residual post operative pneumoperitonium
Reading File
Finding Sources
Finding Sources
Searching PubMed
residual pneumoperitoneum postoperative
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have enough material from the textbooks to give a thorough, well-organized answer. Let me synthesize everything.
Residual Postoperative Pneumoperitoneum
Definition
Residual postoperative pneumoperitoneum refers to free intraperitoneal gas that persists in the abdominal cavity after laparoscopic (or open abdominal) surgery. It is a normal, expected finding after any procedure that requires peritoneal insufflation, and must be distinguished from pathological causes of free intraperitoneal air (e.g., bowel perforation, anastomotic leak).
Mechanism and Gas Kinetics
The gas used for laparoscopic insufflation is almost universally carbon dioxide (CO2). CO2 is chosen because it is:
-
Rapidly absorbed across the peritoneal membrane into the circulation
-
Highly soluble in blood (lowers the risk of gas embolism)
-
Rapidly excreted via the lungs
-
Colorless, odorless, inexpensive, and non-combustible
-
Hinman's Atlas of Urologic Surgery, p. PNEUOPERITONEUM section
Despite active desufflation at the end of surgery, a variable amount of CO2 remains trapped between loops of bowel and under the diaphragm. This residual gas:
-
Is absorbed progressively over 24-72 hours in most patients
-
Can persist longer depending on the volume insufflated, duration of surgery, and patient's peritoneal surface area and respiratory reserve
-
Nitrogen-containing air, if used historically, is absorbed far more slowly (nitrogen is poorly soluble in blood), which is why CO2 replaced air as the standard insufflant
-
Schwartz's Principles of Surgery 11e, p. Laparoscopy section
Clinical Significance and Symptoms
1. Shoulder Tip Pain (Most Common Symptom)
The most characteristic symptom of residual pneumoperitoneum is referred shoulder tip pain, typically right-sided but can be bilateral.
Mechanism: The diaphragm develops from the C3-C5 dermatomal level. Residual subdiaphragmatic CO2 irritates the parietal peritoneum beneath the diaphragm, causing pain to be referred along the phrenic nerve to the C4/C5 dermatome at the shoulder tip (same mechanism as subphrenic abscess-related shoulder pain).
"This also explains why patients frequently complain of shoulder tip pain following laparoscopic or robotic surgery." - Bailey and Love's Short Practice of Surgery 28e
CO2 itself is mildly acidic (forms carbonic acid), adding a chemical irritant component on top of the mechanical distension effect.
2. Upper Abdominal Discomfort
Bloating, fullness, and vague upper abdominal discomfort from peritoneal distension.
3. Pleuritic-Type Chest Discomfort
Occasionally patients experience mild chest or lower rib cage pain, especially on deep inspiration, from diaphragmatic irritation.
4. Nausea
Peritoneal irritation from residual gas may worsen postoperative nausea and vomiting (PONV), which is already elevated in laparoscopic procedures - particularly laparoscopic cholecystectomy.
- Barash Clinical Anesthesia 9e, p. Postoperative Management
Radiology
On chest X-ray or abdominal X-ray, residual pneumoperitoneum appears as:
- Free air under the right hemidiaphragm (most common) - a crescentic lucent shadow
- Can be bilateral
Important distinction: In a postoperative patient, free subdiaphragmatic air is expected up to 3-7 days after laparoscopy (or longer after open surgery). The amount normally decreases on serial films. Persistence or increase in free air after day 3-5 should raise suspicion for:
- Anastomotic leak
- Bowel perforation (missed or new)
- Ongoing enteric fistula
CT scan is more sensitive and can quantify the volume, identify loculations, and help detect underlying complications.
Risk Factors for Prolonged or Symptomatic Residual Pneumoperitoneum
| Factor | Effect |
|---|---|
| Longer operative duration | More CO2 absorbed into tissues, released post-op |
| Higher intra-abdominal pressure (IAP) used | Greater volume instilled |
| Steeper Trendelenburg positioning | Gas pools subdiaphragmatically |
| Incomplete desufflation at end of case | Obvious residual volume |
| Abdominal adhesions | Gas trapping in loculated spaces |
| Obese patients | Larger cavity, longer absorption |
Prevention
Surgical techniques that reduce the severity of residual pneumoperitoneum and associated pain include:
- Lower insufflation pressure (IAP) - use the minimum pressure needed (typically 8-12 mmHg rather than 15 mmHg)
- Active evacuation of subdiaphragmatic CO2 before wound closure - placing the patient in the Trendelenburg position and manually compressing the abdomen while ports are still open
- Shorter duration of pneumoperitoneum (efficient surgery)
- Intraperitoneal saline instillation (dilutes CO2, some evidence it reduces shoulder tip pain)
- Aspiration of residual gas through a port before final removal
- Barash Clinical Anesthesia 9e: "A number of surgical techniques during laparoscopy can reduce the severity of postoperative pain. These include the use of lower IAP, shorter duration of pneumoperitoneum, and evacuation of subdiaphragmatic CO2 prior to wound closure."
Management of Symptoms
| Symptom | Management |
|---|---|
| Shoulder tip pain | NSAIDs / COX-2 inhibitors, paracetamol (acetaminophen), reassurance that it resolves spontaneously in 24-72 h |
| Nausea | Antiemetics (ondansetron, dexamethasone) |
| Abdominal discomfort | Analgesia, early mobilization |
| Severe or persistent symptoms | CT abdomen to exclude pathological cause |
When to Be Concerned (Red Flags)
Residual pneumoperitoneum becomes pathological when accompanied by:
- Fever, tachycardia, peritonism - suggest anastomotic leak, bowel injury, or abscess
- Increasing free air on serial imaging (rather than decreasing)
- New onset of symptoms after an initial asymptomatic period (day 3-5 post-op)
- Port-site tenderness with ileus on day 2-3 - consider bowel entrapment at port site (requires re-exploration)
"If missed during the process of cannula removal, then in the early postoperative period, usually on the second or third postoperative day, the patient may develop an ileus and point tenderness at the port site incision. The treatment is operative." - Campbell Walsh Wein Urology
Summary
Residual postoperative pneumoperitoneum is a normal, self-limiting finding after laparoscopic surgery, caused by retained CO2 that is progressively absorbed over 1-4 days. The dominant clinical manifestation is shoulder tip pain from referred phrenic nerve irritation. Management is supportive with NSAIDs and reassurance. The key clinical task is to distinguish benign residual gas (diminishing over time, no systemic features) from pathological free air (persistent or increasing, with fever, peritonism, or hemodynamic instability), which signals a surgical complication requiring urgent investigation and possible re-intervention.
38 year female came with history of fever for 12 days joint pain and rash developed after 4-5 days of fever vital were normal
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive material. Let me compile the full clinical analysis.
38F: Fever 12 Days + Joint Pain + Rash (Day 4-5)
Clinical Summary
| Feature | Detail |
|---|---|
| Age / Sex | 38-year-old female |
| Fever duration | 12 days |
| Rash onset | Day 4-5 of fever |
| Vitals | Normal |
| Joint pain | Present |
The sequence matters: fever first, then rash and joint pain. This pattern is most consistent with a systemic inflammatory or infectious/post-infectious process rather than a primary rheumatologic condition where arthritis usually precedes or coincides with fever onset.
Differential Diagnosis
1. Adult-Onset Still's Disease (AOSD) - Top Differential
AOSD is a systemic inflammatory disorder with a bimodal age distribution - peaks at 15-25 years and 36-46 years - which fits this patient exactly.
Classic triad:
- High spiking fever (≥39°C), quotidian (once daily) or double-quotidian (twice daily)
- Salmon-pink evanescent maculopapular rash - characteristically appears when the patient is febrile and disappears when afebrile
- Arthralgia / arthritis (knees, wrists, ankles, elbows - DIP joints also involved, which is unusual)
Additional features:
- Nonsuppurative pharyngitis (sore throat)
- Lymphadenopathy, hepatosplenomegaly
- Leukocytosis (neutrophilic)
- Markedly elevated serum ferritin (often >2000 ng/mL) - characteristic and diagnostically helpful
- Can present as fever of unknown origin (FUO) in up to 10% of cases
"AOSD is a systemic inflammatory disorder of unknown etiology. It occurs worldwide and is associated with a bimodal age distribution with peaks between the ages 15-25 years and 36-46 years. The rash often appears when the patient is febrile and disappears during afebrile periods." - Frameworks for Internal Medicine
Yamaguchi Criteria for AOSD (5 or more criteria required, with at least 2 major):
| Major Criteria | Minor Criteria |
|---|---|
| Fever ≥39°C, lasting ≥1 week | Sore throat |
| Arthralgia ≥2 weeks | Lymphadenopathy |
| Typical rash (salmon-colored, evanescent) | Hepatomegaly or splenomegaly |
| WBC ≥10,000 with ≥80% PMNs | Abnormal LFTs |
| RF and ANA negative |
Exclusions: infections, malignancy, other rheumatic disease.
2. Parvovirus B19 Infection - Strong Contender
Particularly relevant in a woman of reproductive age.
Features:
- Prodrome of fever, malaise, headache, myalgia lasting several days - then rash and arthritis appear (mirrors this case exactly)
- Symmetric polyarthritis - elbows, wrists, knees, ankles, feet
- Peripheral macular rash lasting 2-3 days; multiple morphologies described
- Arthropathy occurs in ~30% of adult infections; rash in ~35%
- Important trap: ANA can be transiently elevated - can mimic SLE
- Both parvovirus and SLE are more common in women - differentiation requires parvovirus IgM serology
Diagnosis: Parvovirus-specific IgM antibody in serum
Treatment: NSAIDs; self-limiting - most resolve within weeks, ~10% persist longer
"Parvovirus clearly fits this patient's presentation... She was treated with NSAIDs with good relief of her symptoms. Her rash resolved over 3-4 days, and joint pain was gone at a follow-up visit 2 weeks later." - Symptom to Diagnosis, 4th Edition
3. Systemic Lupus Erythematosus (SLE) - Must Not Miss
- More common in women (9:1), peak reproductive age
- Fever, arthritis/arthralgia, and rash (malar butterfly rash, photosensitive)
- Leukopenia, ANA positive, anti-dsDNA (specific), low complement
- Diagnosis requires ≥4 of 11 ACR criteria (or SLICC criteria)
- Must be excluded before diagnosing AOSD or viral arthritis
- Key distinction: ANA in SLE is persistently positive and at high titer; in parvovirus B19 it is transient
4. Acute Rheumatic Fever (ARF) - Must Not Miss
- Fever then migratory polyarthritis (large joints - knees, ankles, hips, elbows)
- Erythema marginatum (ring-shaped rash, trunk and limbs, not face) - appears with fever
- Other Jones criteria: carditis, Sydenham's chorea, subcutaneous nodules
- Highly responsive to NSAIDs/aspirin (characteristic)
- Requires evidence of preceding GAS infection: elevated ASO/anti-DNase B, positive throat culture
"Arthritis in acute rheumatic fever is classically asymmetric, migratory, and inflammatory, affecting the large joints most frequently. It is highly responsive to salicylates and other NSAIDs." - Frameworks for Internal Medicine
5. Viral Arthritis - Other Causes
| Virus | Clue |
|---|---|
| Chikungunya | Travel to endemic region; severe, often crippling polyarthralgia; can persist months |
| Dengue | Travel history; severe bone pain ("breakbone fever"); thrombocytopenia |
| Rubella / post-vaccination | Rash + arthritis; vaccination history |
| Hepatitis B | Arthritis may precede jaundice; elevated transaminases |
| HIV seroconversion | Risk factors; mononucleosis-like illness |
| EBV/CMV | Mononucleosis syndrome; lymphadenopathy, pharyngitis |
6. Reactive Arthritis (ReA)
- Arthritis occurring 1-4 weeks after enteric (Salmonella, Shigella, Yersinia, Campylobacter) or urogenital (Chlamydia) infection
- Classic triad: arthritis + urethritis + conjunctivitis (Reiter's syndrome)
- Rash: keratoderma blennorrhagica (palms/soles), circinate balanitis
- Ask about preceding GI illness or urogenital symptoms
Approach to This Patient
History to Elicit
- Character of fever: Is it spiking and quotidian? Does the rash appear only with fever spikes? (AOSD)
- Rash description: Salmon-pink and evanescent vs. malar butterfly vs. erythema marginatum vs. maculopapular peripheral
- Joint pattern: Migratory (ARF) vs. symmetric (parvovirus) vs. additive (AOSD)
- Throat soreness (AOSD, ARF)
- Travel history (dengue, chikungunya)
- Contact with children (parvovirus B19)
- Prior GAS infection (ARF)
- GI/urogenital symptoms (reactive arthritis)
- Photosensitivity, oral ulcers, hair loss (SLE)
- Drug history (drug-induced lupus, serum sickness)
Investigations (First-Line)
| Test | Looking For |
|---|---|
| CBC with differential | Leukocytosis (AOSD, bacterial), leukopenia (SLE), thrombocytopenia (dengue) |
| Serum ferritin | Markedly high (>2000 ng/mL) strongly supports AOSD |
| ESR, CRP | Inflammatory marker elevation |
| ANA, anti-dsDNA, complement (C3/C4) | SLE |
| RF, anti-CCP | RA |
| Parvovirus B19 IgM | Viral arthritis |
| ASO titre, anti-DNase B | Preceding streptococcal infection (ARF) |
| Blood cultures | Bacterial endocarditis, gonococcal arthritis |
| LFTs | Hepatitis, AOSD |
| Dengue NS1 Ag + IgM/IgG | If travel history |
| Chikungunya serology | If travel to endemic area |
| Urine analysis | Renal involvement (SLE, AOSD) |
ECG / Echo
If carditis suspected (ARF, SLE), obtain ECG and consider echo.
Summary: Most Likely Diagnoses in Order
- Parvovirus B19 - fever preceding rash + arthritis by days, symmetric polyarthritis, female in reproductive age group - classically fits
- Adult-Onset Still's Disease - 38-year age peak, quotidian fever, evanescent salmon rash with fever spikes, markedly elevated ferritin
- SLE - female, rash + arthritis + fever; must be excluded with ANA/anti-dsDNA
- Acute Rheumatic Fever - if migratory large-joint arthritis and preceding sore throat
- Viral arthritis (dengue/chikungunya) - if travel history present
The key discriminator is the serum ferritin (very high = AOSD), parvovirus B19 IgM (positive = viral arthritis), and ANA/anti-dsDNA (SLE). The pattern of fever (quotidian, rash coinciding with fever spikes) points toward AOSD in a 38-year-old female, while a prodrome followed by symmetric small-joint arthritis + rash points toward parvovirus B19.
- Symptom to Diagnosis, 4th Edition
- Frameworks for Internal Medicine
- Goldman-Cecil Medicine
- Dermatology 2-Volume Set 5e
Renal cell carcinoma diagonosis
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Excellent - I have the TNM staging diagram and all the key clinical content. Now I'll compile the comprehensive answer.
Renal Cell Carcinoma (RCC) - Diagnosis
Epidemiology
- ~81,000 new cases/year in the United States; ~15,000 deaths/year
- 7th most common cancer overall; 6th in males, 9th in females
- Male : Female ratio ~2:1
- Peak incidence: 55-75 years
- Incidence highest in Black Americans; lowest in Asian/Pacific Islanders
- Only 4-6% of cases are familial; the majority are sporadic
Risk Factors:
| Modifiable | Non-Modifiable |
|---|---|
| Cigarette smoking (20-30% of cases; dose-dependent) | Male sex |
| Obesity (risk rises with BMI) | Age (6th-7th decade) |
| Hypertension | Black race |
| Acquired renal cystic disease (dialysis patients) | VHL syndrome / hereditary syndromes |
| Occupational: aromatic hydrocarbons, asbestos, cadmium | Polycystic kidney disease |
- Goldman-Cecil Medicine; Harrison's Principles 22e; Sabiston Textbook of Surgery
Histological Classification
RCC is not one disease - it is a group of distinct entities:
| Subtype | Frequency | Chromosome/Gene | Key Features |
|---|---|---|---|
| Clear cell RCC | 65-80% | 3p deletion / VHL gene | Most aggressive; golden-yellow gross appearance; accounts for ~90% of metastases; HIF-1/VEGF pathway driven |
| Papillary RCC | 10-15% | Trisomy 7, 17; MET proto-oncogene | Often multifocal; two types (type 1 = MET mutation; type 2 = more aggressive) |
| Chromophobe RCC | 5% | Multiple chromosomal losses | More indolent; eosinophilic cytoplasm with perinuclear haloes; tan-brown gross appearance |
| Collecting duct carcinoma | <1% | - | Aggressive; arises from Bellini's ducts |
| Oncocytoma | ~10% | - | Benign; mahogany-brown; cannot reliably distinguish from RCC on imaging alone |
"The metastatic potential depends on the histologic subtype and ranges from the most virulent conventional clear cell carcinomas (65% of total tumors but accounting for 90% of the metastases), to the more indolent papillary and chromophobe carcinomas (25% of the total but only 10% of the metastases)." - Goldman-Cecil Medicine
Hereditary Syndromes Associated with RCC
| Syndrome | Gene | Chromosome | Tumor Type |
|---|---|---|---|
| Von Hippel-Lindau (VHL) | VHL | 3p25 | Clear cell (70% lifetime risk) |
| Hereditary papillary RCC | MET | 7p31 | Papillary (bilateral, multifocal) |
| Birt-Hogg-Dubé | FLCN (folliculin) | 17p11 | Chromophobe / oncocytoma; also lung cysts, fibrolisticulomas |
| Hereditary leiomyomatosis RCC (HLRCC) | FH (fumarate hydratase) | 1q42 | FH-deficient RCC; uterine leiomyomas |
| Tuberous sclerosis | TSC1/TSC2 | 9q34/16p13 | Angiomyolipomas; rare RCC |
| BAP1 tumor predisposition | BAP1 | 3p21 | Mostly clear cell; uveal melanoma, mesothelioma |
- Harrison's Principles of Internal Medicine 22e
Clinical Presentation
Classic Triad (Virchow's Triad of RCC)
- Flank/costovertebral pain
- Gross hematuria
- Palpable flank/abdominal mass
This classic triad is present in only 5-10% of cases and usually indicates advanced, locally advanced disease.
Incidental Discovery
- >50% of RCC is now discovered incidentally on imaging (CT/ultrasound) performed for unrelated reasons
- Despite this, 30% of patients still present with metastatic disease
Symptoms at Advanced Presentation
- Hematuria (most reliable clinical clue - may be intermittent or microscopic)
- Constitutional symptoms: fever, fatigue, weight loss, malaise
- Symptoms of metastasis: pathologic fracture, cough, hemoptysis, neurological symptoms
Paraneoplastic Syndromes (present in ~20% at diagnosis)
RCC is one of medicine's great mimics - it produces a wide variety of syndromes from ectopic hormone production:
| Syndrome | Mechanism |
|---|---|
| Polycythemia | Ectopic erythropoietin production |
| Hypercalcemia | PTHrP secretion |
| Hypertension | Renin secretion |
| Stauffer syndrome | Reversible hepatic dysfunction without liver metastasis (elevated LFTs, ALP) |
| Anemia | Chronic disease |
| Cushing syndrome | Ectopic ACTH |
| Feminization / masculinization | Sex hormone production |
| Elevated ESR / CRP | Inflammatory cytokines |
| Eosinophilia / leukemoid reaction | Cytokine release |
| Amyloidosis | Chronic inflammation |
"Renal cell carcinoma is considered one of the great mimics in medicine, because it tends to produce a diversity of systemic symptoms not related to the kidney." - Robbins Cotran Kumar Pathologic Basis of Disease
Diagnostic Workup
Step 1 - Initial Labs
| Test | Purpose |
|---|---|
| CBC | Polycythemia (Hct↑) or anemia |
| Serum creatinine / eGFR | Baseline renal function; guides partial vs. radical nephrectomy decision |
| LFTs + ALP | Stauffer syndrome; hepatic metastases |
| Serum calcium | Paraneoplastic hypercalcemia |
| LDH | Prognostic marker in metastatic disease |
| ESR, CRP | Elevated in paraneoplastic inflammation |
| Urinalysis | Hematuria (micro or macroscopic) |
Step 2 - Imaging
Ultrasound
- First step for evaluating a renal mass
- Distinguishes simple cysts (benign) from solid masses
- Low sensitivity for small lesions
- Solid or complex cystic lesion on US → proceed to CT/MRI
Contrast-Enhanced CT (CECT) - Primary Diagnostic Modality
- Preferred imaging modality for characterizing renal masses
- Four phases: precontrast → arterial (~25 sec) → nephrographic (~90 sec) → excretory
- Key findings: enhancement on contrast (>15 HU increase) = malignant until proven otherwise
- Evaluates: tumor size, local extension, renal vein and IVC thrombus (critical for staging), regional lymph nodes, adrenal glands
- Macroscopic fat in a solid mass → angiomyolipoma (benign)
- CT chest for pulmonary metastases
Enhancement patterns by subtype:
- Clear cell RCC: avid enhancement in corticomedullary phase, then hypoenhancing in nephrographic phase ("washout")
- Chromophobe RCC: avid enhancement, but less than clear cell; central scar
- Papillary RCC: hypointense on T2-MRI; hypoenhancing on all phases (hypovascular)
MRI
- Similar diagnostic yield to CT for solid masses
- Superior for: IVC/renal vein thrombus assessment, complex cystic lesions (subtraction imaging detects subtle enhancement), patients with contrast allergy or poor renal function
- MRI angiography: maps renal artery anatomy pre-operatively for partial nephrectomy
Contrast-Enhanced Ultrasound (CEUS)
- New, inexpensive; non-nephrotoxic contrast (microbubbles)
- Clear cell RCC: avid early enhancement + pseudocapsule + early washout
- Useful in patients with reduced GFR
Bone Scan
- Indicated in: clinically advanced disease, bone pain, hypercalcemia, elevated ALP
- Not routine for localized disease
Brain MRI
- Indicated when neurological symptoms are present or clinically suspected metastases
Step 3 - Bosniak Classification for Cystic Renal Masses
| Category | CT Features | Malignancy Risk | Management |
|---|---|---|---|
| I | Simple cyst, smooth wall, no septa, no enhancement | 0% | No follow-up |
| II | Few thin septa, minimal calcification, no enhancement | <5% | No follow-up |
| IIF | Multiple thin septa, slight wall thickening, minimal enhancement | 5-15% | Follow-up imaging at 6, 12 months then annually x5 years |
| III | Thickened irregular walls/septa, measurable enhancement | ~50% | Surgical exploration |
| IV | Solid enhancing components, shaggy margins | 70-90% | Treat as malignant - surgical resection |
"Category III and IV cysts are usually treated as representing renal cell carcinomas." - Sabiston Textbook of Surgery
Step 4 - Renal Mass Biopsy
When is biopsy used?
- Increasingly used before ablative therapy or active surveillance to confirm histology
- Before starting systemic therapy for unresectable/metastatic disease (tissue confirmation required)
- When imaging is equivocal and a benign diagnosis (e.g., lymphoma, metastasis from another primary) would change management
Limitations:
- Diagnostic accuracy ~90% for solid masses
- Not routinely done for cystic lesions (poor yield, sampling error, risk of spillage)
- Non-diagnostic in ~10-15% (may require repeat or surgical excision)
- Needle tract seeding is rare but reported
TNM Staging (AJCC)
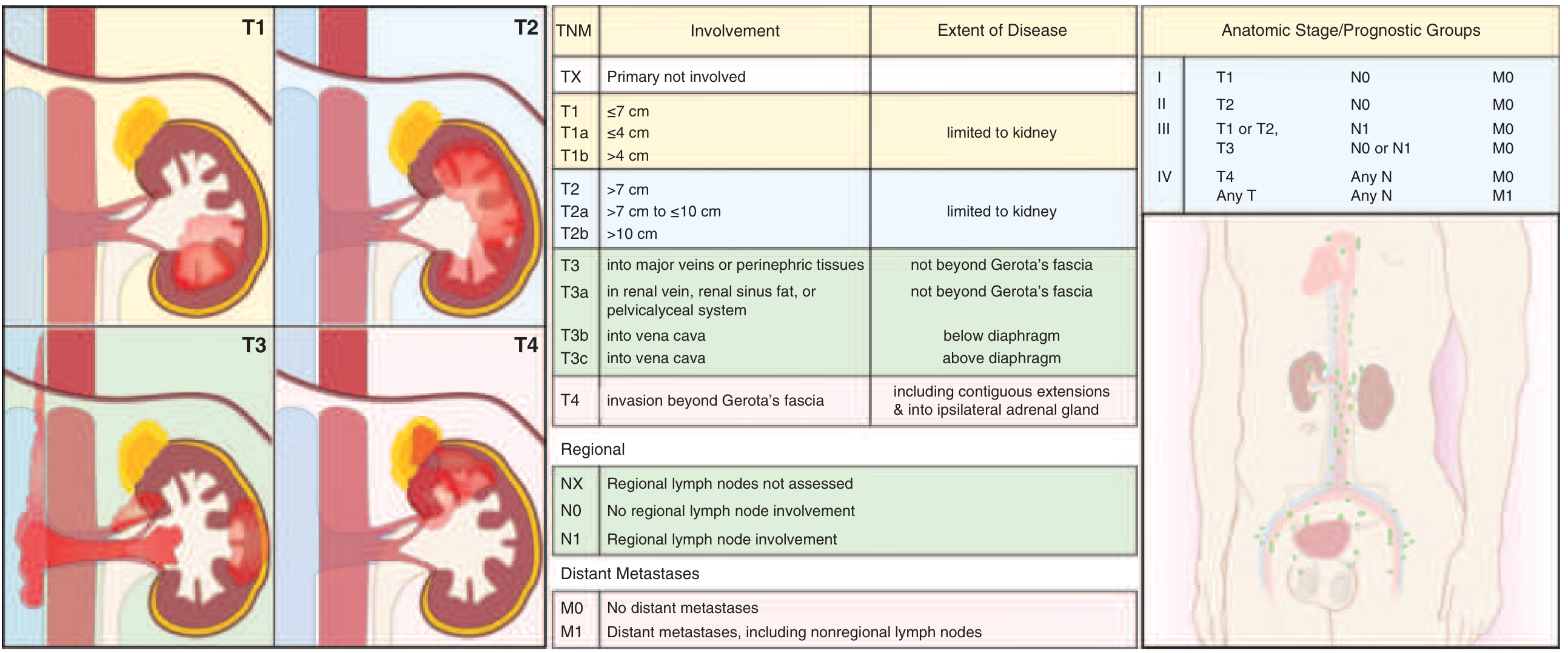
| T Stage | Description |
|---|---|
| T1a | ≤4 cm, limited to kidney |
| T1b | >4 to ≤7 cm, limited to kidney |
| T2a | >7 to ≤10 cm, limited to kidney |
| T2b | >10 cm, limited to kidney |
| T3a | Into renal vein, renal sinus fat, or pelvicalyceal system (not beyond Gerota's fascia) |
| T3b | Into vena cava below diaphragm |
| T3c | Into vena cava above diaphragm |
| T4 | Beyond Gerota's fascia; ipsilateral adrenal invasion |
| N Stage | Description |
|---|---|
| N0 | No regional lymph node involvement |
| N1 | Regional lymph node involvement |
| M Stage | Description |
|---|---|
| M0 | No distant metastases |
| M1 | Distant metastases (lungs >50%, bone 33%, lymph nodes, liver, adrenal, brain) |
Stage Groups:
- Stage I: T1, N0, M0
- Stage II: T2, N0, M0
- Stage III: T1/T2 N1 M0, or T3 any N M0
- Stage IV: T4 any N M0, or any T any N M1
Histologic Grading
The WHO/ISUP grading system (replacing older Fuhrman system) grades on nuclear size, irregularity, and nucleolar prominence:
- Grade 1-2: Low grade (favorable)
- Grade 3-4: High grade (grade 4 includes sarcomatoid/rhabdoid differentiation)
Prognosis
| Stage | 5-Year Survival |
|---|---|
| Localized (no metastases) | ~100% (T1) / ~70% overall |
| Renal vein invasion / perinephric fat extension | ~60% |
| Metastatic (Stage IV) | ~12-15% (dramatically improved with immunotherapy + TKI combinations) |
Key prognostic factors:
- Histologic subtype (clear cell worst, chromophobe best)
- Nuclear grade (Fuhrman/WHO-ISUP)
- Stage (T, N, M)
- Performance status
- Presence of sarcomatoid differentiation (very poor prognosis)
Summary Diagnostic Algorithm
Renal mass found (incidental or symptomatic)
↓
Ultrasound
↓
Simple cyst? → No follow-up
Solid/complex? → CECT abdomen/pelvis + CT chest
↓
Bosniak I-II → follow-up
Bosniak III-IV → treat as malignant → surgical planning
Solid enhancing mass → stage with TNM
↓
If biopsy needed → percutaneous core biopsy (before ablation/surveillance/systemic therapy)
↓
Labs: CBC, CMP, LFTs, Ca2+, LDH, UA
Bone scan if: bone pain, hypercalcemia, elevated ALP
Brain MRI if: neurological symptoms
- Robbins Cotran & Kumar Pathologic Basis of Disease
- Harrison's Principles of Internal Medicine 22e
- Goldman-Cecil Medicine
- Campbell Walsh Wein Urology
- Sabiston Textbook of Surgery
- National Kidney Foundation Primer on Kidney Diseases 8e
This is a shared conversation. Sign in to Orris to start your own chat.