Ct simulation of prostate cancer
Reading File
Finding Sources
Finding Sources
Searching the Web
CT simulation prostate cancer radiation therapy planning protocol 2024
Finding Sources
Reading Web Page
https://acsearch.acr.org/docs/69396/Narrative
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive overview of CT simulation for prostate cancer:
CT Simulation for Prostate Cancer
CT simulation is the foundational step in external beam radiation therapy (EBRT) planning for prostate cancer. It replaces the older technique of using skeletal landmarks and contrast-filled catheters/rectal tubes to infer prostate location - a method shown to produce a 53% error rate in field placement. CT allows direct visualization of the prostate and accurate dose calculation to both the target and surrounding organs.
1. Purpose of CT Simulation
CT simulation accomplishes four goals:
- Localizes the prostate (and seminal vesicles) within the pelvis
- Defines target volumes (GTV, CTV, PTV)
- Identifies organs at risk (OARs): rectum, bladder, femoral heads, bowel, penile bulb, sigmoid colon
- Provides electron density data for accurate dose calculation (tissue inhomogeneity corrections for bone, air, soft tissue)
2. Patient Preparation
Proper preparation is essential because organ filling directly affects prostate position and dosimetry:
Bowel Preparation
- Low-fiber diet for 48 hours before simulation (avoid fresh fruits, vegetables, whole grains, nuts, seeds)
- Laxative (e.g., bisacodyl/Dulcolax) the night before - optional but recommended
- Fleet enema on the morning of simulation
- Simethicone (Gas-X) to reduce bowel gas
- Rationale: a grossly distended rectum at simulation results in worse dosimetry and clinical outcomes. Planning on a distended rectum image is generally not recommended; resimulation should be considered
Bladder Protocol
- Full bladder at simulation - patients typically drink a set volume of water 30-60 minutes before the scan
- A comfortably full (not over-full) bladder pushes bowel loops out of the treatment field and reduces the proportion of bladder receiving high dose
3. Patient Positioning and Immobilization
The position used at simulation must be reproduced exactly at every treatment fraction. Two main positions are used:
| Position | Advantages | Disadvantages |
|---|---|---|
| Supine | More comfortable, more reproducible, better tolerance | Posterior rectum closer to prostate |
| Prone (with belly board) | Displaces bowel anteriorly and inferiorly | Less reproducible, worse for organ motion |
Immobilization devices include:
- Knee support / leg positioner (alpha cradle, Vac-Lok bag)
- Foot stocks to fix leg position
- Rectal balloon - an endorectal balloon inflated inside the rectum displaces the posterior rectal wall away from the prostate, reduces rectal volume in the high-dose region, and immobilizes the prostate to reduce interfraction motion (see Fig. 157.4 reference in Campbell-Walsh)
4. CT Acquisition Parameters
- Slice thickness: 3-5 mm (standard) - allows resolution of prostatic apex to within 2-3 CT slices
- Field of view: extends from above the iliac crests (to include pelvic nodes if needed) to the perineum
- IV contrast: optional; can help delineate pelvic vasculature and lymph nodes
- Bladder/rectal contrast: occasionally used in specific circumstances
- MRI fusion: increasingly standard - MRI is co-registered with the planning CT because CT alone has substantial interobserver variability in prostate contouring. MRI-defined prostate volumes are consistently smaller than CT-defined volumes, and MRI better defines the apex and posterior boundary
5. Target Volume Delineation
After scan acquisition, the radiation oncologist contours structures on the planning CT:
Gross Tumor Volume (GTV)
- The macroscopic tumor. For prostate cancer, the prostate gland itself is usually treated as the GTV in localized disease (the tumor is typically not discretely visible on CT).
Clinical Target Volume (CTV)
- Encompasses the prostate ± seminal vesicles ± pelvic lymph nodes based on risk group:
- Low risk: Prostate only
- Intermediate risk: Prostate + proximal 1 cm of seminal vesicles
- High risk: Prostate + full seminal vesicles ± pelvic lymph nodes
- The CTV attempts to account for microscopic extension beyond the visible gland (extraprostatic extension, EPE)
Planning Target Volume (PTV)
- CTV + margin to account for:
- Interfraction organ motion (bladder/rectal filling changes)
- Intrafraction motion (respiratory, peristalsis)
- Setup error
- Typical PTV margin: 0.5-1.0 cm around the CTV
- The posterior margin (toward rectum) is often reduced to 0.5 cm to minimize rectal dose
6. Organs at Risk (OARs) Contouring
The following structures are delineated and dose-constrained:
| OAR | Clinical Relevance |
|---|---|
| Rectum | Risk of proctitis, rectal bleeding |
| Bladder | Risk of cystitis, hematuria |
| Femoral heads | Risk of femoral neck fracture, avascular necrosis |
| Bowel bag / sigmoid | Risk of bowel toxicity, especially with pelvic nodal treatment |
| Penile bulb | Risk of erectile dysfunction |
7. From Simulation to Treatment Planning
After CT simulation, the imaging data are transferred to the treatment-planning system (TPS) where:
- Dosimetrists and physicists design the beam arrangement (angles, fluences, arc parameters)
- For IMRT/VMAT: Inverse planning algorithms optimize beam intensities to meet dose-volume objectives
- For 3D-CRT: Beam's-eye-view design with custom shaping (blocks or MLCs)
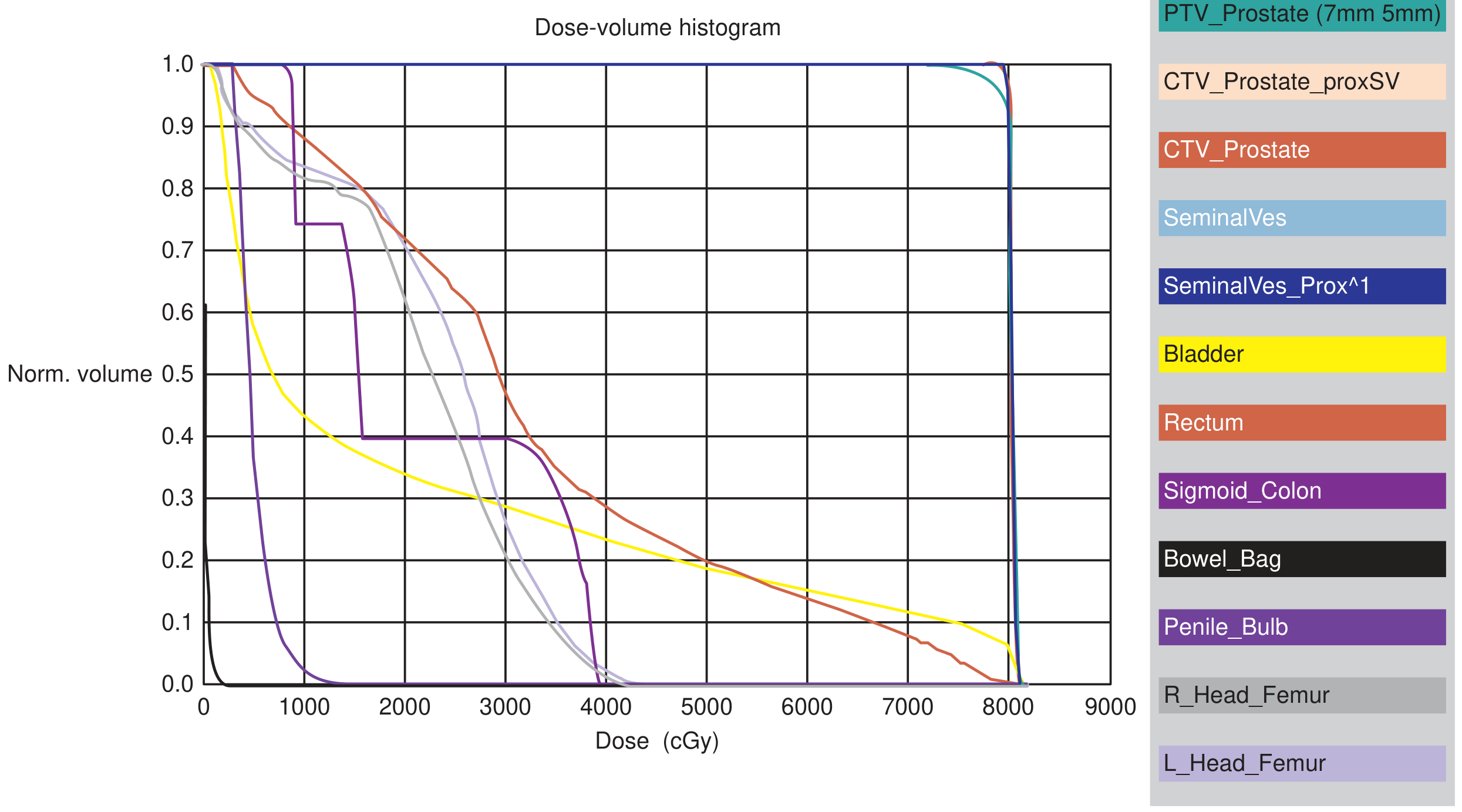
- Results are evaluated using a Dose-Volume Histogram (DVH), which shows the dose received by each contoured structure
The DVH below (from Campbell-Walsh Urology) shows a typical IMRT plan at 78 Gy prescription dose - nearly 100% of the PTV receives prescribed dose, with steep dose fall-off beyond 78-80 Gy, while rectum, bladder, femoral heads, and bowel receive substantially lower doses:
8. Special Scenarios at Simulation
| Finding at CT Sim | Recommended Action |
|---|---|
| Grossly distended rectum | Resimulate after enema; planning on a distended rectum gives worse dosimetry and outcomes |
| Very large prostate (>100 mL) | Continue with current simulation; ADT to downsize is not required; SBRT is less preferred due to higher toxicity risk |
| SBRT/stereotactic plans | CT sim is still required; fiducial markers (gold seeds) are typically placed transrectally or transperineally 1-2 weeks before simulation for daily IGRT |
9. Role of Fiducial Markers and IGRT
For modern IGRT-guided EBRT:
- Gold fiducial markers (3 seeds, typically) are implanted into the prostate transrectally under ultrasound guidance 1-2 weeks before CT simulation
- These seeds are visible on CT and daily kV imaging at the treatment unit
- They allow online prostate localization before each fraction, enabling smaller PTV margins
- Rectal spacer (SpaceOAR hydrogel) - an absorbable hydrogel injected between the prostate and rectum at the same time, creating a ~1-cm space that reduces rectal dose
Summary
CT simulation for prostate cancer is a carefully orchestrated process: bowel prep → bladder filling protocol → reproducible immobilization → CT acquisition at 3-5 mm slices → GTV/CTV/PTV/OAR contouring → MRI fusion (when available) → DVH-guided IMRT/VMAT plan optimization. The quality of the simulation scan directly determines the accuracy of the treatment plan delivered over subsequent weeks.
Sources: Campbell-Walsh Wein Urology, p. 4692-4696 | ACR Appropriateness Criteria - External Beam RT Treatment Planning for Clinically Localized Prostate Cancer | Northwestern Medicine CT Simulation Protocol (2024)
This is a shared conversation. Sign in to Orris to start your own chat.