Lingual thyroid. Ms ent University exam pattern for 10 marks.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive 10-mark answer. Here it is:
Lingual Thyroid - MS ENT University Exam (10 Marks)
Definition
Lingual thyroid is the most common form of ectopic thyroid tissue, resulting from failure of descent of the thyroid anlage from the foramen caecum of the tongue to its normal pretracheal position in the neck. It accounts for approximately 90% of all ectopic thyroid tissue.
Embryology (Developmental Basis)
The thyroid gland originates as a median endodermal outgrowth from the floor of the pharynx at the foramen caecum (junction of anterior 2/3 and posterior 1/3 of tongue) at around the 4th week of embryonic life. It then descends along the thyroglossal tract to reach its final pretracheal position by the 7th week. Failure of this descent at any point results in ectopic thyroid tissue - the most common arrest point being the tongue base, producing a lingual thyroid.
Epidemiology
- Prevalence: 1 in 100,000 (rare)
- Girls are more commonly affected than boys
- In 70-80% of cases, the lingual thyroid is the only functioning thyroid tissue present in the body - this has critical surgical implications
- Up to one-third of patients demonstrate hypothyroidism
- Hyperthyroidism is rare
- Malignant transformation carries the same risk as eutopic thyroid tissue (rare but reported)
Clinical Features / Presentation
Symptoms relate to mass effect and endocrine dysfunction:
| Symptom | Mechanism |
|---|---|
| Dysphagia | Mass at tongue base obstructs swallowing |
| Airway obstruction | Large mass in oropharynx |
| Foreign body sensation / globus | Pharyngeal mass effect |
| Dysphonia | Involvement of pharyngeal structures |
| Haemorrhage | Erosion of overlying mucosa |
| Hypothyroidism | Insufficient thyroid tissue |
- Many patients are completely asymptomatic - detected incidentally on ENT examination or parental observation
- Symptoms may worsen during periods of increased metabolic demand - puberty, pregnancy, or physiological stress (due to TSH-driven enlargement)
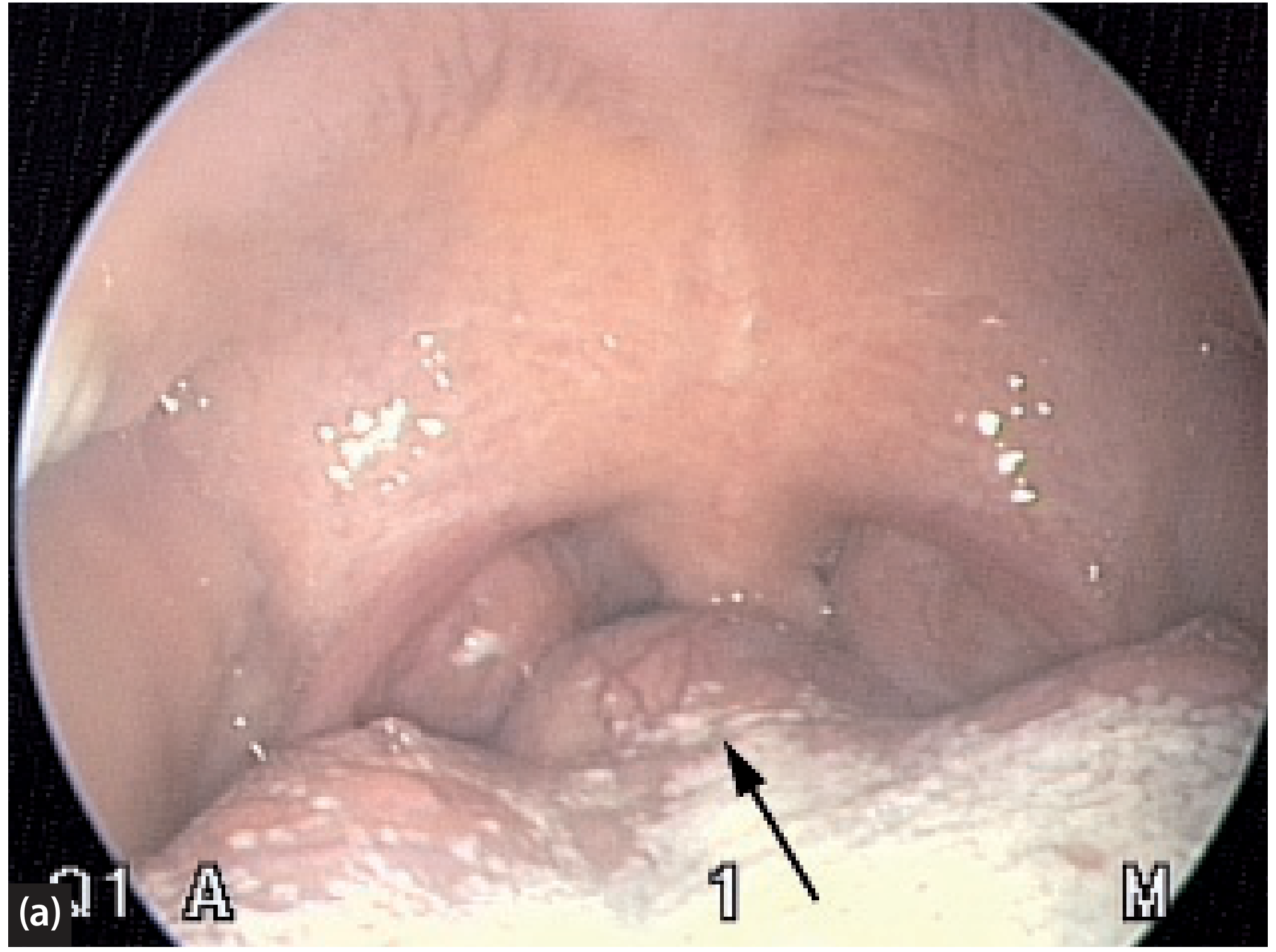
- Appears as a smooth, midline, reddish-pink mass at the base of tongue, just anterior to the foramen caecum
Investigations
1. Imaging
- CT scan (unenhanced) - outlines lingual thyroid well because it is hyperdense compared to surrounding tongue muscle; sagittal views particularly helpful
- MRI - preferred over CT to avoid ionizing radiation, especially in children; sagittal views best
- Purpose: confirm diagnosis AND identify whether any thyroid tissue exists in the normal cervical position
2. Nuclear Medicine
- Technetium-99m (99mTc) thyroid scan - shows metabolic activity at tongue base with no uptake in the neck (confirms absence of ectopic and eutopic tissue)
- Essential before any surgery to confirm the lingual thyroid is the only functioning tissue
3. Thyroid Function Tests (TFTs)
- Usually normal
- Up to 1/3 show hypothyroidism (elevated TSH, low T3/T4)
- Hyperthyroidism rare
4. FNAC
- If malignancy is suspected (though rare)
Treatment
A. Conservative / Medical
Indications: Small, asymptomatic lingual thyroid
- TSH suppression with exogenous thyroid hormone (thyroxine) - reduces TSH drive and may cause gradual reduction in size; reduction is often slow and dramatic results should not be expected
- Paediatric endocrinology input is mandatory
- Radioactive iodine (RAI) - generally avoided in children; may be considered in adults where surgery is not feasible
B. Surgical Excision
Indications:
- Significant obstructive symptoms (dysphagia, airway compromise)
- Repeated or severe haemorrhage
- Symptomatic euthyroid patients
- Suspected malignancy
Approaches:
| Approach | Details |
|---|---|
| Transoral | Preferred for most; nasotracheal intubation used; CO2 laser or cautery |
| Transoral robotic | Emerging technique for larger lesions |
| Transcervical | Lateral pharyngotomy or transhyoid pharyngotomy for larger/deeper lesions |
| Tracheostomy | May be required for very large masses where post-excision swelling and airway obstruction are anticipated |
Key Surgical Principle:
Since 70-80% of these patients have the lingual thyroid as their only functioning thyroid tissue, the clinician must be prepared to administer lifelong exogenous thyroid hormone replacement therapy postoperatively. Removing the lingual thyroid renders the patient permanently hypothyroid.
Important Points for Exam
- Lingual thyroid = most common ectopic thyroid (90% of all ectopic thyroid)
- Located at foramen caecum (junction of anterior 2/3 and posterior 1/3 of tongue)
- In 70-80% of cases, it is the ONLY thyroid tissue
- Always do 99mTc scan before surgery to assess for normal cervical thyroid
- Never biopsy/excise without confirming functional status - risk of rendering patient hypothyroid
- Malignancy risk same as eutopic thyroid
- Lifelong thyroid function monitoring is essential
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2, Chapter 41; Cummings Otolaryngology Head and Neck Surgery, Chapter 90
This is a shared conversation. Sign in to Orris to start your own chat.