Eye trauma
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Searching PubMed
"ocular trauma" AND management
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have extensive, well-sourced material covering all major aspects of eye trauma. Let me compose the comprehensive answer.
Eye Trauma
Eye trauma ranges from minor self-limiting injuries to true ophthalmic emergencies that can cause permanent vision loss. Here is a structured overview based on Tintinalli's Emergency Medicine, Goldman-Cecil Medicine, and Textbook of Family Medicine.
Initial Assessment (Any Eye Trauma)
The first priorities are:
- Visual acuity - check before any other intervention; this is the vital sign of the eye
- Anterior chamber depth - if flat, a ruptured globe is certain; stop the exam immediately
- Globe integrity - look for the Seidel sign (aqueous leaking through a corneal/scleral defect, diluting fluorescein dye)
- Ocular motility - restricted upgaze or lateral gaze suggests orbital blow-out fracture with entrapment
- Intraocular pressure - only if no signs of open globe
Key rule: never pressure the globe in a suspected open globe injury. Apply a protective metal shield (or a paper cup bent over the orbit - see below) and refer emergently.
Classification by Mechanism
1. Chemical Burns - TRUE EMERGENCY (Act First, Examine Later)
Chemical burns are the one injury where treatment precedes full examination.
- Acid burns (e.g., battery acid): cause immediate coagulative necrosis; the eschar limits further penetration
- Alkali burns (e.g., lye, ammonia, cement): far more devastating - saponify cell membranes and continue penetrating long after initial contact. Can cause corneal melting, perforation, and chronic glaucoma. An alkaline substance like lye can cause permanent, irreversible blindness.
Immediate management:
- Copious irrigation - up to 1,000 mL normal saline or lactated Ringer's (or water from any available source in the field)
- Continue until conjunctival pH = 7.5-8.0; check pH after irrigation and again 30 minutes later
- Aggressive antibiotic ointment and lubrication post-irrigation
- Immediate ophthalmology consultation
2. Corneal Injuries
Corneal Abrasion
- Caused by contact lenses, fingernails, foreign objects, or high-speed machinery
- Symptoms: intense pain (delayed up to several hours), foreign body sensation, photophobia, tearing, blepharospasm
- Diagnosis: fluorescein staining under cobalt blue light; slit lamp exam shows irregular epithelial defect
- Relief of pain with topical anesthetic is virtually diagnostic
- Management:
- Topical NSAIDs or short course of topical antibiotics (e.g., erythromycin ointment)
- Patching is generally not recommended
- Heals in 24-48 hours typically
- Follow up for abrasions from contact lens wear (risk of Pseudomonas infection)
Corneal Foreign Body
- History of high-speed machinery (grinder, lawn mower, hammering metal on metal) raises concern for full-thickness penetration
- Metal foreign bodies leave a rust ring within hours; remove with a burr at slit lamp
- After removal, treat as corneal abrasion
Corneal Laceration / Open Globe
- Seidel test: positive streaming of aqueous through the wound (fluorescein washes out in a stream)
- Do not remove any impaled objects
- CT orbit (2-3 mm cuts, axial and coronal) - preferred imaging; MRI contraindicated if metallic foreign body possible
- Ophthalmology emergently; NPO, antiemetics, avoid Valsalva
3. Conjunctival Injuries
- Less symptomatic than corneal injuries due to lower innervation
- Subconjunctival hemorrhage: bright red, well-demarcated; usually benign and resolves in 1-2 weeks. However, 360-degree hemorrhage after trauma should raise suspicion for globe rupture
- Conjunctival laceration: check with Seidel test to rule out globe perforation; most do not require suturing
- Management: erythromycin ointment 0.5% QID x 2-3 days; refer if globe laceration suspected
4. Blunt Trauma - Specific Injuries
Hyphema
Hemorrhage into the anterior chamber, usually from blunt trauma tearing the iris root.
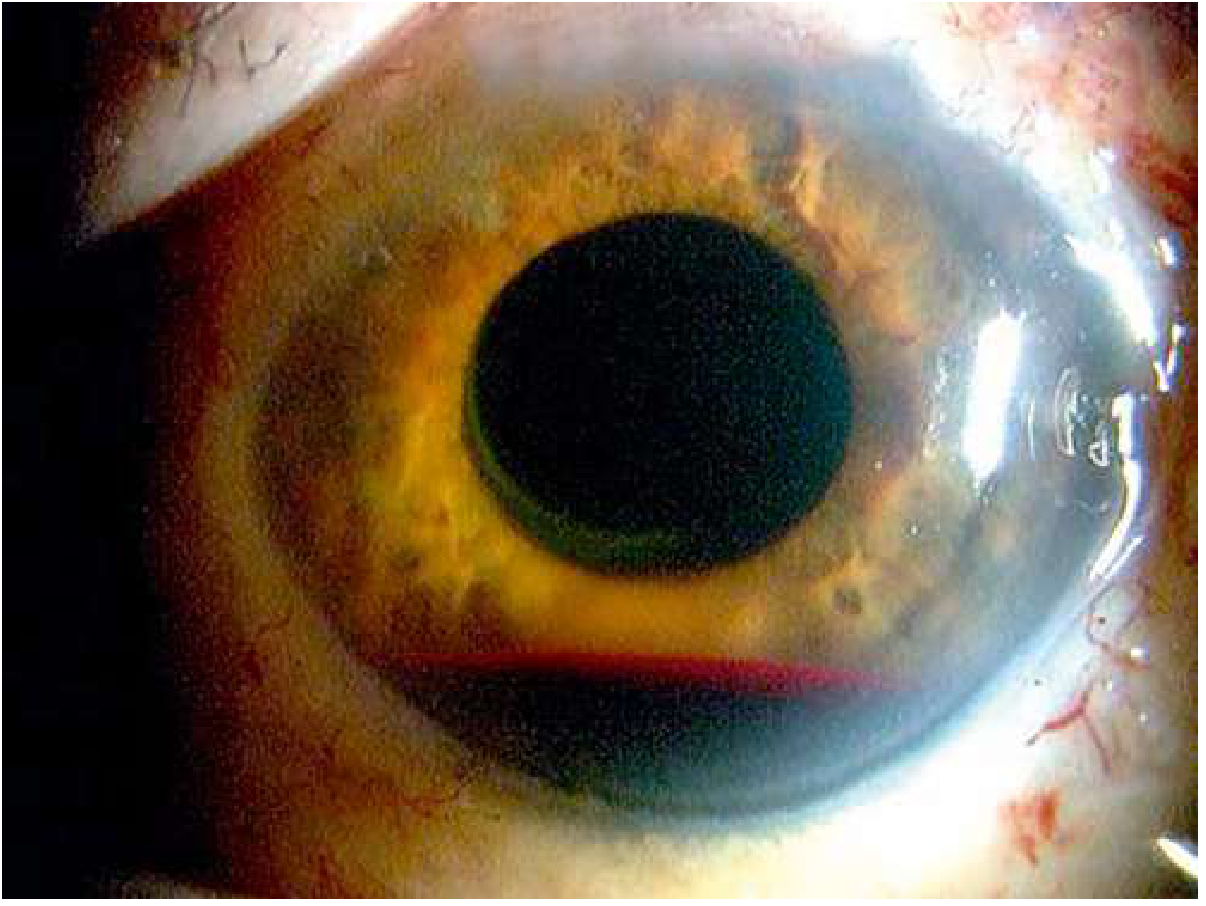
Hyphema: blood has settled by gravity to form a fluid level in the inferior anterior chamber. (Edward S. Harkness Eye Institute, Columbia University)
- Graded by percentage of anterior chamber filled (Grade I < 1/3, Grade II 1/3-1/2, Grade III > 1/2, Grade IV = "8-ball" total)
- If supine, blood distributes uniformly over iris simulating heterochromia
- Complications: secondary glaucoma, corneal blood staining (especially with IOP > 25 mmHg), rebleeding (peak at day 3-5)
- Requires prompt ophthalmology evaluation; management includes head elevation 30-45°, cycloplegics, aminocaproic acid to prevent rebleeding, and monitoring IOP
Globe Rupture
- Most common rupture site: the limbus (junction of cornea and sclera) - a pigmented mass there may be a blood clot or prolapsed uveal tissue (iris)
- Signs: 360° subconjunctival hemorrhage, peaked/irregular pupil pointing toward rupture, flat anterior chamber, decreased IOP (paradoxically may be normal), poor view of fundus due to vitreous hemorrhage
- Any manipulation may extrude intraocular contents - stop the exam, shield, and refer emergently for surgical repair
Traumatic Iritis
- Common after blunt trauma; cells and flare on slit lamp
- Pupil may be constricted or dilated
- Treat with cycloplegics and topical steroids; ophthalmology follow-up
Lens Dislocation (Subluxation)
- Blunt trauma can rupture zonular fibers
- Slit lamp shows asymmetric lens position, iridodonesis (trembling iris)
- Urgent ophthalmology referral
Vitreous Hemorrhage
- Floaters, cobwebs, painless visual loss
- Fundus view obscured; ultrasound is the key imaging tool to rule out retinal detachment
- Urgent ophthalmology
5. Orbital Injuries
Orbital Blow-Out Fracture
- Mechanism: blunt force raises intraorbital pressure, fracturing the weak floor (or medial wall) into the maxillary/ethmoid sinus
- Clinical features:
- Restricted upgaze (inferior rectus entrapment)
- Enophthalmos (sunken globe - may be masked early by edema)
- Infraorbital numbness (inferior orbital nerve)
- Diplopia
- Imaging: CT facial bones
- Avoid nose-blowing (forces air into orbit causing emphysema)
- Ophthalmology + ENT/plastics referral; surgery if significant enophthalmos or persistent diplopia
Orbital Hemorrhage / Retrobulbar Hematoma
- Postseptal hemorrhage can cause orbital compartment syndrome - a true emergency
- Clinical: eye pain, proptosis, impaired EOM, decreased vision, afferent pupillary defect, elevated IOP
- IOP > 40 mmHg - indication for emergency lateral canthotomy and cantholysis
- Lateral canthotomy procedure: local anesthetic at lateral canthus, clamp horizontally for 1 minute, then incise to release lateral canthal tendon
6. Eyelid Injuries
- Lacerations involving the lid margin (> 1 mm) require repair by an oculoplastic specialist
- Full-thickness lid lacerations need layered repair: tarsus with absorbable 6-0 suture (not through conjunctiva - would abrade cornea); lid margin with 6-0 silk using meibomian gland orifices as landmarks; skin with 7-0 nylon
- Medial canthal lacerations: risk damage to lacrimal canaliculi - probe before repair
7. Intraocular Foreign Body (IOFB)
- High suspicion with: hammering metal on metal, grinding, weed whacking
- May present with surprisingly mild symptoms
- CT orbit (NOT MRI if metallic) essential
- Urgent surgical removal; risk of endophthalmitis and siderosis/chalcosis over time
8. Radiation / UV Injury (Photokeratitis)
- Caused by welding arc, sun lamps, UV reflection off snow
- Delayed onset 6-12 hours after exposure
- Bilateral pain, photophobia, foreign body sensation
- Punctate corneal staining on fluorescein
- Treatment: cycloplegics, topical NSAIDs, lubricants; resolves in 24-48 hours
Summary - Urgency Classification
| Condition | Urgency | Key Action |
|---|---|---|
| Chemical burn | Immediate (seconds) | Irrigate first, then assess |
| Open globe / ruptured globe | Immediate | Shield, NPO, emergent OR |
| Retrobulbar hematoma with OCS | Immediate | Lateral canthotomy |
| Central retinal artery occlusion | Minutes (< 90 min) | Massage, paracentesis, ophthalmology |
| Hyphema | Urgent (hours) | Ophthalmology, IOP monitoring |
| Corneal laceration | Urgent | Ophthalmology same day |
| Traumatic iritis | Same day | Cycloplegics, ophthalmology |
| Orbital blow-out fracture | 1-2 weeks | CT, ophthalmology + ENT |
| Corneal abrasion | Same day follow-up | Antibiotics, analgesia |
| Subconjunctival hemorrhage | Routine | Reassurance, monitor |
Sources:
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide - Chapter 241, "Eye Trauma" (pp. 1586-1600)
- Goldman-Cecil Medicine, "Major Ocular Trauma" (p. 4128)
- Textbook of Family Medicine 9e, "Eye Trauma" and "Chemical Burns" (pp. 354-355)
This is a shared conversation. Sign in to Orris to start your own chat.