Tracheoesophageal fistula. Anaesthetic management in a one day baby posted for tracheoesophageal fistula repair
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching PubMed
tracheoesophageal fistula neonatal anesthesia management
I now have comprehensive content from three major anaesthesia textbooks. Let me compile the full answer.
Anaesthetic Management of Tracheoesophageal Fistula (TEF) in a Neonate (Day 1 of Life)
1. Understanding the Lesion
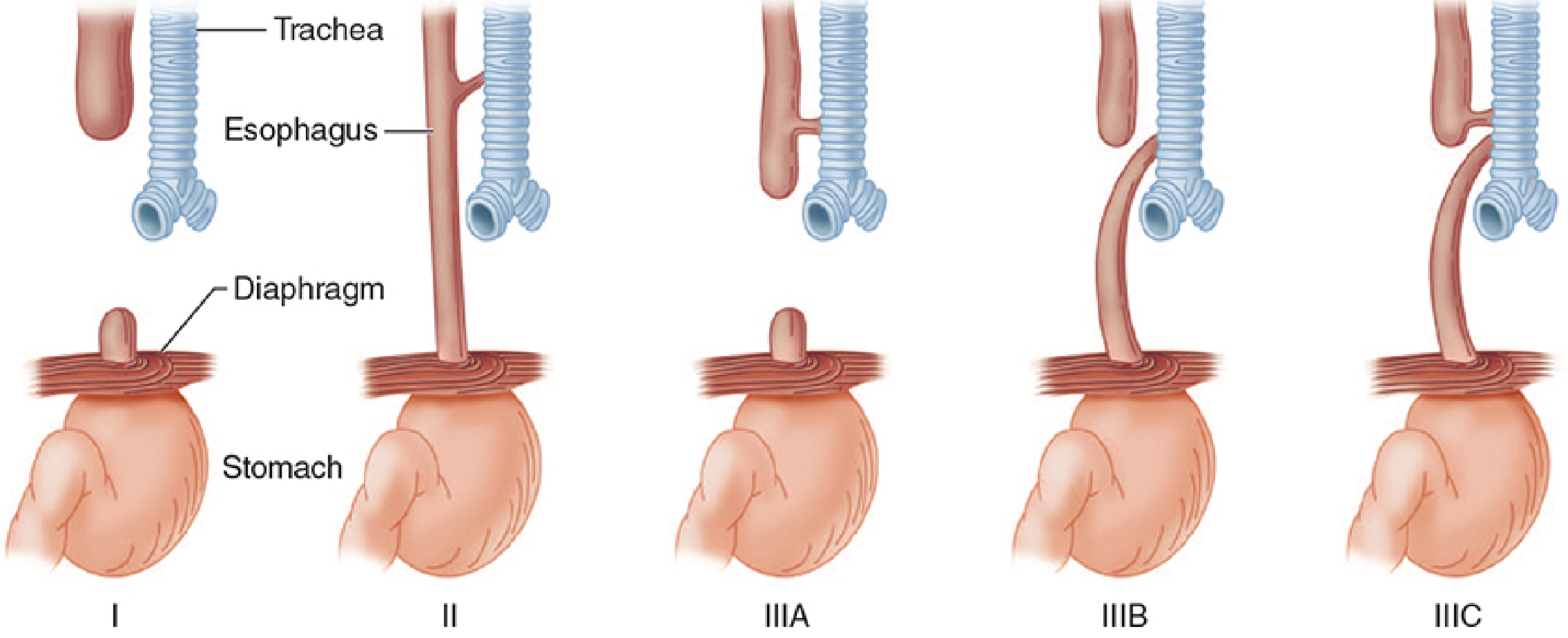
The most common variant (Type IIIB, ~90%) consists of a blind proximal esophageal pouch and a fistula connecting the distal trachea to the esophagus. The fistula is typically located just above the carina on the posterior wall of the membranous trachea. The characteristic triad is choking, coughing, and cyanosis with feeding. Diagnosis is confirmed by failure to pass a nasogastric tube into the stomach.
2. Preoperative Assessment and Preparation
Associated Anomalies (MANDATORY workup)
- Screen for VACTERL association: Vertebral, Anal atresia, Cardiac defects, TracheoEsophageal fistula, Renal anomalies, Limb defects
- Echocardiogram: Rule out congenital heart disease and right-sided aortic arch (alters surgical approach) - ~15-25% have cardiovascular anomalies
- Abdominal ultrasound: Rule out major renal abnormalities
- ~50% of affected infants have associated congenital anomalies
Respiratory Status
- Assess for aspiration pneumonia - common from reflux of gastric juice into the proximal pouch and from the fistula itself
- Chest X-ray to evaluate pulmonary status
- Severe pneumonia may necessitate a staging procedure (gastrostomy under local anaesthesia first) and delay primary repair until lungs improve
Stabilisation Before Surgery
- Nil by mouth - stop all feeds
- Place a Replogle tube (double-lumen sump catheter) in the proximal esophageal pouch and apply continuous suction to prevent aspiration
- Head-up, prone position to reduce reflux into the airway
- IV access and fluid resuscitation: neonates are often dehydrated and malnourished
- Correct electrolyte imbalances
- IV antibiotics if aspiration pneumonia is present
Physiological Considerations Specific to Day-1 Neonate
- Transitional circulation may still be present (patent ductus arteriosus, patent foramen ovale)
- Immature thermoregulation - maintain strict normothermia (warm theatre, warm IV fluids, overhead heater, warm blankets)
- Immature hepatic and renal drug metabolism - reduce drug doses accordingly
- High closing capacity relative to FRC - prone to atelectasis
3. Intraoperative Anaesthetic Management
Monitoring
- Arterial line (pre-ductal - right radial preferred): mandatory for beat-to-beat BP monitoring; surgical retraction compresses great vessels and causes sudden desaturation/hypotension
- Pre-ductal AND post-ductal pulse oximetry (right hand + any foot): detects intracardiac shunting
- Precordial stethoscope: placed in the dependent (left) axilla to immediately detect main-stem bronchus obstruction from surgical retraction - a drop in breath sounds is an early warning
- ECG, temperature probe (rectal/oesophageal - not oesophageal in this case!), capnography
- Blood group and crossmatch - blood must be immediately available
Positioning
- Left lateral decubitus for right extrapleural thoracotomy (conventional open approach)
- VATS (video-assisted thoracoscopic surgery) is increasingly preferred and requires similar positioning
Induction - Three Accepted Strategies
| Technique | Approach | Key Point |
|---|---|---|
| Awake/minimally sedated intubation | Laryngoscopy with topical lidocaine spray, no relaxants | Protects airway, reduces aspiration risk; preferred in very sick neonates |
| Inhalational induction + spontaneous breathing | Sevoflurane mask induction, then topical lidocaine + intubate awake | Avoids PPV before tube placement; preferred standard |
| IV/inhalational induction + muscle relaxants | Standard RSI-like approach | Risk of gastric distention via fistula with PPV - only if fistula is small or gastrostomy is in place |
Avoid mask positive pressure ventilation (PPV) before intubation - air inflates the stomach via the fistula, causing gastric distention that compresses the diaphragm, reduces FRC, and worsens ventilation. This risk is greater with large fistulae or poor lung compliance.
Endotracheal Tube Placement - The Critical Step
The ideal position is the tip of the ETT distal to the fistula and proximal to the carina so that gas passes into the lungs, not the stomach.
Technique for blind correct placement:
- Advance the ETT until it enters a mainstem bronchus (unilateral chest rise, unilateral breath sounds)
- Slowly withdraw until bilateral equal breath sounds are confirmed
- The tip now lies just distal to the fistula (which opens just above the carina posteriorly)
Bronchoscopy: Ideally performed after induction to:
- Confirm fistula size and location
- A Fogarty balloon catheter may be placed directly into the fistula lumen to occlude it, enabling safer PPV
Pitfalls:
- The ETT may inadvertently enter the fistula - suspect if sudden gastric distention, increased difficulty ventilating, and desaturation occur. Surgeon can palpate the tip. Withdraw immediately.
- The fistula may connect to the carina or a mainstem bronchus - in this case correct positioning is impossible; intermittent venting of a gastrostomy tube is the workaround
Maintenance of Anaesthesia
- Inhalational agents (sevoflurane or isoflurane) in air/oxygen mixture
- Maintain spontaneous ventilation if possible until the fistula is ligated - this is the safest strategy to avoid fistula distention
- Once fistula is ligated, controlled ventilation is acceptable
- Use lowest PIP necessary with permissive hypercapnia to avoid barotrauma
- Opioids judiciously (morphine or fentanyl) - be mindful of respiratory depression in day-1 neonate
- Muscle relaxants (vecuronium or cisatracurium) after intubation confirmed correctly
- Maintain normothermia actively throughout
Gastrostomy Tube Management (if present)
- Leave open to air (not to suction) at the head of the table
- Anesthesiologist must ensure it does not kink
- Vent intermittently if gastric distention occurs during PPV
- Its presence makes controlled ventilation safer
Intraoperative Hazards
| Problem | Cause | Management |
|---|---|---|
| Sudden desaturation + gastric distention | ETT in fistula | Surgeon palpates tip; withdraw ETT |
| Sudden desaturation + loss of breath sounds | Surgical retraction of lung | Ask surgeon to reexpand lung |
| Hypotension | Compression of great vessels or heart | Surgeon releases retraction; volume bolus |
| Bradycardia | Vagal stimulation from mediastinal manipulation | Atropine IV; surgeon releases |
| Hypothermia | Large exposed thoracic cavity in day-1 neonate | Warm IV fluids, heated blanket, warmed gases |
4. Postoperative Management
- Extubation decision is coordinated with the surgeon - based on lung condition and adequacy of repair
- Most neonates with pre-existing aspiration pneumonia require continued postoperative ventilation with PEEP
- Neonates in good condition with no complications may be extubated early
- Avoid neck extension and esophageal suctioning - may disrupt anastomosis
- No nasogastric tube instrumentation without surgical clearance
- Continue monitoring in NICU
Postoperative Analgesia
- Wound infiltration with local anaesthetic (surgeon-applied)
- Caudal epidural catheter threaded to thoracic level - excellent for multimodal analgesia
- Paravertebral catheter at the surgical level
- Systemic opioids (IV morphine infusion) with apnoea monitoring - neonates are at high risk for opioid-induced apnoea
Postoperative Complications
- Gastroesophageal reflux and recurrent aspiration pneumonia
- Anastomotic leak
- Anastomotic stricture
- Recurrent fistula
- Tracheal compression from the repaired segment
5. Summary Checklist for the Anaesthesiologist
- Echocardiogram reviewed (CHD, arch sidedness)
- Replogle tube in pouch on continuous suction
- Arterial line (right radial) pre-induction or awake
- Blood crossmatched and available
- Theatre warmed, warm fluids, overhead heater
- Avoid mask PPV before correct ETT placement
- ETT tip distal to fistula - confirmed by auscultation bilaterally
- Bronchoscopy to assess fistula (Fogarty balloon if needed)
- Pre- and post-ductal SpO2 probes
- Precordial stethoscope on left (dependent) axilla
- Gastrostomy tube open to air if present
- Maintain spontaneous ventilation until fistula ligated
- Postoperative analgesia plan (caudal/paravertebral + local infiltration)
- Extubation decision coordinated with surgeon
Sources: Miller's Anesthesia 10e (pp. 10638-10639) | Morgan & Mikhail's Clinical Anesthesiology 7e (pp. 1715-1716) | Barash's Clinical Anesthesia 9e (pp. 3664-3666)
This is a shared conversation. Sign in to Orris to start your own chat.