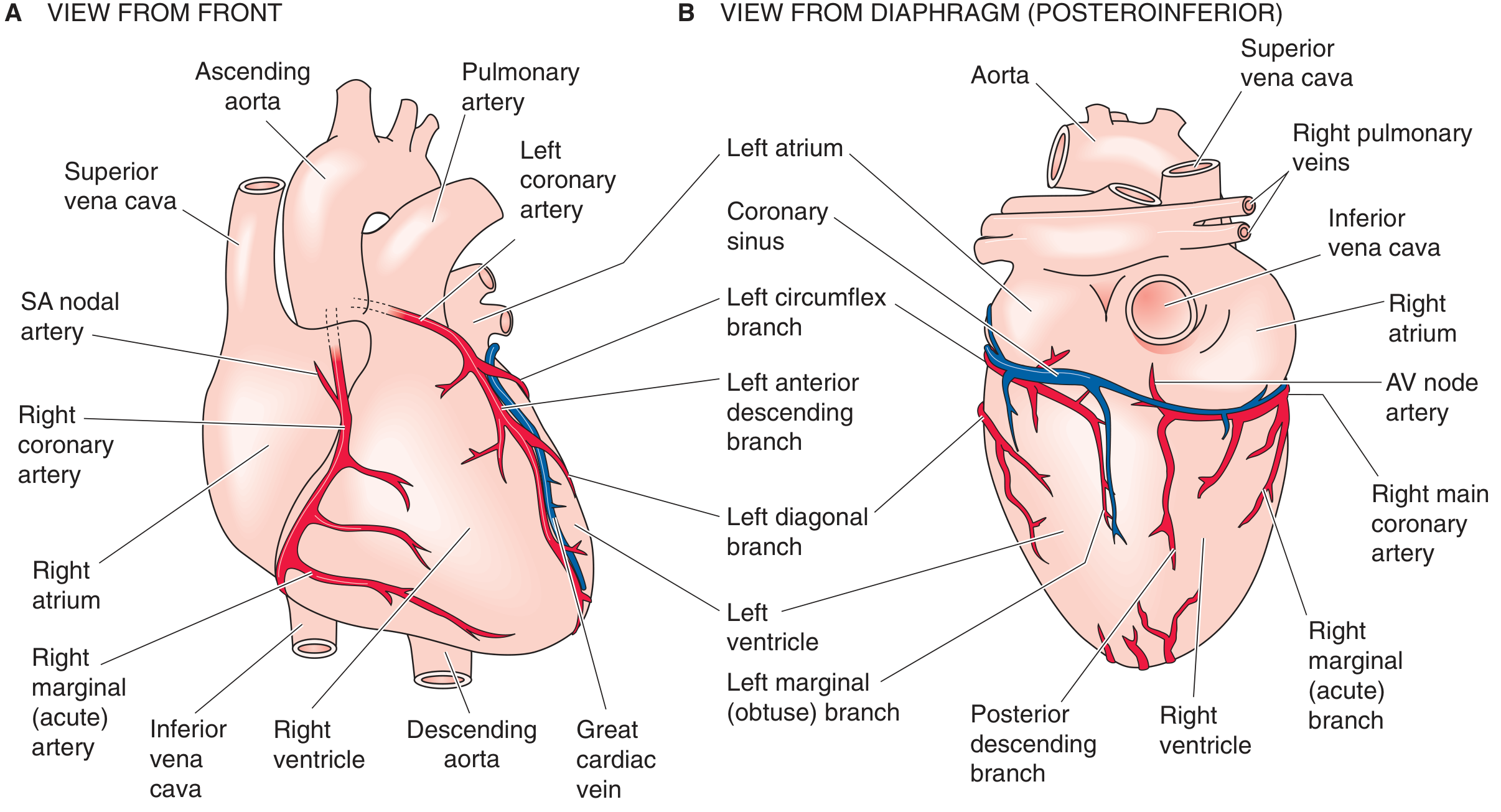
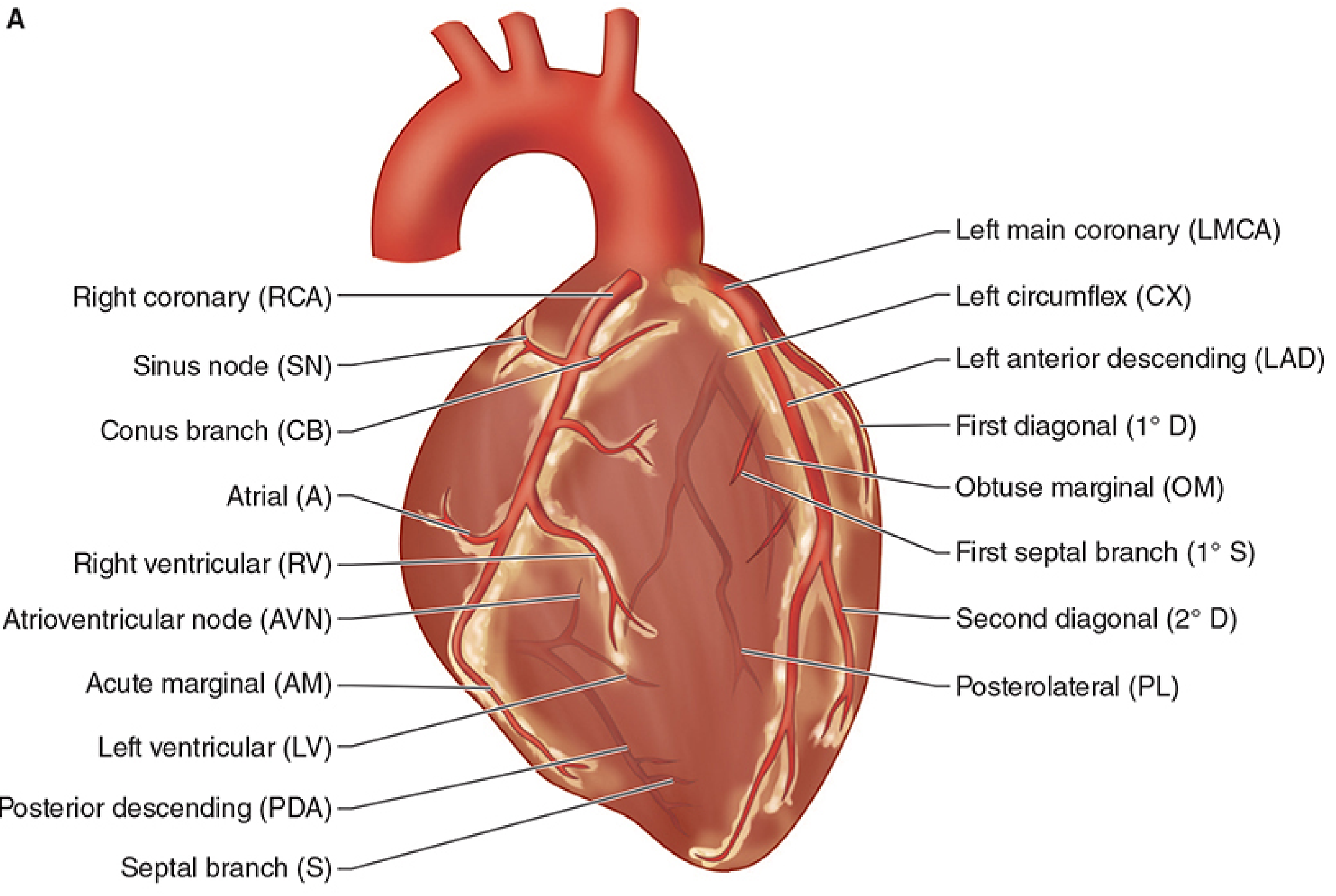
1. Right Coronary Artery (RCA)
- Supplies the right atrium, most of the right ventricle, and the inferior wall of the left ventricle
- In ~85% of people (right dominant), the RCA gives rise to the posterior descending artery (PDA), which supplies the superior-posterior interventricular septum and the inferior wall
- The remaining 15% have a left dominant circulation, where the PDA arises from the left circumflex
- Key branches:
- SA nodal artery - from the RCA in ~60% of individuals
- AV nodal artery - from the RCA in 85-90% of individuals
- Acute marginal (right marginal) branch - supplies the right ventricular free wall
- Posterior descending artery (PDA) - in right-dominant cases
2. Left Main Coronary Artery (LMCA)
- A short trunk that bifurcates into two principal branches:
a. Left Anterior Descending Artery (LAD)
- Descends in the anterior interventricular groove
- Supplies:
- Anterior and lateral walls of the left ventricle
- Anterior two-thirds of the interventricular septum (via septal perforators)
- The apex of the heart
- Part of the right ventricle
- Key branches: septal perforators, diagonal branches
b. Left Circumflex Artery (LCx/CX)
- Courses in the left AV groove
- Supplies the left atrium and the lateral wall of the left ventricle
- Branches: obtuse marginal branches
- In left-dominant circulation, wraps around to become the PDA
- Gives the SA nodal artery in ~40% of people, and the AV nodal artery in 10-15%
Coronary Dominance
| Dominance | PDA Origin | Frequency |
|---|---|---|
| Right dominant | RCA | ~85% |
| Left dominant | LCx | ~15% |
Dominance is defined by which artery supplies the PDA (and thus the posterior septum and inferior wall).
Blood Supply to the Conduction System
| Structure | Primary Supply | Frequency |
|---|---|---|
| SA node | RCA | 60% |
| SA node | LAD | 40% |
| AV node | RCA | 85-90% |
| AV node | LCx | 10-15% |
| Bundle of His | Dual (PDA + LAD) | - |
| Anterior papillary muscle (mitral) | Dual (LAD diagonals + LCx marginals) | - |
| Posterior papillary muscle (mitral) | PDA only (usually) | More vulnerable to ischemia |
- Morgan & Mikhail's Clinical Anesthesiology, 7e
Venous Drainage
Blood returns from the myocardium through three systems:
- Coronary sinus - the dominant route; drains ~75% of left ventricular coronary venous blood into the right atrium. Tributaries include the great, middle, and small cardiac veins.
- Anterior cardiac veins - drain most of the right ventricular venous blood directly into the right atrium (bypass the coronary sinus)
- Thebesian veins (smallest cardiac veins) - minute vessels that drain small amounts of blood directly into all four cardiac chambers. Because their drainage enters the ventricles, this deoxygenated blood bypasses the pulmonary circulation, contributing to a small physiological shunt.
- Guyton & Hall; Medical Physiology (Boron & Boulpaep)
Phasic Nature of Coronary Blood Flow
Coronary perfusion is unique - unlike other systemic vascular beds, it is intermittent rather than continuous:
- Left ventricle: perfused almost entirely during diastole. During systole, intramyocardial pressures approach systemic arterial pressure, nearly occluding the intramural vessels. Left coronary perfusion pressure = aortic diastolic pressure - LVEDP.
- Right ventricle: perfused during both systole and diastole because right ventricular systolic pressures are much lower.
This is why aortic diastolic pressure (not MAP) is the most important determinant of left heart myocardial perfusion. Conditions that raise LVEDP (e.g., heart failure) or lower diastolic pressure (e.g., aortic regurgitation, hypotension) compromise left ventricular perfusion.
- Morgan & Mikhail's Clinical Anesthesiology, 7e
Collateral Circulation
Direct anastomotic connections and collateral vessels exist between distal coronary branches. These provide alternative routes of blood flow if a primary vessel is occluded. Their presence and development is variable - they can become critically important in chronic ischemic heart disease as a protective adaptation.
Clinical Correlates
| Coronary Artery | Territory | Clinical Consequence of Occlusion |
|---|---|---|
| LAD | Anterior LV, septum, apex | Anterior MI, LBBB, anterior wall motion abnormality |
| LCx | Lateral LV wall | Lateral MI; may be electrically "silent" |
| RCA | Inferior LV, RV, AV node | Inferior MI, AV block, RV infarction |
| PDA (RCA in right dominance) | Posterior septum, inferior wall | Inferior-posterior MI |
| Posterior papillary (PDA only) | Papillary muscle | More vulnerable to ischemia - can cause acute mitral regurgitation |
Sources: Guyton and Hall Textbook of Medical Physiology; Medical Physiology (Boron & Boulpaep); Morgan & Mikhail's Clinical Anesthesiology, 7e; Barash's Clinical Anesthesia, 9e
This is a shared conversation. Sign in to Orris to start your own chat.