Dysfunctional uterine bleeding
Reading File
Finding Sources
Finding Sources
Searching PubMed
"dysfunctional uterine bleeding" OR "abnormal uterine bleeding" management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Dysfunctional Uterine Bleeding (DUB)
Definition
Dysfunctional uterine bleeding (DUB) is uterine bleeding that lacks an underlying structural or organic abnormality - it is a diagnosis of exclusion. It most commonly stems from hormonal disturbances disrupting the normal hypothalamic-pituitary-ovarian (HPO) axis.
Note: The term "DUB" has been largely replaced in modern classification by the broader term Abnormal Uterine Bleeding (AUB) under the FIGO PALM-COEIN system (2011, updated 2018), though DUB remains widely used clinically and in examinations.
- Robbins & Kumar Basic Pathology, p. 589; Robbins Cotran & Kumar Pathologic Basis of Disease, p. 927
Normal Menstrual Cycle (Baseline)
| Parameter | Normal Range |
|---|---|
| Duration | 4.5 - 8 days |
| Interval | 24 - 38 days |
| Blood loss | ≤30 mL average; >80 mL = abnormal |
The endometrium depends on the sequential and precisely timed action of estrogen (proliferative phase) and progesterone (secretory phase). Estrogen drives glandular and stromal proliferation; progesterone down-regulates estrogen receptors, suppresses proliferation, and promotes differentiation. Withdrawal of both hormones triggers menstruation via vasoconstriction of spiral arterioles.
- Tintinalli's Emergency Medicine, p. 649
FIGO PALM-COEIN Classification of AUB
The modern FIGO system divides AUB into:
| Category | Examples |
|---|---|
| P - Polyps | Endometrial polyps |
| A - Adenomyosis | Ectopic endometrial glands in myometrium |
| L - Leiomyoma | Submucosal fibroids most symptomatic |
| M - Malignancy/Hyperplasia | Endometrial carcinoma, atypical hyperplasia |
| C - Coagulopathy | Von Willebrand disease (most common), platelet disorders |
| O - Ovulatory dysfunction | Classic DUB - anovulatory cycles, luteal phase defect |
| E - Endometrial | Intrinsic endometrial hemostatic defects |
| I - Iatrogenic | OCPs, anticoagulants, tamoxifen, SSRIs |
| N - Not yet classified | Rare/undetermined |
Structural causes = PALM. Non-structural causes = COEIN.
- Schwartz's Principles of Surgery, p. 1822; Tintinalli's Emergency Medicine, p. 650
Causes of DUB / AUB by Age Group
| Age Group | Common Causes |
|---|---|
| Prepuberty | Precocious puberty (hypothalamic, pituitary, or ovarian origin) |
| Adolescence | Anovulatory cycle (HPO axis immaturity), coagulation disorders (up to 20% have a coagulopathy; VWD most common) |
| Reproductive age | Pregnancy complications, anatomic lesions (fibroids, polyps, adenomyosis, carcinoma), anovulatory DUB, luteal phase defect |
| Perimenopausal | Anovulatory DUB, leiomyomas, polyps, carcinoma, thyroid dysfunction |
| Postmenopausal | Endometrial atrophy (most common ~30%), exogenous hormone use (~30%), endometrial lesions including cancer (~30%) |
- Robbins Cotran & Kumar, Table 22.2; Tintinalli's Emergency Medicine, Table 96-3
Pathophysiology of Anovulatory DUB
Anovulation is the most common cause of DUB.
Without ovulation:
- No corpus luteum is formed
- No progesterone is secreted
- Endometrium is exposed to unopposed estrogen - continuous proliferation without secretory transformation
- The endometrium becomes thickened and eventually unstable, leading to irregular, often heavy shedding without the structural support of progesterone-induced decidualization
This produces proliferative-type glands with stromal breakdown on histology (the classic anovulatory endometrium - panel C in the image below).
Causes of anovulation:
- HPO axis immaturity (menarche) or dysregulation (perimenopause)
- Endocrine disorders: thyroid disease, adrenal disease, hyperprolactinemia (pituitary tumors), PCOS
- Functioning ovarian tumors (granulosa cell tumors secreting estrogen)
- Generalized metabolic disturbances: obesity, malnutrition, chronic illness
Luteal phase defect is a less common cause - insufficient progesterone production by the corpus luteum, leading to premature shedding.
- Robbins Cotran & Kumar, p. 927; Robbins & Kumar Basic Pathology, p. 596
Histological Appearance
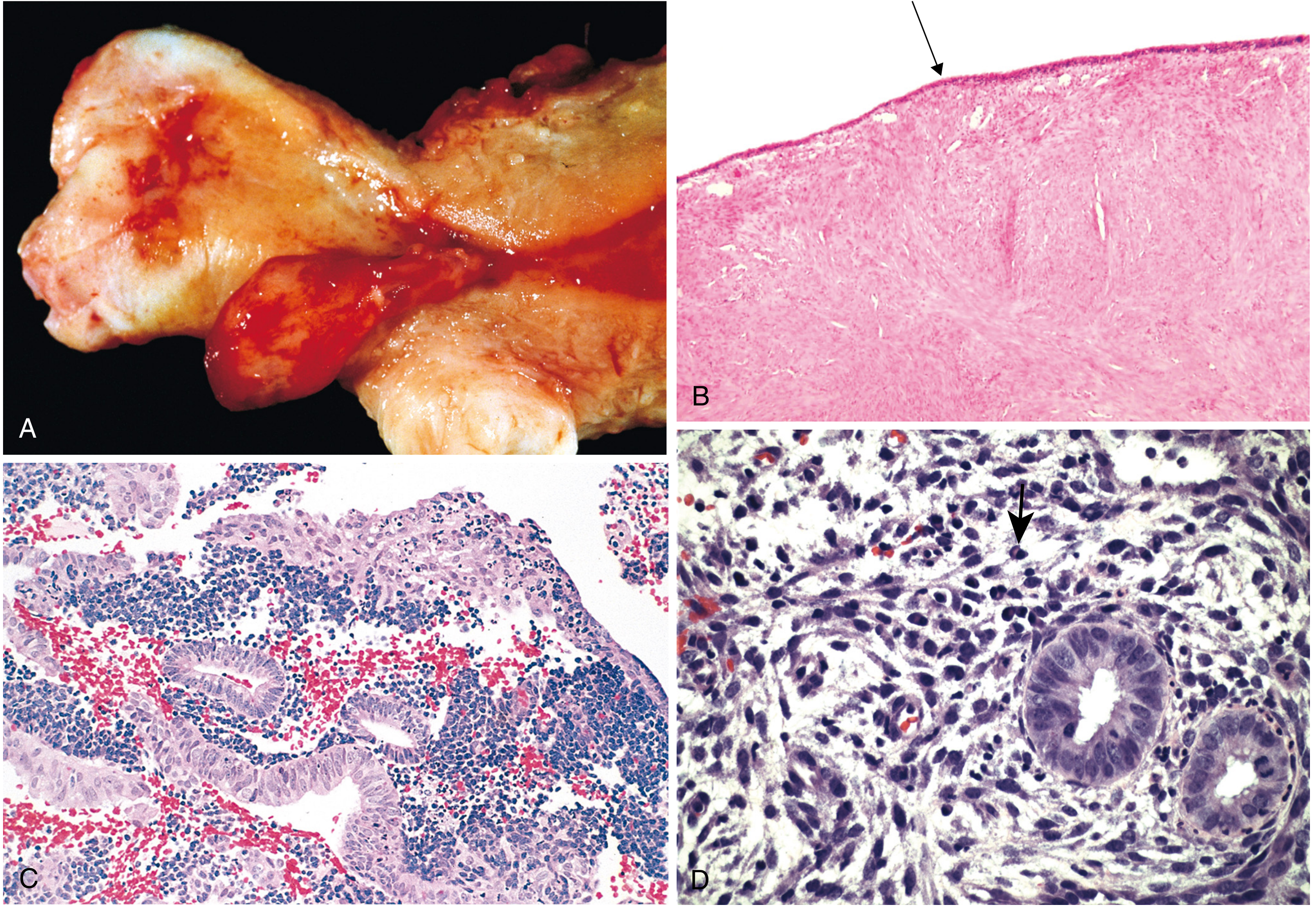
Fig. 22.20 - Common causes of abnormal uterine bleeding. (C) Anovulatory DUB: proliferative glands with stromal breakdown. (D) Chronic endometritis: plasma cells (arrow). - Robbins Cotran & Kumar
Clinical Features
- Irregular, unpredictable bleeding - varying in timing, duration, and amount
- Menorrhagia - heavy but regular bleeding
- Metrorrhagia - bleeding at irregular intervals
- Menometrorrhagia - both heavy and irregular
- Absence of ovulatory symptoms (no mid-cycle pain, no premenstrual breast tenderness)
- Signs of anemia in chronic cases
History Red Flags
- Heavy menses since menarche - screen for coagulopathy
- Postcoital bleeding - consider cervical pathology
- Postmenopausal bleeding - malignancy until proven otherwise
- Medications: anticoagulants, SSRIs, tamoxifen, ginseng
Investigations
Initial workup:
- Pregnancy test (urine/serum beta-hCG) - always first
- CBC (hemoglobin, platelet count)
- TSH
- Coagulation screen (PT, aPTT, von Willebrand panel) - especially in adolescents
- LH, FSH, prolactin if anovulation suspected
- Pelvic ultrasound - assess endometrial thickness, structural lesions
Further workup:
- Endometrial biopsy - mandatory for postmenopausal bleeding, age >45, or risk factors for carcinoma
- Saline infusion sonohysterography or hysteroscopy - if polyp/fibroid suspected
- MRI - for adenomyosis characterization
Management
Acute Heavy Bleeding (Emergency)
| Agent | Dose | Notes |
|---|---|---|
| Conjugated equine estrogen (Premarin) | 25 mg IV q4-6h | Until bleeding diminishes; antiemetics needed; contraindicated in VTE, vascular disease, malignancy |
| Tranexamic acid | 1.0-1.3 g IV, then 1 g PO TID | Antifibrinolytic; FDA-approved for menorrhagia; effective in ~3h; contraindicated in VTE/thrombophilia |
| Combined OCP (monophasic, <35 mcg EE) | 3 tabs daily x7 days | Then taper; bleeding stops in ~3 days; antiemetics; multiple contraindications |
| Medroxyprogesterone acetate | 20 mg PO TID x7 days | For estrogen contraindications; slower response (>3 days) |
| Fluid resuscitation/transfusion | PRN | For hemodynamic compromise |
- Tintinalli's Emergency Medicine, Table 96-4
Chronic/Maintenance Medical Management
- Combined OCP - first-line for most reproductive-age women; regulates cycles, reduces blood loss
- Progestin-only therapy - medroxyprogesterone acetate cyclically or continuously; useful when estrogen contraindicated
- Levonorgestrel-releasing IUD (Mirena) - highly effective for chronic heavy menstrual bleeding; reduces blood loss by 80-90%
- NSAIDs (naproxen 500 mg BD, ibuprofen 400-800 mg TID, mefenamic acid) - reduce prostaglandin-mediated blood loss by 20-50%; useful as adjunct
- Tranexamic acid PO - 1 g TID x5 days during menses
- GnRH agonists - temporary (max 6 months); used pre-surgically or to induce amenorrhea
Surgical Management
| Procedure | Indication | Notes |
|---|---|---|
| Dilatation & Curettage (D&C) | Acute, uncontrolled bleeding; diagnostic | Temporary; not definitive treatment |
| Endometrial ablation | Failed medical therapy, no desire for fertility | ~50% amenorrhea rate, ~33% reduced bleeding; 40% may still need hysterectomy later |
| Myomectomy | Symptomatic fibroids with fertility preservation | 25-30% recurrence rate |
| Uterine artery embolization | Symptomatic fibroids | Effective alternative to myomectomy |
| Hysterectomy | Definitive treatment; failed conservative therapy | Most common indication in USA is fibroid-related AUB |
- Schwartz's Principles of Surgery, p. 1822-1823
Key Points Summary
- DUB = uterine bleeding without structural cause; a diagnosis of exclusion
- Anovulation is the most common cause - occurs at the extremes of reproductive life (menarche, perimenopause)
- Modern classification uses FIGO PALM-COEIN - "DUB" maps to the "O" (Ovulatory dysfunction) category
- Always rule out pregnancy first
- Screen adolescents for coagulopathy - up to 20% have an underlying disorder (VWD most common)
- Postmenopausal bleeding = endometrial carcinoma until proven otherwise
- Unopposed estrogen (from anovulation) can cause endometrial hyperplasia - a precursor to carcinoma
- Management is tailored by age, severity, fertility desires, and underlying etiology
Recent Evidence: A 2025 systematic review (PMID 39617186) on etiology and diagnosis of heavy menstrual bleeding across adolescents and adults found coagulopathy is significantly underdiagnosed, supporting broader hemostatic screening, particularly in adolescents presenting with heavy bleeding from menarche.
This is a shared conversation. Sign in to Orris to start your own chat.