Tiles classification with images
Asking for Preferences
Tiles classification for Pelvis
Reading File
Finding Sources
Searching the Web
Tile classification pelvic fractures types A B C images diagram
Finding Sources
Reading Web Page
https://radiopaedia.org/articles/tile-classification-of-pelv…
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
I now have all the content and images needed for a complete answer. Here is the full guide:
Tile Classification of Pelvic Fractures
The Tile classification (also aligned with the AO/OTA system) categorizes pelvic ring fractures based on stability - both rotational and vertical. This directly guides treatment decisions and predicts prognosis. It was developed by Marvin Tile in 1984 and later modified by Helfet to align with the AO/OTA fracture system.
Source: Campbell's Operative Orthopaedics 15th Ed 2026; Rockwood & Green's Fractures in Adults 10th Ed 2025
Overview Principle
The key biomechanical question is: Are the posterior pelvic ligaments (sacroiliac + sacrospinous + sacrotuberous) intact?
| Type | Stability | Posterior Ligaments |
|---|---|---|
| A | Stable | Intact |
| B | Rotationally unstable, vertically stable | Partially disrupted |
| C | Rotationally AND vertically unstable | Completely disrupted |
TYPE A - Stable Pelvic Ring Injuries
The posterior ligamentous complex is intact. The pelvic ring is not significantly disrupted. These can be managed non-operatively.
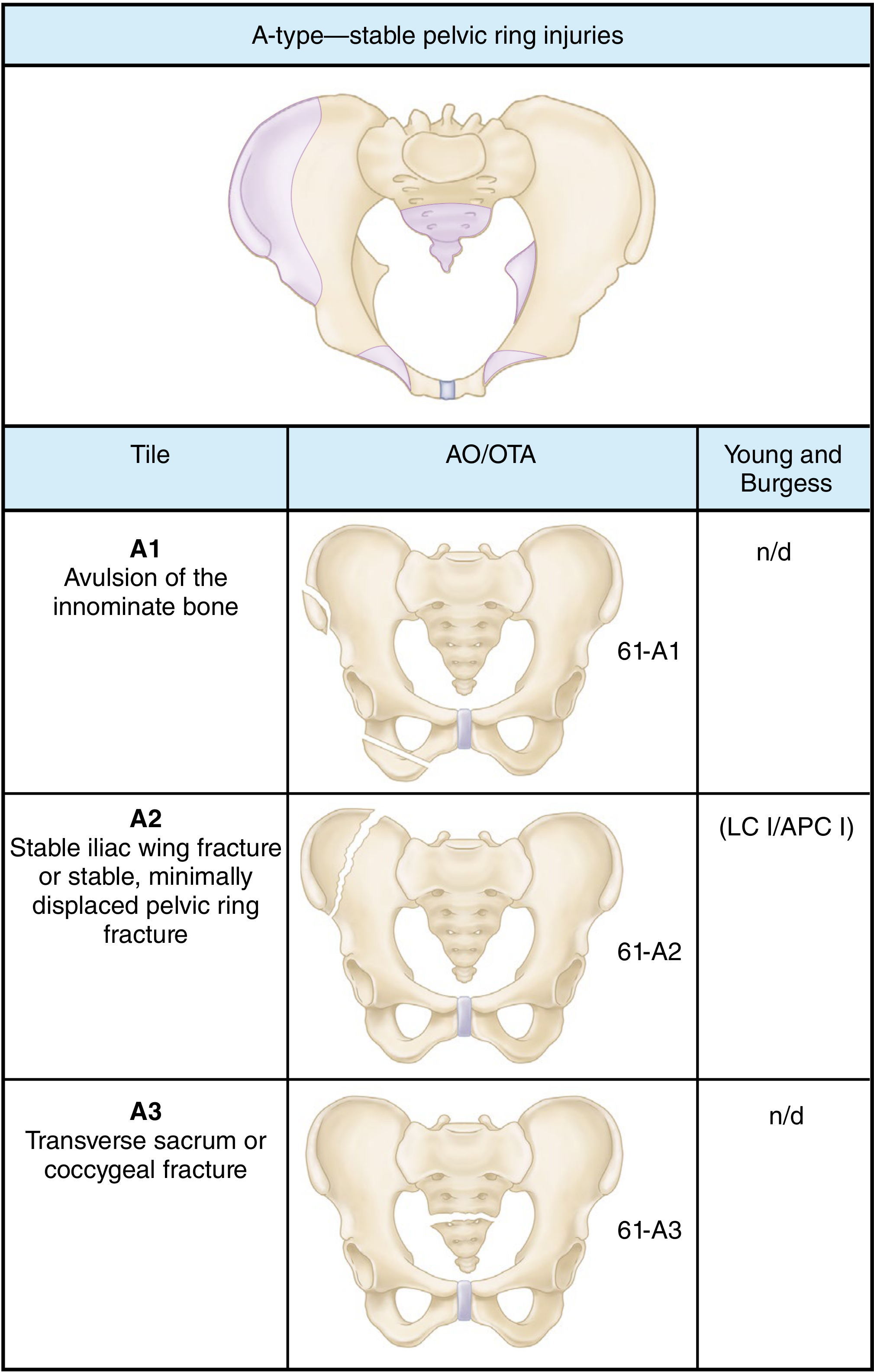
| Subtype | Description | Example |
|---|---|---|
| A1 | Fractures NOT involving the ring | Avulsions of ASIS, AIIS, ischial tuberosity; isolated iliac wing fracture |
| A2 | Stable, minimally displaced ring fractures | Iliac wing fracture (Duverney), isolated anterior ring injury |
| A3 | Transverse sacrococcygeal fractures | Sacral or coccyx fractures - considered spinal injuries, not ring disruptions |
Management: Non-operative (protected weight bearing). Early mobilization is safe.
TYPE B - Rotationally Unstable, Vertically STABLE
The posterior sacroiliac (SI) ligaments and interosseous ligaments are partially intact - they prevent vertical displacement but the pelvis can rotate. Requires surgical fixation.
| Subtype | Description | Mechanism | Notes |
|---|---|---|---|
| B1 | Open-book injury (external rotation) | Anteroposterior compression (APC) | Symphysis diastasis; stages by width: Stage 1 (<2.5 cm, intact sacrospinous), Stage 2 (>2.5 cm, sacrospinous ruptured), Stage 3 (bilateral) |
| B2 | Lateral compression - ipsilateral | LC (internal rotation) | B2.1: ipsilateral sacral fracture; B2.2: posterior SI ligament rupture; B2.3: crescent fracture (ilium) |
| B3 | Bilateral injury | Combined APC + LC | B3.1: bilateral open book; B3.2: "windswept pelvis" (LC-III); B3.3: bilateral LC |
Key radiographic sign: Symphysis widening >2.5 cm = rupture of sacrospinous ligament = rotational instability.
Management: Anterior fixation (external fixator or symphyseal plating) is usually sufficient due to intact posterior column.
TYPE C - Rotationally AND Vertically Unstable
Complete disruption of all posterior ligamentous structures. The hemipelvis is free to displace in all directions - the most severe and life-threatening pattern.
| Subtype | Description | Notes |
|---|---|---|
| C1 | Unilateral | C1-1: iliac fracture; C1-2: SI fracture-dislocation; C1-3: sacral fracture |
| C2 | Bilateral - one side B, one side C | One hemipelvis vertically stable, one unstable |
| C3 | Bilateral - both sides C | Both hemipelves rotationally AND vertically unstable; may have associated acetabular fracture |
Mechanism: Vertical shear (VS) - upward force through one lower extremity (e.g., fall from height).
Management: Requires BOTH anterior AND posterior fixation. Associated with worst outcomes, highest rate of neurologic injury.
Denis Sacral Zone Classification (used alongside Tile for C1-3)
When the posterior injury involves the sacrum (C1-3), the Denis zones define neurologic risk:
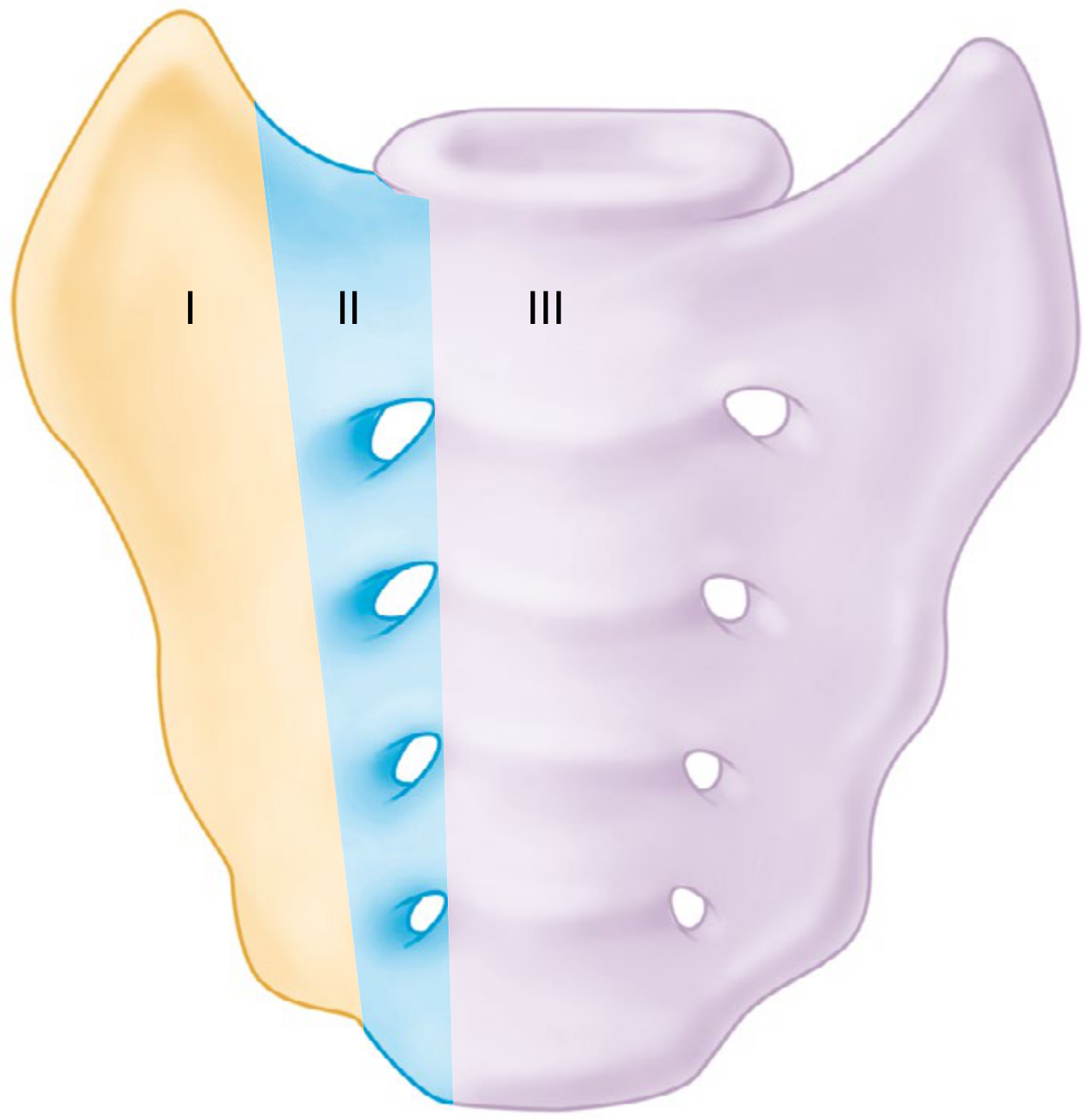
| Zone | Location | Nerve injury rate |
|---|---|---|
| Zone I | Lateral to sacral foramina (sacral ala) | 1.9-5.9% (L5 root) |
| Zone II | Through sacral foramina (transforaminal) | 5.8-28.4% (L5-S2) |
| Zone III | Medial to foramina (central/spinal canal) | 8.6-56.7% (bowel/bladder in 76%) |
Complete Tile/AO-OTA Classification Summary
| Tile | AO/OTA | Description | Stability |
|---|---|---|---|
| A1 | 61-A1 | Avulsion of innominate bone | Stable |
| A2 | 61-A2 | Stable iliac wing or minimally displaced ring fracture | Stable |
| A3 | 61-A3 | Transverse sacrum/coccyx | Stable |
| B1 | 61-B1 | Open book (external rotation) | Rotationally unstable |
| B2 | 61-B2 | LC ipsilateral (internal rotation) | Rotationally unstable |
| B3 | 61-B3 | Bilateral (windswept/LC-III) | Rotationally unstable |
| C1 | 61-C1 | Unilateral complete disruption | Rotationally + vertically unstable |
| C2 | 61-C2 | Bilateral (one B, one C) | Rotationally + vertically unstable |
| C3 | 61-C3 | Bilateral complete disruption | Rotationally + vertically unstable |
Clinical Pearls
- Type B vs C distinction is the most critical: check for vertical displacement on AP pelvis X-ray (hemipelvis riding up = C-type).
- Symphysis >2.5 cm on X-ray = sacrospinous rupture = at minimum Type B1.
- Type C injuries have the worst outcomes, primarily due to associated neurologic injuries (S1-S3 nerve roots, cauda equina).
- Hemorrhage risk increases with injury severity: Tile B and C injuries are associated with high transfusion requirements and hemodynamic instability.
- Open-book injuries (B1) increase pelvic volume - circumferential binder placed at the level of the greater trochanters (not the iliac crests) reduces volume and tamponades venous bleeding.
Sources: Campbell's Operative Orthopaedics 15th Ed 2026, p. 3530-3531; Rockwood & Green's Fractures in Adults 10th Ed 2025, p. 2328-2329
Young and burges classification of pelvis with images explain
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I now have all the images and content needed for a detailed, image-rich explanation. Here is the complete guide:
Young-Burgess Classification of Pelvic Fractures
Introduced by Young and Burgess (1987), this is the most widely used classification for pelvic ring injuries. It is based on the mechanism of injury (force vector) rather than stability alone. It has four main types: LC, APC, VS, and CM.
Sources: Rockwood & Green's Fractures in Adults 10th Ed 2025; Miller's Review of Orthopaedics 9th Ed; Campbell's Operative Orthopaedics 15th Ed 2026
Classification Overview Diagram
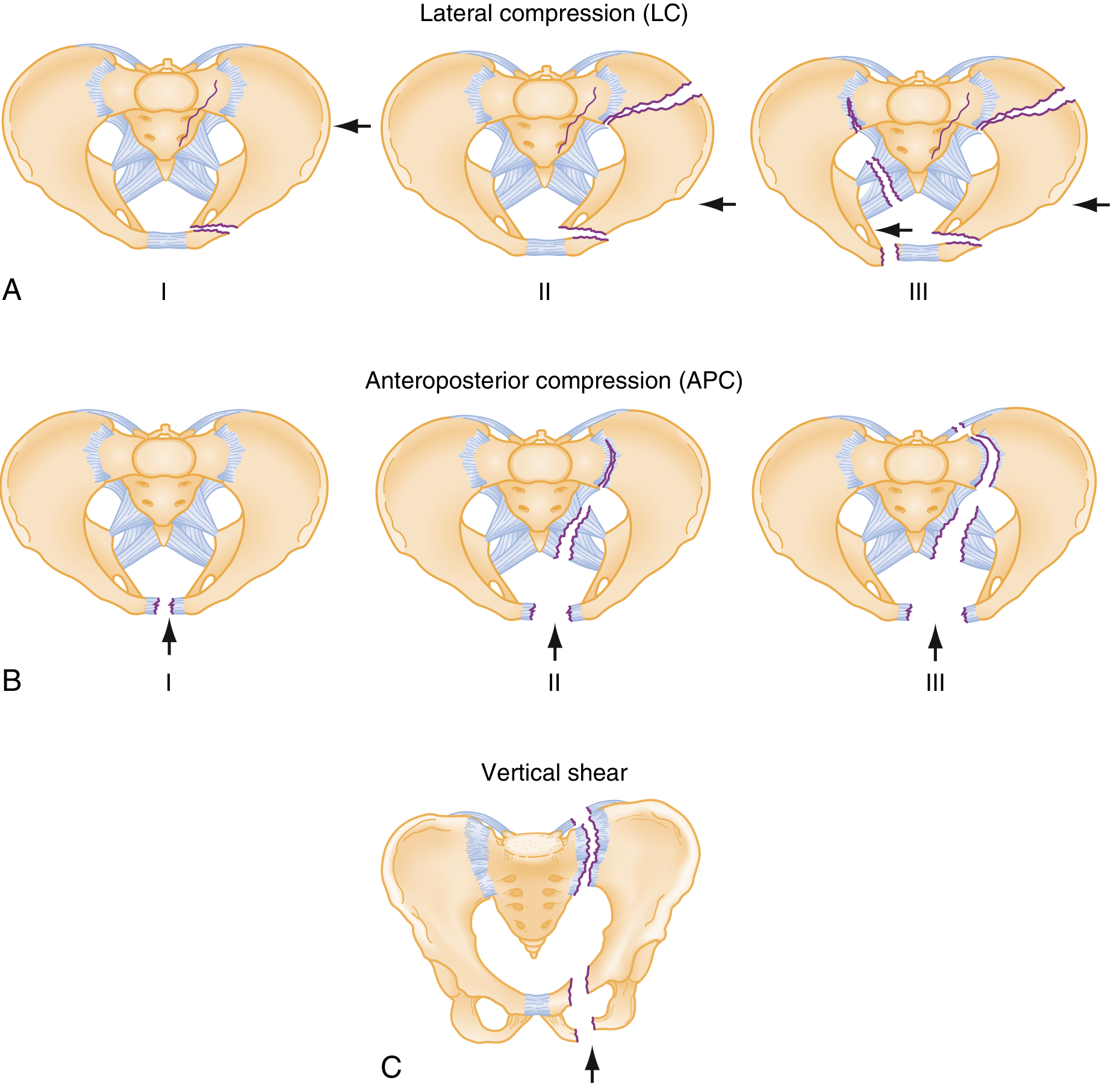
Fig. 11.6 from Miller's Review of Orthopaedics - The three main injury vectors. Arrows indicate direction of applied force.
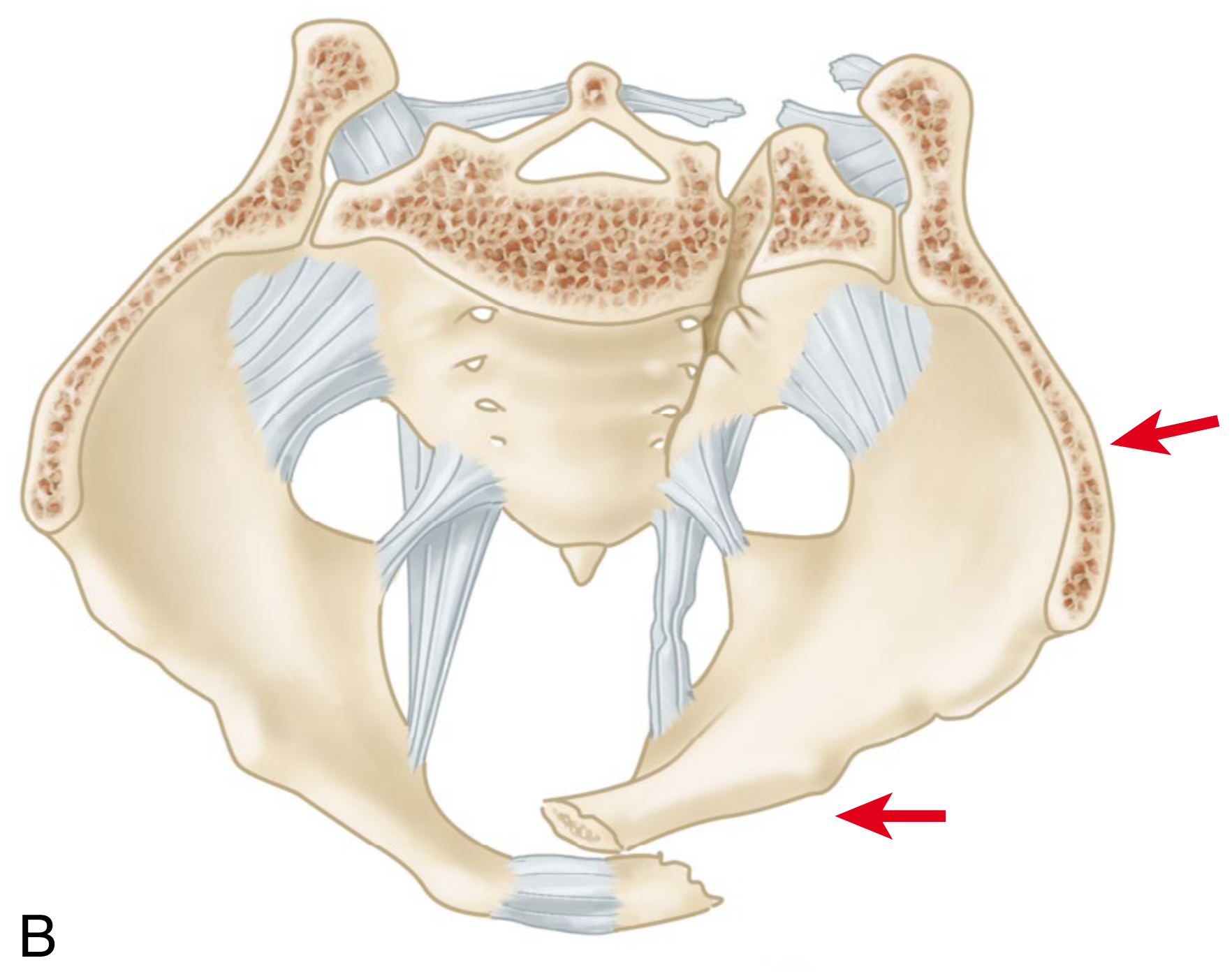
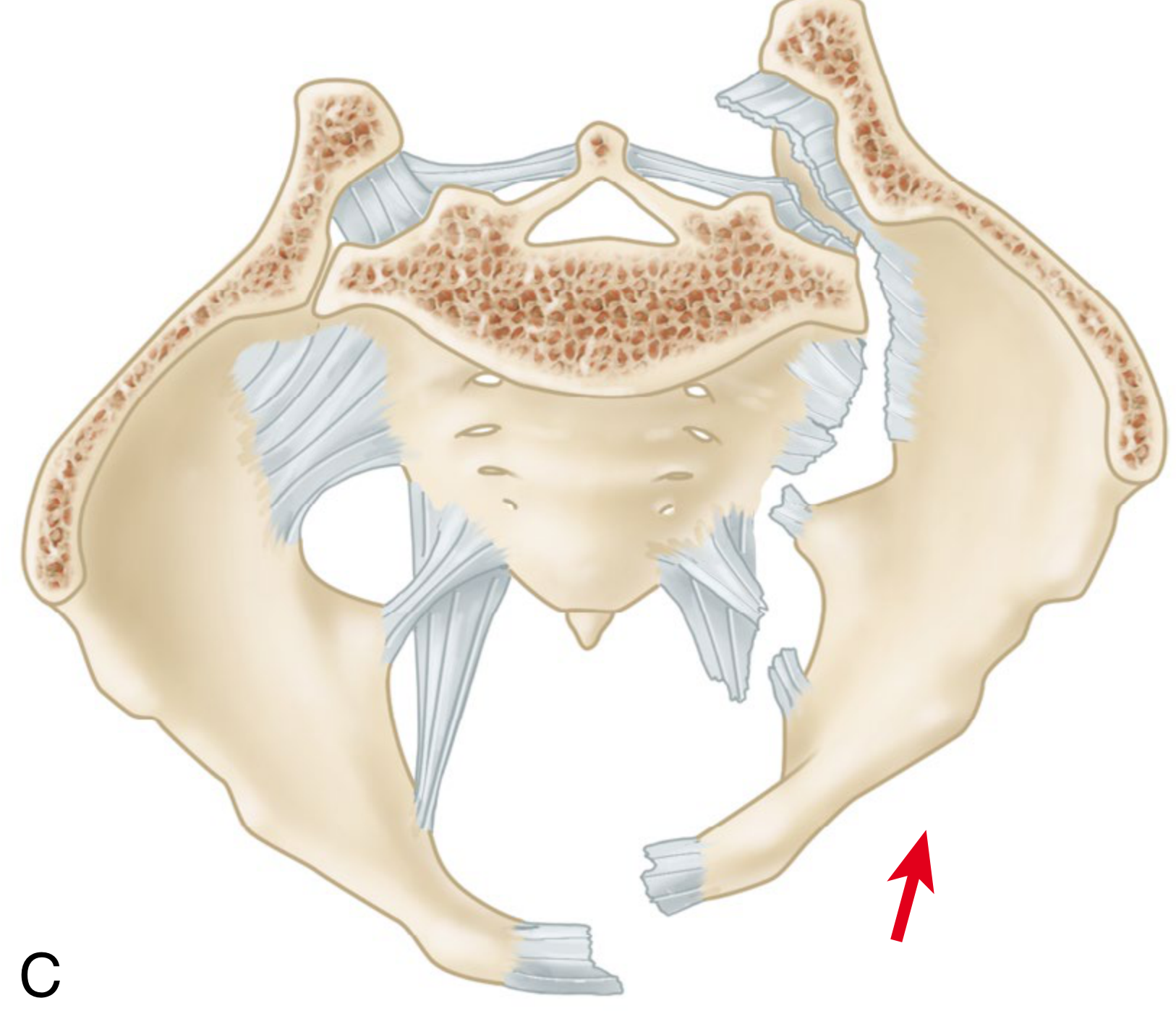
TYPE 1: LATERAL COMPRESSION (LC) - Most Common (~41%)
Mechanism: Side-impact force causing internal rotation of the hemipelvis. Classic cause: T-bone motor vehicle collision, direct blow to the side.
Anterior injury: Oblique/horizontal pubic rami fractures (ipsilateral)

| Subtype | Posterior Injury | Ligaments | Stability | Tile Equivalent |
|---|---|---|---|---|
| LC I | Sacral impaction fracture on side of impact (sacral ala crushed) | Intact | Rotationally stable | B2.1 |
| LC II | Crescent fracture - fracture-dislocation of iliac wing through SI joint | Partially disrupted | Rotationally unstable | B2.3 |
| LC III | LC I or II on side of impact + contralateral open-book (windswept pelvis) | Contralateral SS/ST disrupted | Unstable | B3.2 |
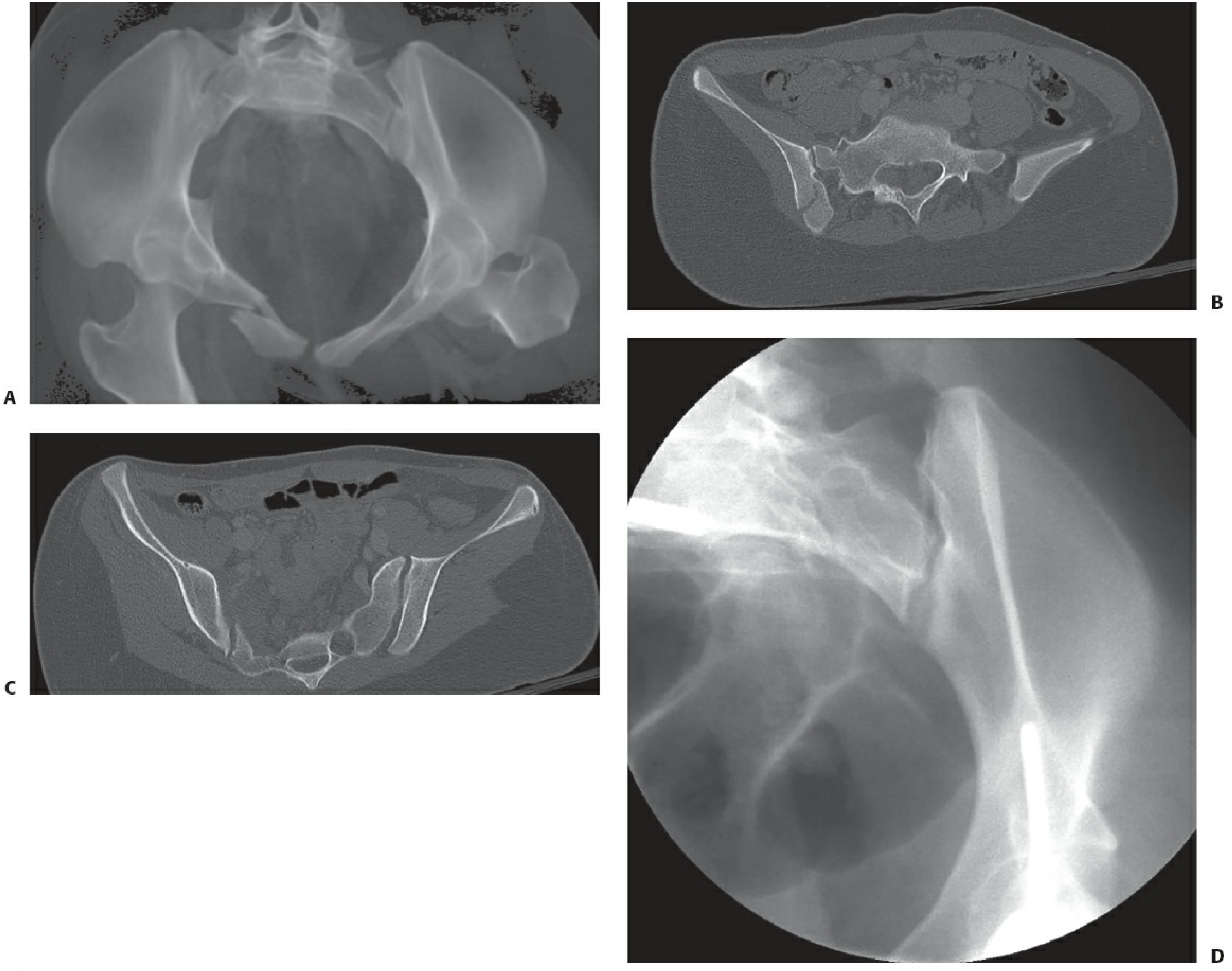
LC-III "windswept pelvis" - Note ipsilateral sacral fracture entering the SI joint (crescent fracture), with contralateral SI joint widening on stress examination (panel D)
Associated injuries: Brain injury (LC-I, LC-II), bowel injury (LC-III). LC-III is usually from a crush injury.
TYPE 2: ANTEROPOSTERIOR COMPRESSION (APC) - "Open Book" (~26%)
Mechanism: Force applied front-to-back causing external rotation of the hemipelvis - hinged posteriorly at the SI joint. Causes: head-on collision, motorcycle accident, fall landing on extended leg.
Anterior injury: Symphysis pubis diastasis or rami fractures
Ligament failure progresses in a domino pattern: Symphysis → Sacrospinous → Sacrotuberous → Anterior SI ligament → Posterior SI ligament
| Subtype | Symphysis | Ligaments Disrupted | SI Joint | Tile Equivalent |
|---|---|---|---|---|
| APC I | <2.5 cm diastasis | Symphysis only; posterior ligaments intact | Minor anterior opening | A2/B1 |
| APC II | >2.5 cm diastasis | Sacrospinous + Sacrotuberous + Anterior SI | Anterior SI opens; posterior SI intact | B1 |
| APC III | Wide diastasis | ALL ligaments including posterior SI | Complete disruption | C1 |
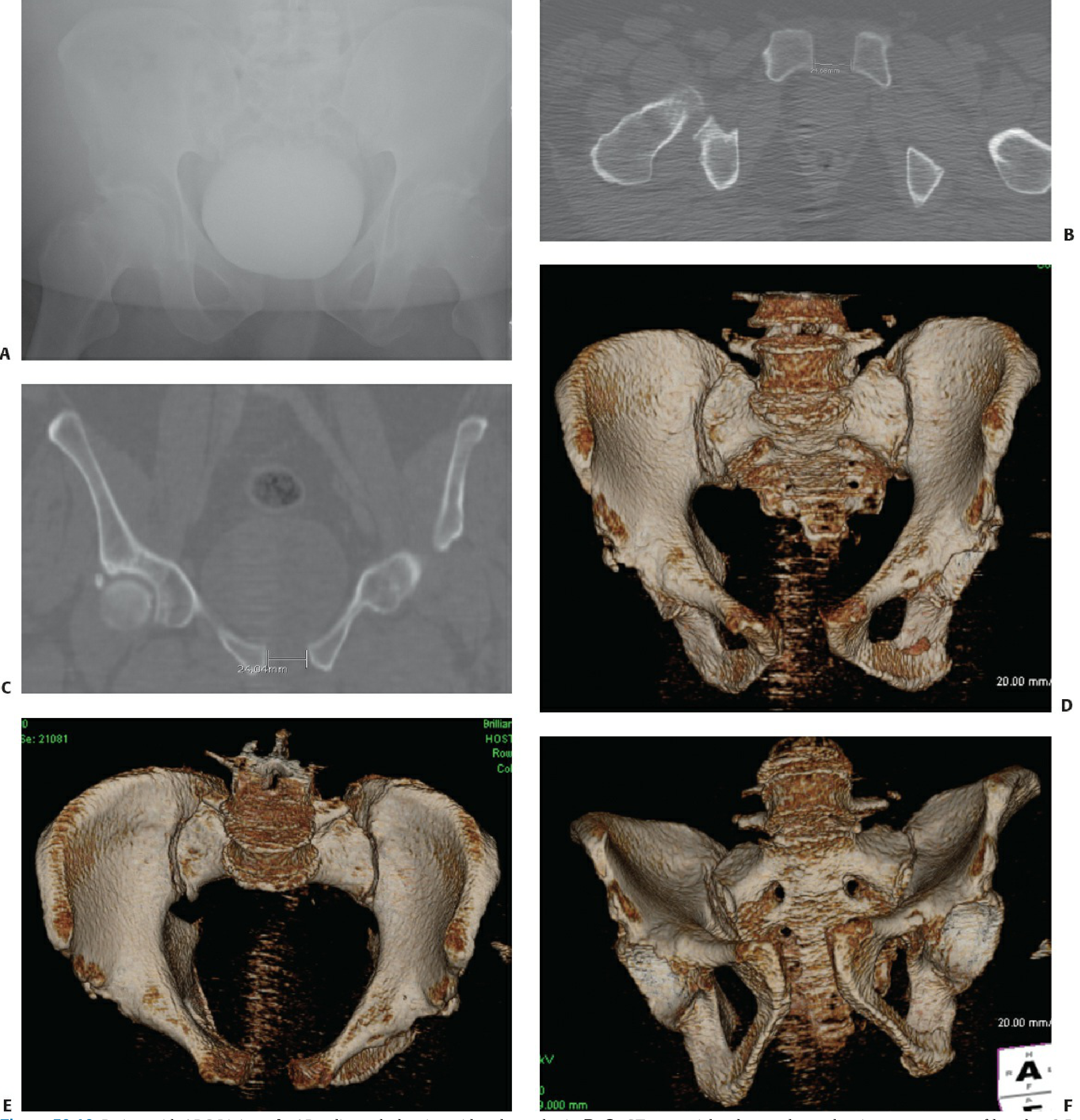
APC I: Note the symphysis widening on AP X-ray (A), CT measuring <2.5 cm diastasis (B,C), and 3D CT reconstructions showing the externally rotated hemipelvis (D-F)
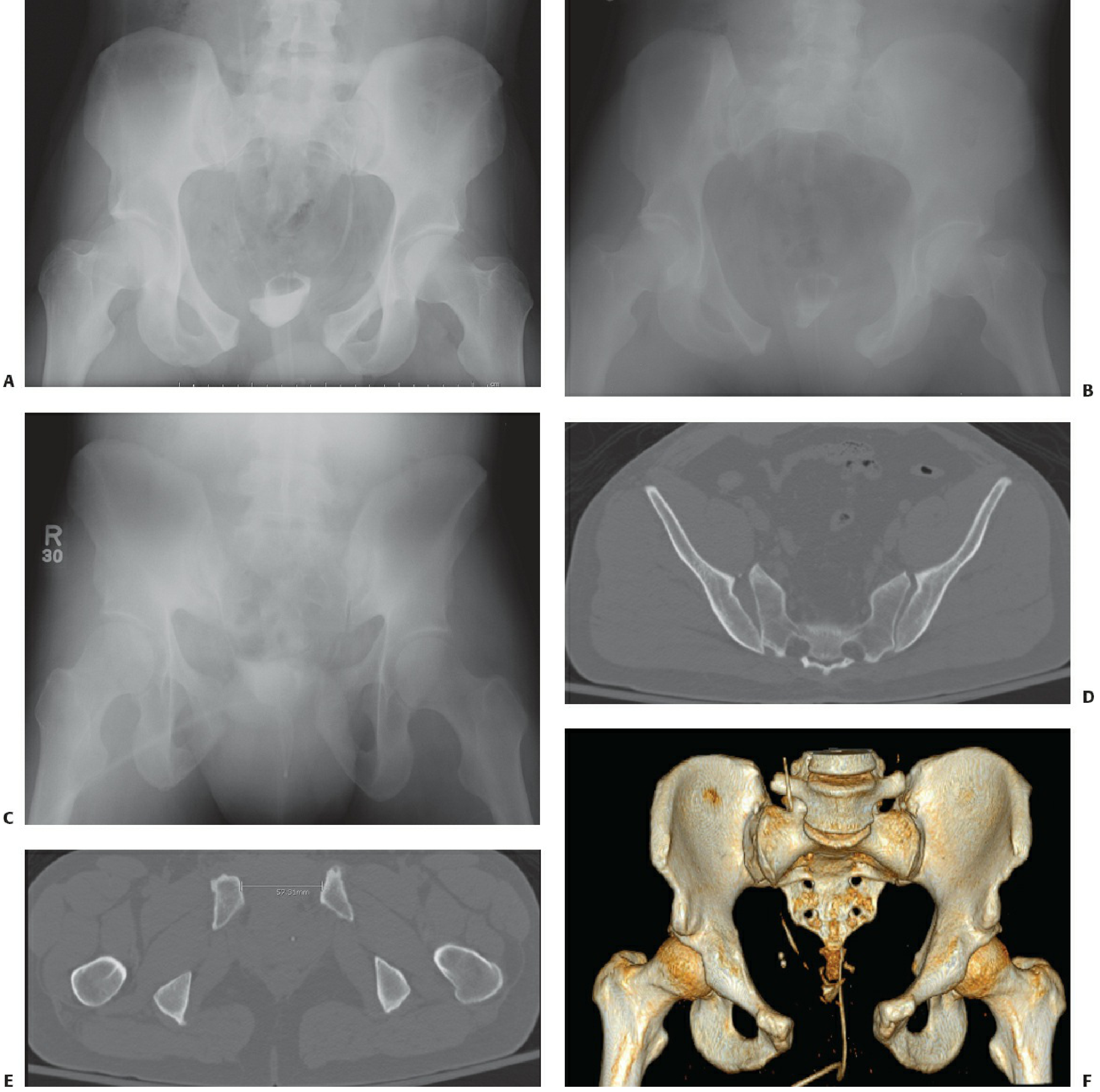
APC II: AP, inlet, and outlet radiographs (A-C), axial CT showing right SI joint widening (D), CT measuring 5.7 cm diastasis (E), 3D reconstruction (F)
Key rule: Symphysis >2.5 cm = sacrospinous ligament disrupted = at least APC II
Associated injuries: Urethral/bladder injuries (most common in APC), splenic/liver/bowel/vascular injuries increase APC I → III. APC III has the highest transfusion requirements of all types.
TYPE 3: VERTICAL SHEAR (VS) - (~5%)
Mechanism: Vertical force directed cephalad through one lower extremity - the hemipelvis is displaced superiorly. Cause: fall from height, high-energy impact.
Injuries: Complete disruption of ALL pelvic ligaments (equivalent to APC III). Vertical displacement of entire hemipelvis.
Anterior injury: Vertical rami fractures or symphysis diastasis
Posterior injury: Iliac wing fracture, sacral fracture, or SI joint dislocation
Key radiographic clue: Iliac crest on the injured side rides cephalad (higher) compared to the normal side on AP pelvis. L5 transverse process fracture (avulsion by iliolumbar ligament) may indicate vertical instability.
Tile equivalent: C1 (most severe single-sided pattern)
Associated injuries: Mortality and injury pattern similar to APC II and APC III.
TYPE 4: COMBINED MECHANISM (CM) - (~10%)
Mechanism: Multiple force vectors acting simultaneously. These injuries exhibit features from two or more of the above patterns.
Examples: LC + VS, APC + LC (the latter producing the "windswept" appearance)
Stability: Variable - determined by the components present.
3D CT of a Severe Pelvic Ring Injury
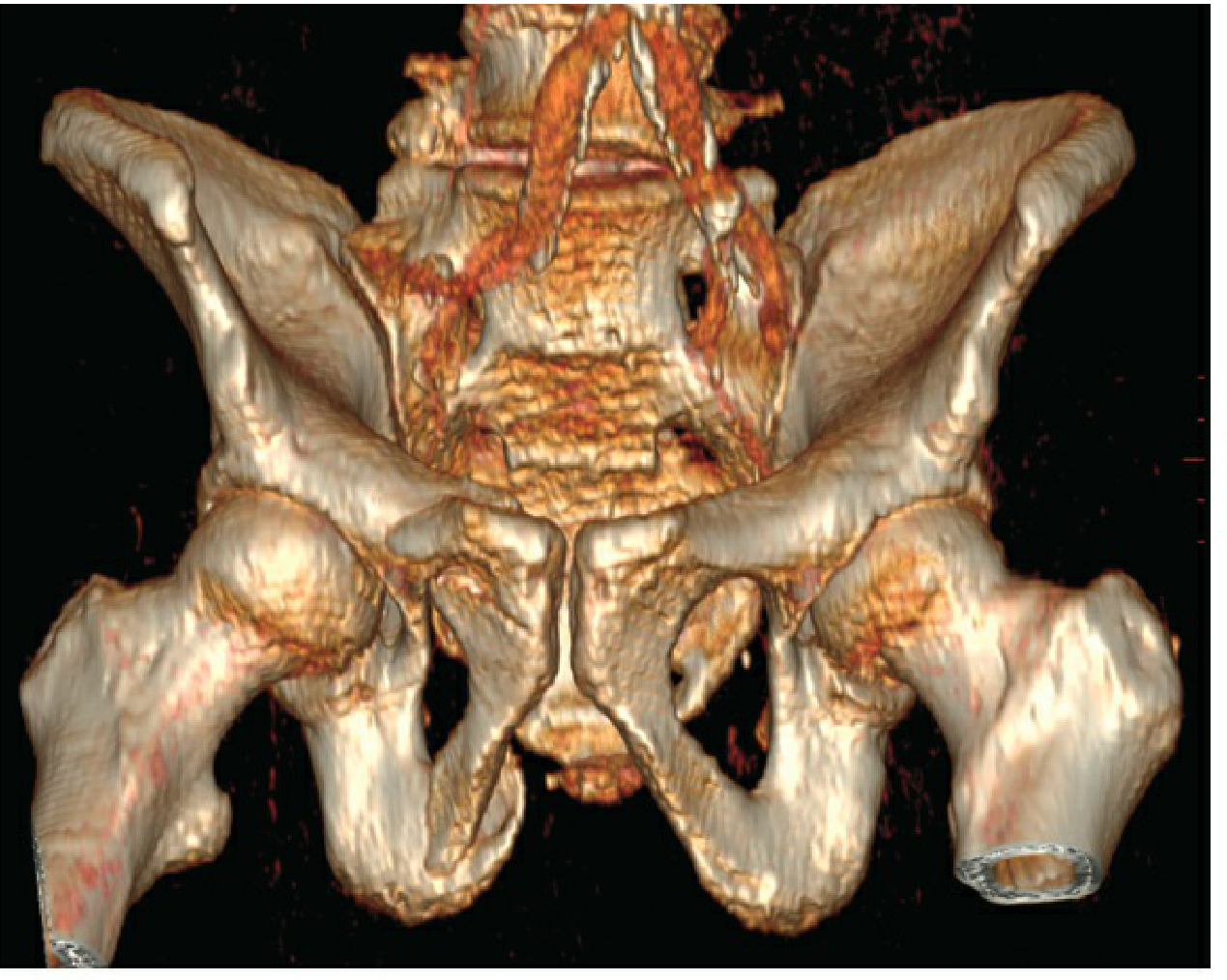
3D CT reconstruction illustrating a high-energy pelvic ring disruption - essential for pre-operative planning
Full Classification Summary Table
| Type | Subtype | Mechanism | Anterior Injury | Posterior Injury | Ligaments | Hemorrhage Risk | Tile |
|---|---|---|---|---|---|---|---|
| LC I | Lateral compression | Side impact (internal rotation) | Horizontal rami # | Sacral impaction | Intact | Low | B2.1 |
| LC II | Lateral compression | Side impact | Horizontal rami # | Crescent fracture (iliac wing-SI) | Partial | Moderate | B2.3 |
| LC III | Lateral compression | Crush / T-bone | Rami ± symphysis | LC + contralateral APC (windswept) | Bilateral | High | B3.2 |
| APC I | Open book | AP force | Symphysis <2.5 cm | None/minimal | Symphysis only | Low | A2/B1 |
| APC II | Open book | AP force | Symphysis >2.5 cm | Anterior SI opens | SS + ST + Ant. SI | High | B1 |
| APC III | Open book | AP force | Wide diastasis | Complete SI disruption | All (including post. SI) | Highest | C1 |
| VS | Vertical shear | Fall from height | Vertical rami/symphysis | SI dislocation/sacral # | All disrupted | High | C1 |
| CM | Combined | Variable | Variable | Variable | Variable | Variable | B/C |
Clinical Pearls
- LC injuries are most common (41%) but APC injuries bleed more (pelvic volume increases with external rotation).
- APC II vs APC III distinction is key: APC II has intact posterior SI ligaments - so anterior fixation (symphyseal plate) alone may suffice. APC III needs posterior fixation too.
- VS injuries are easiest to miss - always check if one hemipelvis rides higher than the other on AP X-ray.
- Circumferential pelvic binder is most effective for APC injuries (reduces pelvic volume). It is LESS effective for VS (no volume reduction needed).
- Transfusion prediction: APC III > VS > LC III > APC II; LC I and APC I have minimal blood loss.
- The Young-Burgess system predicts associated injuries better than Tile, while Tile is better for guiding surgical fixation strategy.
Sources: Rockwood & Green's Fractures in Adults 10th Ed 2025, pp. 2328-2332; Miller's Review of Orthopaedics 9th Ed, p. 907
This is a shared conversation. Sign in to Orris to start your own chat.