SVT
Reading File
Finding Sources
Finding Sources
Searching PubMed
"supraventricular tachycardia" AND management
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive information. Let me compile the full SVT overview.
Supraventricular Tachycardia (SVT)
Definition
SVT is a broad term for any tachyarrhythmia that originates at or above the bundle of His (i.e., in the atria, AV node, or AV junctional tissue). The term is often used specifically to mean paroxysmal SVT (PSVT) - a group of regular, narrow-complex tachycardias that arise suddenly and terminate abruptly.
Classification
| Type | Mechanism | Frequency |
|---|---|---|
| AVNRT (AV Nodal Reentrant Tachycardia) | Reentry within the AV node using dual pathways | ~80% of PSVT |
| AVRT (AV Reentrant Tachycardia) | Reentry using an accessory pathway (e.g., WPW) | ~15-20% |
| Atrial Tachycardia | Ectopic atrial focus or intra-atrial reentry | Remaining cases |
| Atrial flutter | Macro-reentry in right atrium | Common, usually regular |
| Atrial fibrillation | Multiple reentrant wavelets | Most common arrhythmia overall |
| Junctional tachycardia | Automatic or triggered focus in AV junction | Rare in adults |
AVNRT - The Prototype
Mechanism: The AV node has two functionally distinct pathways:
- Fast pathway: fast conduction, long refractory period
- Slow pathway: slow conduction, short refractory period
In typical (slow/fast) AVNRT (85-90% of cases): A premature atrial beat finds the fast pathway refractory, conducts down the slow pathway, and then re-enters via the fast pathway retrogradely, establishing a reentrant circuit. The atria and ventricles are activated simultaneously.
In atypical AVNRT: Fast/slow (fast antegrade, slow retrograde) or slow/slow variants account for the remaining 10-15%.
- Fuster and Hurst's The Heart, 15th Ed, p.1127-1128
ECG Features of PSVT
| Feature | Finding |
|---|---|
| Rate | 130-300 bpm (typically 170-180 bpm) |
| Rhythm | Regular |
| QRS | Narrow (<100 ms) unless aberrancy |
| P waves | "Buried" in QRS (~70%); retrograde P immediately before/after QRS (~30%) |
| RP interval | Short RP (RP < PR) in typical AVNRT; Long RP (RP ≥ PR) in atypical AVNRT / AT |
Differential diagnosis based on RP interval:
-
Short RP (RP < PR): Typical AVNRT, AVRT
-
Long RP (RP ≥ PR): Atypical AVNRT, atrial tachycardia, PJRT (permanent junctional reciprocating tachycardia), sinus tachycardia
-
Tintinalli's Emergency Medicine, Table 18-16
Clinical Presentation
-
More common in females, peak in late teens/young adults
-
Most patients have no structural heart disease
-
Abrupt onset and offset - patients can often identify when it starts and terminates
-
Symptoms: palpitations, lightheadedness, dyspnea, near-syncope
-
Can cause syncope if rates are very high or vasomotor instability occurs
-
In children: rate >220 bpm (infants) or >180 bpm (older children) suggests SVT over sinus tachycardia
-
Tintinalli's Emergency Medicine, p.153
Acute Management
Treatment algorithm (hemodynamically stable narrow-complex tachycardia):
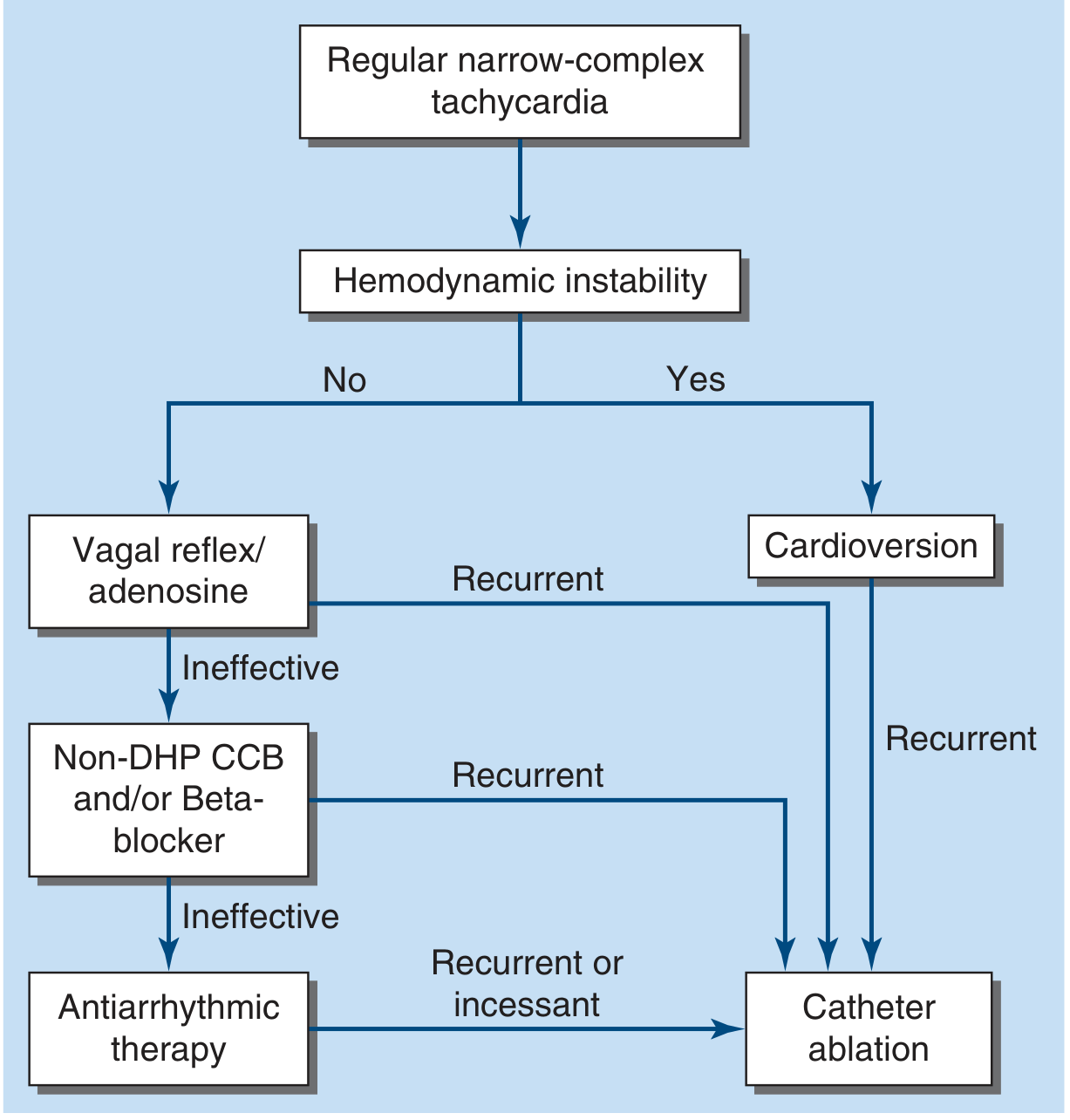
Step 1: Hemodynamic instability?
- Yes → Synchronized DC cardioversion (QRS-synchronous)
- No → proceed to vagal maneuvers
Step 2: Vagal Maneuvers
- Valsalva maneuver (first line, patient can self-administer)
- Carotid sinus massage (check for carotid bruits first; avoid if prior stroke)
- Face immersion in ice water (especially in children)
- A 2025 network meta-analysis (PMID 41380061) is evaluating optimal vagal maneuver techniques
Step 3: Adenosine (drug of choice)
- 6 mg IV rapid bolus → if ineffective, 12 mg IV (repeat once)
- Must be followed immediately by NS flush
- Nearly 100% effective for AVNRT
- Mechanism: transient AV nodal blockade via A1 purinergic receptors
- Cautions:
- Cardiac transplant recipients: very sensitive - start at 1 mg
- WPW with pre-excited AF: avoid (can accelerate conduction down accessory pathway)
- Asthma: caution (may trigger bronchospasm)
- Theophylline/caffeine: antagonize effect (higher doses may be needed)
- Dipyridamole: potentiates effect
- Side effects: transient chest pain, flushing, dyspnea, sinus bradycardia, may precipitate AF (in up to 15%)
Step 4: AV Nodal Blocking Agents (if adenosine fails or tachycardia recurs)
- Verapamil IV (non-DHP CCB): slows both fast and slow pathways
- Diltiazem IV
- Beta-blockers IV (metoprolol, esmolol)
- Note: may cause hypotension; avoid in patients with systolic dysfunction
Step 5: Wide-complex tachycardia (SVT with aberrancy vs VT)
-
Treat as VT until proven otherwise
-
If regular, stable, adenosine trial is reasonable (may reveal SVT with aberrancy)
-
Irregular wide-complex tachycardia: likely pre-excited AF - treat with cardioversion, procainamide, or ibutilide (do NOT use adenosine/verapamil)
-
Harrison's Principles of Internal Medicine 22E (2025), p.1986
-
Fuster and Hurst's The Heart, 15th Ed, p.1129-1130
Long-term / Chronic Management
| Approach | Details |
|---|---|
| Catheter ablation | First-line for recurrent/symptomatic PSVT; >95% success for AVNRT slow-pathway ablation; preferred over lifelong drug therapy |
| Beta-blockers or CCBs (oral) | Rate control; can take "pill-in-pocket" (e.g., verapamil) to terminate acute episodes |
| Antiarrhythmic drugs | Flecainide, propafenone (class IC) for patients not candidates for ablation |
| Observation | For infrequent, well-tolerated, self-terminating episodes |
Most patients with recurrent PSVT are candidates for catheter ablation, which is curative. - Harrison's Principles of Internal Medicine 22E (2025), p.1986
VT vs SVT with Aberrancy - Key Differentiators
| Feature | VT | SVT with Aberrancy |
|---|---|---|
| AV dissociation | Present (strongly favors VT) | Absent |
| Fusion/capture beats | Present | Absent |
| QRS in tachycardia = QRS in sinus | Unlikely | Likely (same morphology) |
| Response to adenosine | Transient VA dissociation if 1:1 VA conduction | Terminates or exposes mechanism |
| Concordance in V1-V6 | Positive or negative | Unusual |
- Braunwald's Heart Disease, Textbook of Cardiovascular Medicine, p.553-554
Special Situations
| Situation | Notes |
|---|---|
| WPW syndrome | Accessory pathway enables pre-excitation; avoid AV nodal blockers (adenosine, verapamil) in pre-excited AF; use procainamide or cardioversion |
| Pregnancy | Adenosine is safe; electrical cardioversion is safe; avoid beta-blockers and CCBs in first trimester if possible |
| Children | Adenosine preferred; check Harriet Lane dosing; consider accessory pathways (Ebstein's anomaly, corrected TGA) |
| Post-cardiac transplant | Exquisite adenosine sensitivity; start at 1 mg |
Recent Evidence
- A 2025 network meta-analysis (PMID 41380061) compared vagal maneuver techniques for stable SVT, evaluating optimal first-line non-pharmacologic approaches.
- A 2024 systematic review/meta-analysis (PMID 39242347) examined troponin elevation in SVT patients - relevant for distinguishing demand ischemia from true ACS in patients presenting with SVT.
Sources: Harrison's Principles of Internal Medicine 22E (2025) | Fuster and Hurst's The Heart, 15th Ed | Tintinalli's Emergency Medicine | Braunwald's Heart Disease | Tintinalli's (Pediatric) | Creasy & Resnik's Maternal-Fetal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.