Classify Burns and explain the pt management and rehabilitation of 30 year old man with Burns on the anterior aspect of neck and chest in detail for 10 marker with explanation of everything thing in detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Searching the Web
burn rehabilitation neck chest contracture physiotherapy pressure garment splinting 2024
I now have all the information needed for a comprehensive 10-marker answer. Let me compose it:
Burns: Classification, Patient Management, and Rehabilitation
Case: 30-year-old male with burns on the anterior neck and chest
PART 1: CLASSIFICATION OF BURNS
Burns are classified along four major axes: depth, size (TBSA), cause, and severity.
A. Classification by Depth
Based on the original classification by Dupuytren (1832), burns are classified into the following degrees (Schwartz's Principles of Surgery, 11th Ed.):
| Degree | Layers Involved | Clinical Features | Healing |
|---|---|---|---|
| Superficial (1st degree) | Epidermis only | Painful, erythematous, dry, no blisters, blanches on pressure | Within 1 week, no scarring |
| Superficial Partial-Thickness (2nd degree - superficial) | Epidermis + papillary dermis | Very painful, wet, blisters, erythematous, blanches | 1-3 weeks, minimal scarring |
| Deep Partial-Thickness (2nd degree - deep) | Epidermis + reticular dermis | Painful to pressure only, mottled/white/erythematous, may be wet or dry, can blister | 2-9 weeks, often requires grafting, hypertrophic scarring |
| Full-Thickness (3rd degree) | Entire dermis + subcutaneous fat | Leathery, waxy/white/gray/black, insensate, no blisters, inelastic eschar | Weeks-months, requires surgical grafting |
| Deep Full-Thickness (4th degree) | Muscle, tendon, ligament, bone | Charred, completely insensate, may require amputation | Surgical reconstruction needed |
ROSEN's Emergency Medicine (9th Ed.): "Full-thickness burns involve the entire dermis and often some underlying adipose tissue and result in an inelastic burn eschar that is waxy and white, gray, or black without blisters."
Jackson's Three Zones of Burn Injury (Schwartz's Principles of Surgery):
- Zone of Coagulation (center): Maximum damage, coagulated necrotic tissue - requires excision and grafting
- Zone of Stasis (middle): Variable ischemia - can convert deeper with infection or poor perfusion; can be saved with good resuscitation
- Zone of Hyperemia (periphery): Minimal damage, heals spontaneously - similar to superficial partial-thickness
B. Classification by Size - The Rule of Nines
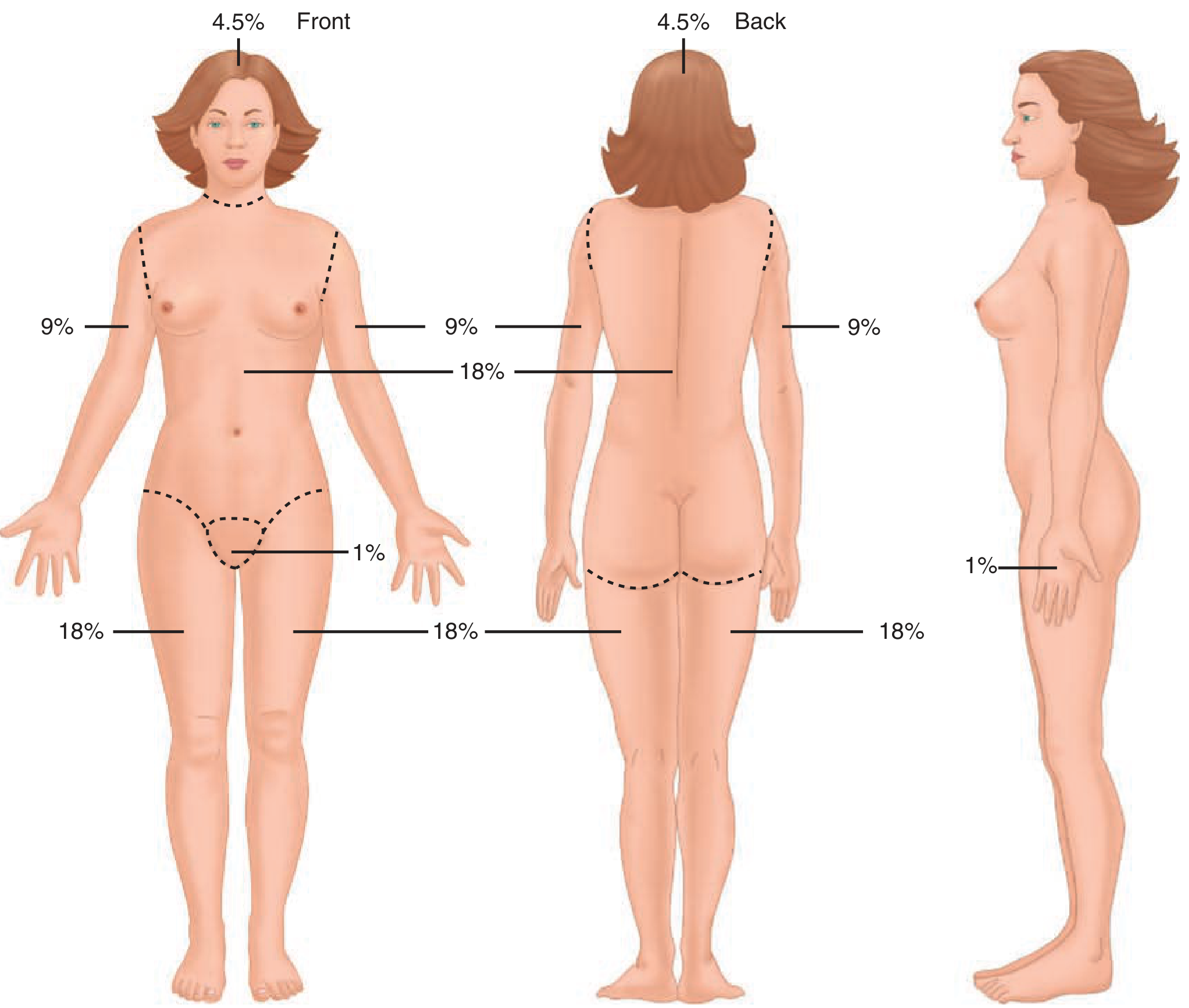
In our patient (anterior neck + anterior chest):
- Anterior neck = approximately 1% TBSA
- Anterior chest = 9% TBSA (anterior trunk is 18%, chest alone is ~9%)
- Total estimated TBSA = ~10%
This is a moderate burn by size, but the location (neck and chest) is critical:
- Anterior neck burns risk airway compromise from edema/eschar
- Chest burns may restrict respiratory excursion
- These are classified as special area burns requiring special consideration
C. Classification by Cause
| Type | Mechanism |
|---|---|
| Thermal | Flame, scald (hot water/steam), contact with hot object |
| Chemical | Acid or alkali exposure causing progressive tissue destruction |
| Electrical | Entry/exit wounds, deep tissue destruction despite small surface wound |
| Radiation | Sunburn, radiotherapy |
| Friction | Abrasion-type burns |
D. Classification by Severity (ABA Criteria)
| Category | Criteria |
|---|---|
| Minor | <10% TBSA partial-thickness in adults; no face/hands/feet/genitalia/major joints/circumferential involvement |
| Moderate | 10-20% TBSA partial-thickness; or <10% full-thickness |
| Major/Severe | >20% TBSA partial-thickness; or >5% full-thickness; any burn of face, hands, feet, genitalia; inhalation injury; circumferential burn |
Our 30-year-old patient (anterior neck + anterior chest, ~10% TBSA): classified as moderate by size, but the neck location upgrades it to major due to risk of airway compromise and potential for functionally debilitating contractures.
PART 2: PATIENT MANAGEMENT
Step 1 - Primary Survey (ABCDE)
A - Airway (Most Critical in Neck Burns):
Burns of the anterior neck demand immediate airway assessment. Signs of inhalation injury or impending obstruction include:
- Singed nasal hairs, eyebrows, facial burns
- Hoarseness, stridor, carbonaceous sputum
- Burns in an enclosed space
Early endotracheal intubation is recommended if any airway compromise is suspected - edema will worsen progressively over the next 24-48 hours. Once significant edema develops, intubation becomes extremely difficult.
B - Breathing:
Chest burns (especially circumferential) can restrict chest wall excursion, resulting in restrictive respiratory failure. If chest movement is compromised, escharotomy (incision through the burn eschar) is required to release the chest wall.
C - Circulation:
- Establish two large-bore IV lines (through or around burned tissue if necessary)
- Early fluid resuscitation
- Monitor urine output (Foley catheter)
D - Disability: Neurological status (GCS)
E - Exposure/Environment: Full exposure to assess all burns, prevent hypothermia
Step 2 - Fluid Resuscitation
Burn injury drives a massive inflammatory response causing capillary leak with plasma extravasation into the extravascular space (Sabiston Textbook of Surgery). This fluid loss peaks in the first 24 hours.
Parkland (Baxter) Formula - the most widely used:
4 mL × body weight (kg) × % TBSA burned = total Lactated Ringer's in first 24 hours
For our 30-year-old patient (assuming 70 kg, 10% TBSA):
4 × 70 × 10 = 2,800 mL of Lactated Ringer's over 24 hours
- Half (1,400 mL) in the first 8 hours from time of burn
- Remaining half (1,400 mL) over the next 16 hours
The American Burn Association consensus recommends starting with 2 mL/kg/% TBSA to avoid over-resuscitation ("fluid creep"). The formula is only a starting point - fluids must be titrated to:
- Urine output: 30 mL/hour in adults (0.5 mL/kg/h)
- Mean arterial pressure: >60 mmHg
Colloids are generally not given in the first 24 hours (capillary permeability is too high and they will leak into interstitium). After 24 hours, albumin may be given to restore oncotic pressure.
Step 3 - Wound Assessment and Initial Care
Estimating Burn Depth: Even experienced burn surgeons find accurate depth assessment challenging within the first 48-72 hours, as burn wounds evolve during this period (Schwartz's Principles of Surgery). Adjuncts include laser Doppler imaging, biopsy, and thermal imaging.
Initial Wound Care:
- Gentle cleaning - remove debris, loose dead tissue, open blisters
- Topical antimicrobials - the cornerstone of preventing wound infection:
- Silver sulfadiazine 1% - broad spectrum, most widely used
- Mafenide acetate - penetrates eschar, useful for deep burns
- Silver-containing dressings (e.g., Mepilex Ag, Aquacel Ag) - modern alternatives with less frequent changes
- Dressing goals (Sabiston Textbook of Surgery):
- Protect damaged epithelium
- Minimize bacterial/fungal colonization
- Maintain moist wound environment
- Reduce evaporative heat and cold stress
- Provide comfort
- Splint in position of function
For the anterior neck: The neck must be positioned in extension to prevent contracture formation - use a neck conformer or cervical collar.
Step 4 - Surgical Management
Escharotomy: For full-thickness circumferential or near-circumferential burns of the chest or neck, escharotomy is performed to:
- Release the chest wall for adequate ventilation
- Prevent compression of the airway/vascular structures in the neck
Early Excision and Grafting:
The current standard of care for deep partial-thickness and full-thickness burns is early (within 72 hours) tangential or fascial excision followed by skin grafting (Sabiston Textbook of Surgery):
- Superficial partial-thickness burns - heal conservatively with dressings in 1-3 weeks
- Deep partial-thickness burns - benefit from excision and split-thickness skin graft (STSG); early grafting reduces hospital stay, infection, and scarring
- Full-thickness burns - require excision and grafting (STSG or full-thickness skin graft)
For the neck and chest:
- Contour and mobility requirements make the neck technically challenging to graft
- Sheet grafts (not meshed) are preferred for the face and neck to optimize cosmesis and reduce scarring
- Z-plasty or flap reconstruction may be needed for contractures if they develop later
Step 5 - Analgesia and Sedation
Burns are intensely painful. A multimodal analgesic approach:
- Opioids (morphine, fentanyl) - for background and procedural pain
- Paracetamol + NSAIDs - adjuncts
- Ketamine - excellent for dressing changes (provides analgesia + dissociative sedation)
- Gabapentin/pregabalin - for neuropathic pain
- Patient-controlled analgesia (PCA) where applicable
Step 6 - Nutritional Support
Burns cause a hypermetabolic state with massive catabolism (Sabiston Textbook of Surgery). Early enteral nutrition is started within hours of admission:
- Preserves gut mucosal integrity, reduces bacterial translocation, and supports healing
- Caloric requirements calculated using Curreri formula (adults): (25 kcal × weight) + (40 kcal × % TBSA burned)
- High-protein diet: 1.5-2 g/kg/day
- Nasogastric feeding if oral intake is insufficient
Step 7 - Infection Prevention and Monitoring
- Topical antimicrobials (as above) - systemic prophylactic antibiotics are NOT routinely recommended
- Regular wound surveillance for signs of infection (increased exudate, erythema, fever, leucocytosis)
- Wound swabs and blood cultures if infection suspected
- Tetanus prophylaxis
- Scheduled replacement of IV lines to minimize catheter-related sepsis
PART 3: REHABILITATION
Rehabilitation begins on Day 1 and continues for months to years. For anterior neck and chest burns, the primary rehabilitation concerns are:
- Neck flexion contracture (chin-to-chest deformity)
- Chest wall restriction limiting respiratory function
- Hypertrophic scarring
- Psychological impact
Phase 1: Acute Phase (Day 1 to wound closure)
Positioning:
- The neck must be positioned in neutral to slight extension - NOT in flexion (which is the position of comfort but leads to contracture)
- Use a foam cervical collar or conformer to maintain neck extension when at rest
- Head of bed elevated 30-45° to reduce edema
- Shoulders in slight retraction to prevent pectoral contracture from chest burns
Passive and Active Range of Motion (ROM) Exercises:
- Begin passive ROM from Day 1 - even through bandages
- Cervical ROM: flexion, extension, lateral flexion, rotation
- Shoulder ROM: flexion, abduction, external rotation (anterior chest burns pull the shoulder into adduction and internal rotation)
- Trunk extension exercises to counter chest tightening
- Progress to active-assisted ROM and then active ROM as tolerated
- Exercise should be performed before dressing changes when analgesia is at its peak
Respiratory Physiotherapy:
- Anterior chest burns are a unique challenge - the scar can restrict chest expansion and cause restrictive lung defect
- Deep breathing exercises, incentive spirometry
- Active cycle of breathing technique (ACBT)
- Humidified oxygen and nebulized bronchodilators if inhalation injury present
- Early mobilization - even ventilated patients can be sat out of bed with sufficient analgesia (Sabiston Textbook of Surgery)
Phase 2: Post-Grafting / Sub-Acute Phase (Wound closure to 3-6 months)
Pressure Garment Therapy (PGT):
- The mainstay of hypertrophic scar prevention and treatment
- Custom-fitted compression garments providing 24-25 mmHg pressure are worn 23 hours/day for 12-24 months
- For the neck: a cervical compression collar and/or a face/neck mask (transparent facial orthosis)
- For the chest: a compression vest
- Mechanism: reduces blood flow to the scar, flattens and softens the scar tissue, and reduces pruritus
- Garments must be replaced every 2-3 months as they lose elasticity and as the patient changes shape
Silicone Gel Therapy:
- Silicone gel sheets or gel applied under pressure garments
- Softens and flattens hypertrophic scars
- Used 12-24 hours/day in combination with compression garments
- Mechanism: hydration of the stratum corneum, reducing collagen synthesis in the scar
Splinting:
- Neck conformer/extension splint to prevent chin-to-chest contracture
- Worn at night (or 24 hours a day in resistant contractures)
- The three-poster brace or custom thermoplastic conformer holds the neck in extension, lateral flexion, and rotation
- Chest brace or trunk extension splint to prevent pectoral tightening
Scar Massage:
- Once wounds are fully closed, scar massage begins
- Firm circular massage using a neutral cream for 10-15 minutes per session, 2-3 times daily
- Softens the scar, reduces adhesions, and improves tissue mobility
Stretching and Exercise:
- Progressive stretching of neck flexors and pectorals
- Shoulder strengthening and thoracic mobility exercises
- Resistance training as tolerated
Phase 3: Long-Term Rehabilitation (6 months onward)
Scar Maturation:
Hypertrophic scars typically mature over 1-2 years, becoming paler, flatter, and softer. Management continues until the scar is mature.
Surgical Intervention for Contractures:
If conservative rehabilitation fails, surgical release is required:
- Z-plasty - gold standard for linear contractures; the interdigitating flaps by design lengthen the contracted site
- Y-V plasty - for shorter contractures
- Full-thickness skin grafts - replace more dermis, reducing recurrence of contracture compared to split-thickness grafts
- Pedicled or free flaps - for complex or recurrent contractures
Post-surgical rehabilitation restarts immediately.
Psychological Rehabilitation:
- Burns of the neck and chest are visible and affect body image and social functioning
- Cognitive behavioral therapy (CBT) for adjustment disorder, depression, PTSD
- Peer support groups (burn survivor networks)
- Social reintegration programs - vocational rehabilitation, return-to-work planning
- Monitoring for post-traumatic stress disorder (PTSD)
Itch (Pruritus) Management:
- Hypertrophic scars are intensely itchy and this significantly impairs quality of life
- Antihistamines (cetirizine, hydroxyzine)
- Gabapentin - most effective agent for burn itch
- Topical menthol or counterirritants
- Massage and compression also reduce itch
Summary Table: Management at a Glance
| Phase | Key Priorities |
|---|---|
| Immediate (0-24h) | Airway (early intubation if needed), Fluid resuscitation (Parkland formula: 2,800 mL LR in 24h), wound cleaning |
| Acute (Day 1 to closure) | Topical antimicrobials, positioning in extension, ROM exercises, respiratory physio, analgesia, nutrition |
| Sub-acute (Post-closure to 6 months) | Pressure garments (23h/day), silicone therapy, splinting, scar massage, progressive exercise |
| Long-term (6m-2 years) | Scar maturation monitoring, surgical release if contracture develops, psychological support |
Key References:
- Schwartz's Principles of Surgery, 11th Ed. - Burn Depth and Resuscitation chapters
- Sabiston Textbook of Surgery, current ed. - Wound Care and Organ Failure in Burns
- ROSEN's Emergency Medicine - Classification and Diagnosis of Burns
- ACI Burn Physiotherapy & Occupational Therapy Clinical Practice Guide (Jan 2025)
- Prevention and Treatment of Burn Scar Contractures, PMC 2024
Classify Burns and explain the physiotherapy management and rehabilitation of 30 year old man with Burns on the anterior aspect of neck and chest in detail for 10 marker with explanation of everything thing in detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
physiotherapy management burns anterior neck chest rehabilitation positioning splinting pressure garment 2024
Reading File
Reading File
Reading Web Page
https://aci.health.nsw.gov.au/__data/assets/pdf_file/0018/23…
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive, exam-ready 10-marker answer with full physiotherapy focus. Let me compose it:
Burns: Classification & Physiotherapy Management/Rehabilitation
Case: 30-year-old male with burns on the anterior neck and anterior chest
PART 1: CLASSIFICATION OF BURNS
Burns are classified based on four main parameters: depth, extent (TBSA), etiology/cause, and severity.
A. Classification by Depth (Degrees)
Based on Dupuytren's original classification (1832), burns are graded by the skin layers destroyed. The modern surgical classification focuses on the need for surgical intervention and healing potential (Tintinalli's Emergency Medicine; ROSEN's Emergency Medicine).
| Degree | Layers Involved | Clinical Features | Healing Time | Scar Risk |
|---|---|---|---|---|
| Superficial (1st) | Epidermis only | Painful, erythematous, dry, no blisters, blanches on pressure | ~7 days | None |
| Superficial Partial-Thickness (2nd - superficial) | Epidermis + papillary dermis | Very painful, wet, blisters, erythematous, blanches | 14-21 days | Minimal |
| Deep Partial-Thickness (2nd - deep) | Epidermis + reticular dermis (including hair follicles, sweat glands) | Painful to pressure only, mottled/white/erythematous, wet or dry, may blister | 3-8 weeks | Permanent hypertrophic scar |
| Full-Thickness (3rd) | Entire dermis + subcutaneous fat | Leathery, insensate, waxy/white/gray/black, no blisters, inelastic eschar | Weeks-months | Severe scarring, requires grafting |
| Deep Full-Thickness (4th) | Muscle, tendon, bone | Charred, completely insensate | Requires reconstruction/amputation | Severe |
ROSEN's Emergency Medicine: "Full-thickness burns involve the entire dermis and often some underlying adipose tissue and result in an inelastic burn eschar that is waxy and white, gray, or black without blisters. Full-thickness burns are insensate."
Jackson's Three Zones of Burn Injury (Schwartz's Principles of Surgery, 11th Ed.):
- Zone of Coagulation (center): Coagulated necrotic tissue - maximum damage, requires excision and grafting
- Zone of Stasis (middle): Variable ischemia - can deepen with infection or poor resuscitation; can be saved with good care
- Zone of Hyperemia (outer): Minimal injury, heals spontaneously
B. Classification by Extent - The Rule of Nines
The body is divided into regions each representing 9% (or multiples of 9%) of Total Body Surface Area (TBSA):
- Head and neck: 9%
- Each upper limb: 9%
- Anterior trunk: 18%
- Posterior trunk: 18%
- Each lower limb: 18%
- Genitalia: 1%
For our patient:
- Anterior neck = ~1% TBSA
- Anterior chest = ~9% TBSA (half of the anterior trunk)
- Total TBSA burned = approximately 10%
For irregular burns, the Rule of Palm is also used: the patient's palm (including fingers) = approximately 1% TBSA.
For pediatric patients, the Lund-Browder chart is more accurate as it accounts for proportional changes with age.
C. Classification by Cause/Etiology
| Type | Mechanism | Key Feature |
|---|---|---|
| Thermal | Flame, scald (hot water/steam), contact burns | Most common |
| Chemical | Acid/alkali - continue to cause damage until removed | Progressive injury |
| Electrical | Entry/exit wounds, massive deep tissue destruction | Iceberg injury - surface underestimates depth |
| Radiation | Sunburn, radiotherapy, nuclear | Delayed presentation |
| Friction | High-speed abrasion | Combination with abrasion |
D. Classification by Severity (American Burn Association)
| Category | Criteria |
|---|---|
| Minor | <10% TBSA partial-thickness; no special area involvement |
| Moderate | 10-20% TBSA partial-thickness; or <10% full-thickness |
| Major/Severe | >20% TBSA partial-thickness; or >5% full-thickness; any burn of face/hands/feet/genitalia; circumferential burn; inhalation injury |
Our patient's classification: ~10% TBSA - moderate by size, but upgraded to major due to the anterior neck location (risk of airway compromise and functionally debilitating contracture).
PART 2: PHYSIOTHERAPY MANAGEMENT
Physiotherapy begins on Day 1 and is a continuous, evolving process across three phases of recovery. The key physiotherapy goals in this patient are:
- Maintain airway patency and respiratory function
- Prevent neck flexion contracture and shoulder/chest tightening
- Preserve and restore full range of motion (ROM)
- Manage oedema
- Manage hypertrophic scarring
- Restore functional independence and quality of life
PHASE 1: ACUTE PHASE (Day 1 to Wound Closure)
1. Respiratory Physiotherapy
Burns of the anterior chest place the patient at high risk for restrictive respiratory impairment - the forming eschar and later scar tissue physically limit chest wall expansion. Anterior neck burns further risk airway compromise from oedema and eschar.
Physiotherapy interventions:
- Airway clearance techniques: Active cycle of breathing technique (ACBT), forced expiratory technique (FET/huffing), postural drainage
- Incentive spirometry: Encourages maximum inspiratory effort, recruits alveoli, prevents atelectasis
- Deep breathing exercises: Diaphragmatic and lateral costal breathing performed hourly when awake
- Positioning: Head of bed elevated 30-45° to reduce airway oedema and facilitate breathing
- Early mobilisation: Even patients on ventilatory support should be sat out of bed with adequate analgesia - this reduces respiratory complications (Sabiston Textbook of Surgery)
- If inhalation injury is present: Nebulized bronchodilators (salbutamol), nebulized heparin, and nebulized acetylcysteine are used alongside physiotherapy
2. Positioning and Oedema Management
Patients instinctively adopt a position of comfort, which is invariably the position of maximum contracture - neck flexion, shoulder protraction, chest collapse. The physiotherapist must counteract this from the first day.
Anti-contracture positioning for this patient (PM&R KnowledgeNow; ACI Burn Therapy Guide 2025):
| Body Region | Correct Anti-Contracture Position | Rationale |
|---|---|---|
| Neck | Neutral to 15° of extension, no rotation or lateral flexion | Prevents chin-to-chest (mentosternal) contracture |
| Shoulders | 90° of abduction with external rotation | Counters anterior chest burn pulling shoulders into adduction/protraction |
| Trunk | Thoracic extension, shoulders retracted | Prevents pectoral tightening from anterior chest burns |
| Head of bed | 30-45° elevation | Reduces oedema of neck and face |
JSM Burns and Trauma: "A neutral to slightly extended neck position achieved by removing pillows under the head during the whole wound healing process prevents the deformity of the chin and neck to either side or mandible-chest adhesion due to wound contracture and hypertrophic scarring."
Oedema management principles (ACI Burn Physiotherapy Guide, January 2025):
- Elevation of the affected area
- Compression bandaging (elastic bandages/Tubigrip) - can begin immediately
- Active exercise to stimulate lymphatic drainage
- Avoidance of dependent positioning
3. Splinting
Splinting is used when the patient cannot actively maintain anti-contracture positioning due to pain, sedation, or poor compliance.
For this patient:
- Neck extension conformer/splint: A custom thermoplastic or foam cervical conformer holds the neck in neutral to slight extension. This prevents the chin from dropping to the chest - the classic neck burn contracture deformity.
- Worn at all times (during dressing changes and exercises, it may be removed briefly)
- For deep burns: worn 23-24 hours/day; for cooperative patients with full active ROM: may be worn only at night
- Trunk extension splint: For significant anterior chest burns, a thoracic extension splint or positioning aid keeps the thorax in extension and the shoulders retracted
Indications for splinting by depth (WRHA Burn Care Guidelines 2025):
- Superficial partial-thickness + full AROM: No splint needed
- Deep partial-thickness + decreased ROM: Night splint
- Deep partial-thickness + uncooperative: Splint all times (except during exercise)
- Full-thickness: Splint all times (except during exercise)
4. Range of Motion (ROM) Exercises
ROM exercises are begun on Day 1 and are the most important active intervention to prevent contractures (PM&R KnowledgeNow).
Progression:
- Passive ROM (PROM) - therapist moves the joint through full range; used initially or when patient is sedated
- Active-Assisted ROM (AAROM) - therapist assists the patient's own movement
- Active ROM (AROM) - patient moves independently
- Resisted/Strengthening exercises - added in later phases
Specific exercises for anterior neck and chest burns:
Cervical ROM:
- Neck extension and retraction (priority - counteracts the contracture direction)
- Cervical lateral flexion (ear to shoulder, each side)
- Cervical rotation (chin to each shoulder)
- Cervical flexion (performed cautiously - only to assess range, not to stretch)
Thoracic/Shoulder ROM:
- Shoulder flexion and overhead elevation
- Shoulder horizontal abduction and external rotation
- Thoracic extension (arms clasped behind head or "open book" stretch)
- Pectoral stretching (doorway stretch)
- Trunk lateral flexion and rotation
Key principle: Exercises should be performed before dressing changes (when analgesic effect is greatest), and at least 2-3 times daily (Brigham and Women's Hospital Inpatient Burn PT Guide).
PHASE 2: POST-GRAFTING / SUB-ACUTE PHASE (Wound Closure to 6 Months)
Once wounds are closed (spontaneously or after skin grafting), the focus shifts to scar management and restoration of full function. This is a critical window - hypertrophic scars are most active and responsive to intervention in the first 1-2 years.
1. Pressure Garment Therapy (PGT)
The single most important scar management intervention. Custom-fitted garments apply sustained pressure of 24-25 mmHg to the scar.
For this patient:
- Cervical compression collar (also called a neck conformer) - fitted custom to the patient's neck contour
- Chest compression vest - covers the anterior chest
Protocol:
- Worn 23 hours/day (removed only for skin care, exercise, and bathing)
- Continued for 12-18 months (until scar maturation)
- Replaced every 2-3 months as elasticity fades and body shape changes
Mechanism: Reduces blood flow to the scar, compresses capillary loops, reduces collagen synthesis, and physically flattens the scar.
Start time: Approximately 3 weeks post-grafting, or when open areas are smaller than a nickel (Brigham and Women's Hospital Burn PT Guide).
2. Silicone Gel Therapy
Applied under or in addition to compression garments:
- Silicone gel sheets or topical silicone gel
- Applied to fully closed skin for 12-24 hours/day
- Softens and flattens hypertrophic scars by hydrating the stratum corneum, reducing collagen synthesis
3. Scar Massage
Once wounds are fully epithelialized and the skin is no longer fragile:
- Firm circular/transverse friction massage using a neutral moisturizing cream
- Duration: 10-15 minutes per area, 2-3 times daily
- Achieves: desensitization of the scar, prevention of adhesions, improved tissue mobility, reduction of pruritus (itch)
- The patient and family/carer are trained in self-massage for home use (PM&R KnowledgeNow)
4. Progressive Stretching and Exercise
- Sustained passive stretching of neck flexors: hold for 30-60 seconds, multiple sets daily
- Pectoral stretching targeting anterior chest tightness
- Progressive strengthening: cervical stabilizers, shoulder external rotators, thoracic extensors
- Aerobic exercise: Introduced progressively - intensive aerobic and resistance training (1 hour, 3×/week) is associated with improved aerobic capacity, muscle strength, physical mobility, and quality of life (PM&R KnowledgeNow)
- Hydrotherapy (pool therapy): Gentle resistance and ROM in warm water - reduces pain during exercise and facilitates movement
5. Continuation of Splinting
Splinting continues alongside exercise during the sub-acute phase:
- The neck conformer/extension splint is worn at night throughout the scar maturation period (12-24 months)
- Upgraded to dynamic splints if contracture is developing despite static splinting
- Serial casting may be used for resistant contractures - a series of progressively correcting casts applied weekly
PHASE 3: LONG-TERM REHABILITATION (6 Months to 2 Years+)
1. Scar Maturation Monitoring
Hypertrophic scars progress through predictable stages (ACI Burn Physiotherapy Guide):
- Acute: Red, raised, active
- 3 months: Thickened and dry
- 7-9 months: Beginning to soften
- 12-24 months: Mature scar (pale, soft, flat)
Intervention continues until the scar is fully mature. Scar assessment tools such as the Vancouver Scar Scale (assessing vascularity, pigmentation, pliability, height) are used to guide ongoing treatment.
2. Surgical Release and Post-Operative Physiotherapy
If conservative rehabilitation fails to prevent contracture, surgical intervention is required:
- Z-plasty: Gold standard for linear contractures - the interdigitating flaps lengthen the contracted area
- Y-V plasty or W-plasty: For shorter contractures
- Full-thickness skin grafts: Replace more dermis, reducing recurrence
- Pedicled/free flaps: For complex recurrent contractures
Post-operatively, physiotherapy restarts immediately - splinting, positioning, ROM exercises, and progressive exercise as above.
3. Itch (Pruritus) Management
Hypertrophic scars are intensely pruritic - this severely affects sleep and quality of life. Physiotherapy contributes through:
- Scar massage - direct mechanical reduction of itch
- Compression garments - reduce scar vascularity and itch
- Transcutaneous electrical nerve stimulation (TENS) - for neuropathic itch
- Cold therapy / cooling sprays - temporary relief
- Pharmacological adjuncts: gabapentin (most effective), antihistamines (cetirizine/hydroxyzine), topical menthol creams
4. Functional and Vocational Rehabilitation
- Activities of Daily Living (ADL) retraining: Dressing, grooming, eating - all affected by neck and shoulder restriction
- Work hardening: Progressive work-specific exercises to prepare for return to employment
- Driving assessment: Neck ROM restriction may impact driving safety
5. Psychological Rehabilitation
Burns of the neck and chest are visible and affect body image profoundly:
- Screening for PTSD, depression, and anxiety is mandatory
- Cognitive Behavioural Therapy (CBT)
- Burn survivor peer support groups
- Body image counselling and social reintegration programs
SUMMARY: Physiotherapy Priorities at Each Phase
| Phase | Key Physiotherapy Interventions |
|---|---|
| Acute (Day 1 to closure) | Respiratory physio (deep breathing, ACBT, spirometry), anti-contracture positioning (neck 15° extension), neck conformer splint, passive + active ROM exercises, oedema management |
| Sub-acute (closure to 6 months) | Pressure garment (23h/day), silicone gel, scar massage, sustained neck stretching, progressive strengthening, aerobic conditioning, dynamic splinting if needed |
| Long-term (6m to 2 years) | Scar maturation monitoring, serial casting/surgical release if contracture develops, vocational rehab, psychological support, itch management |
Key clinical pearl for anterior neck burns: The #1 complication is mentosternal (chin-to-chest) contracture. Preventing this requires unrelenting physiotherapy from Day 1 - positioning in extension, neck conformer splinting, and daily ROM exercises. The patient's natural tendency is to hold the neck in flexion (comfort position), which is the exact position that causes contracture. Every physiotherapy visit must address this.
References:
- Schwartz's Principles of Surgery, 11th Ed. - Burn Depth and Jackson's Zones
- ROSEN's Emergency Medicine - Classification and Diagnosis of Burns
- Tintinalli's Emergency Medicine - Burn Depth Table (Table 217-2)
- Sabiston Textbook of Surgery - Wound Care; Rehabilitation; Early Mobilisation
- ACI Burn Physiotherapy & Occupational Therapy Clinical Practice Guide, January 2025
- PM&R KnowledgeNow - Burn Rehabilitation (AAPMR)
- Brigham and Women's Hospital - Inpatient Physical Therapy Management of Burns
This is a shared conversation. Sign in to Orris to start your own chat.