Case sheet for surgery
Asking for Preferences
Reading File
Finding Sources
Searching the Web
pre-operative assessment case sheet components surgery
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Here is a complete explanation of all components of a pre-operative assessment case sheet in surgery, drawn from Schwartz's Principles of Surgery (11e) and Miller's Anesthesia (10e):
Pre-Operative Assessment Case Sheet - Components Explained
A pre-op case sheet is a structured document that risk-stratifies the patient, identifies modifiable problems, and guides anesthetic and surgical planning. It has the following major sections:
1. Patient Identification
- Name, age, sex, date of admission
- Unit/bed number, hospital registration number
- Date of surgery, name of operating surgeon and anaesthetist
2. Chief Complaint (CC)
- The primary reason the patient is presenting for surgery, stated in the patient's own words, with duration
- Example: "Swelling in the right lower abdomen for 3 months"
3. History of Presenting Illness (HPI)
A detailed chronological account covering:
- Onset, duration, character, and progression of symptoms
- Aggravating and relieving factors
- Previous episodes and treatment received
- Symptoms relevant to likely diagnosis (e.g., for a bowel case - change in bowel habit, blood in stool, weight loss)
4. Past Medical History (PMH)
- Known comorbidities: hypertension, diabetes mellitus, ischemic heart disease, COPD, renal disease, liver disease
- Previous hospitalizations
- Prior surgeries and any complications during those surgeries (bleeding, anaesthetic problems)
- History of deep vein thrombosis or pulmonary embolism (relevant for VTE risk)
5. Drug History
- Current medications with doses - especially:
- Anticoagulants (warfarin, heparins, NOACs) - need bridging or reversal
- Antiplatelet agents (aspirin, clopidogrel) - may need to be stopped
- Insulin and oral hypoglycaemics - perioperative glucose management protocols
- Antihypertensives, ACE inhibitors, ARBs
- Steroids - need stress dosing
- Herbal supplements - many affect bleeding (garlic, ginseng, ginkgo)
6. Allergy History
- Documented drug allergies with the nature of the reaction (rash vs. anaphylaxis)
- Latex allergy (important for OT preparation)
- Food allergies (especially shellfish if iodine-based contrast is planned)
7. Personal History
- Smoking: pack-year history (impacts pulmonary risk and wound healing)
- Alcohol use: chronic use affects anaesthetic dosing and liver function
- Substance use: opioids, benzodiazepines affect anaesthetic management
- Occupation and activity level (used to estimate functional capacity)
8. Family History
- History of anaesthetic complications in family: malignant hyperthermia, pseudocholinesterase deficiency
- Bleeding disorders (haemophilia, von Willebrand disease)
- Cardiovascular disease, diabetes, malignancy
9. Menstrual and Obstetric History (in females)
- Last menstrual period (LMP) - rule out pregnancy before surgery and anaesthesia
- Parity, previous caesarean sections (relevant for pelvic/abdominal surgery)
- Oral contraceptive pill use (thromboembolism risk)
10. Review of Systems (Systemic Enquiry)
A structured head-to-toe screen for undetected comorbidities:
| System | Key Questions |
|---|---|
| Cardiovascular | Chest pain, dyspnoea, orthopnoea, ankle swelling, palpitations |
| Respiratory | Cough, wheeze, exertional dyspnoea, recent URTI |
| Neurological | Seizures, TIA, stroke, motor/sensory deficits |
| Renal | Oliguria, haematuria, known CKD |
| Hepatic | Jaundice, ascites, easy bruising |
| Endocrine | Symptoms of uncontrolled DM, thyroid disease |
| Haematological | Easy bruising, prolonged bleeding after cuts, anaemia symptoms |
11. Physical Examination
General
- Build, nutrition, pallor, icterus, cyanosis, clubbing, lymphadenopathy, oedema
- Weight, height, BMI - important for drug dosing and VTE risk
Vital Signs
- Blood pressure (both arms if cardiovascular history)
- Heart rate, respiratory rate, SpO2 on room air
- Temperature
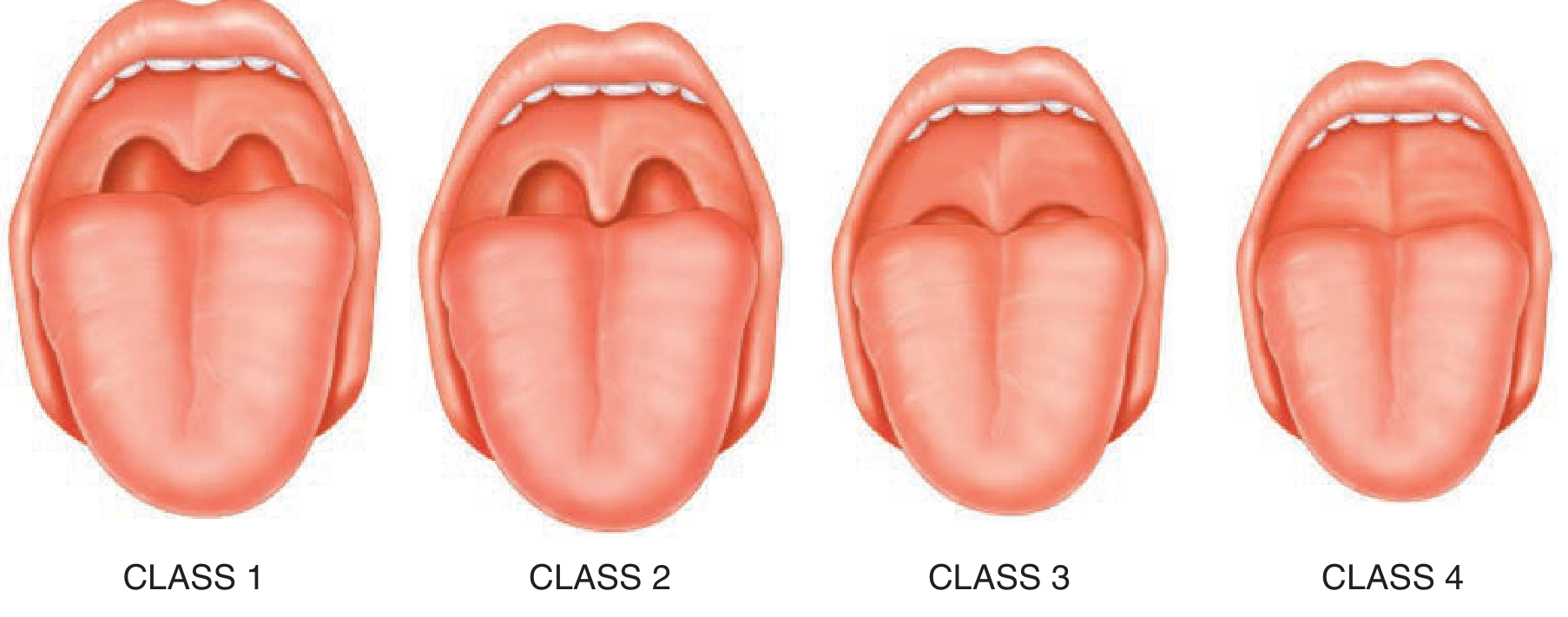
Airway Assessment (mandatory pre-op)
Per Schwartz's, the airway exam must screen for anticipated difficult intubation:
- Mallampati classification (Class 1-4 based on visible oropharyngeal structures)
- Mouth opening (normal >4 cm or 3 finger-breadths)
- Thyromental distance (normal >6 cm - less than 6 cm predicts difficult intubation)
- Neck mobility and circumference
- Presence of large overbite, small mandible, limited jaw protrusion
- Obesity is an independent risk factor for both difficult intubation and difficult mask ventilation
Cardiovascular Examination
- JVP, pulse character, cardiac auscultation (murmurs, added sounds)
- Peripheral vascular status
Respiratory Examination
- Chest expansion, percussion, auscultation
Abdominal Examination
- Specific to the surgical problem plus general assessment (hepatosplenomegaly, ascites)
Neurological Examination
- Baseline motor and sensory function (especially for spine/regional anaesthesia cases)
12. ASA Physical Status Classification
This is recorded on every pre-op assessment. It risk-stratifies the patient for anaesthesia and surgery:
| ASA Class | Definition |
|---|---|
| I | Healthy patient, no systemic disease |
| II | Mild systemic disease, no functional limitation |
| III | Severe systemic disease with functional limitation |
| IV | Severe systemic disease that is a constant threat to life |
| V | Moribund patient not expected to survive without surgery |
| VI | Brain-dead patient for organ donation |
| E suffix | Emergency surgery (e.g., ASA IIE) - increases risk |
(Schwartz's Principles of Surgery, 11e)
13. Functional Status Assessment
- Measured in METs (Metabolic Equivalents)
- Patients who cannot achieve 4 METs are considered poor functional status and may need further cardiac workup before surgery
- 4 METs = walking up a flight of stairs, climbing a hill, or walking at 3-4 mph on level ground
- This directly determines whether further pre-operative cardiac investigations are needed (ACC/AHA guidelines)
14. Investigations
Routine / Baseline
| Investigation | Purpose |
|---|---|
| CBC / haemogram | Anaemia, infection, thrombocytopaenia |
| Blood group and crossmatch | Preparation for transfusion |
| Blood glucose / HbA1c | Diabetes screening and control (elevated HbA1c increases surgical infection risk) |
| Serum electrolytes (Na, K, Cl, HCO3) | Electrolyte balance |
| Renal function tests (BUN, creatinine) | Baseline - drug dosing, contrast use |
| Liver function tests | Coagulopathy risk, drug metabolism |
| Coagulation profile (PT, aPTT, INR) | Bleeding risk |
| Urinalysis | Infection, proteinuria |
| ECG | Baseline cardiac assessment (mandatory >40 years or cardiac history) |
| Chest X-ray | Cardiorespiratory baseline |
Targeted / Specialty-Based
- Echocardiogram - if cardiac murmur or reduced functional status
- Pulmonary function tests - for thoracic surgery or significant lung disease
- Serum albumin - marker of nutritional status and wound healing risk
- Pregnancy test (urine beta-hCG) - all women of reproductive age
- Imaging relevant to the planned procedure (CT, MRI, ultrasound)
15. Cardiac Risk Assessment
The Revised Cardiac Risk Index assesses risk of major adverse cardiac events (MACE) and incorporates six factors:
- History of ischaemic heart disease
- Congestive cardiac failure
- Cerebrovascular disease
- Insulin-dependent diabetes mellitus
- Chronic kidney disease (baseline creatinine >2 mg/dL)
- High-risk surgery: major vascular, intraperitoneal, or intrathoracic
(Schwartz's Principles of Surgery, 11e, p. 2062)
16. Thromboembolism Risk Assessment
- Caprini or Wells score for DVT/PE risk
- Determines whether pharmacological prophylaxis (low-molecular-weight heparin) and/or mechanical prophylaxis (compression stockings, sequential compression devices) are needed
17. Preoperative Fasting Status (NPO Status)
Per ASA guidelines:
| Time Before Surgery | Permitted |
|---|---|
| Up to 8 hours | Food and fluids freely |
| Up to 6 hours | Light meal (toast, crackers), infant formula |
| Up to 4 hours | Breast milk |
| Up to 2 hours | Clear liquids only |
- Patients at high aspiration risk (GORD, gastroparesis, achalasia, bowel obstruction) need rapid sequence induction regardless of fasting status.
18. Consent
- Documented informed consent for the surgical procedure
- Discussion of the procedure, alternatives, risks (general and specific), and benefits
- Anaesthetic consent (separate in many institutions)
- For patients with DNR/DNI orders, pre-operative discussion must clarify whether these orders apply in the perioperative period
19. Anaesthetic Plan / Pre-operative Orders
- Type of anaesthesia planned: general, regional, local with sedation
- Airway plan including backup plan for anticipated difficult airway
- Blood product orders
- Antibiotic prophylaxis (type, dose, timing - typically within 60 minutes of incision)
- DVT prophylaxis plan
- Glucose management protocol (for diabetics)
- Instructions for regular medications (what to hold, what to give on the morning of surgery)
20. Pre-operative Risk Summary
A brief summary note documenting:
- ASA class
- Cardiac risk (Revised Cardiac Risk Index)
- Airway classification (Mallampati)
- Key comorbidities and whether they are optimized
- Any outstanding issues (e.g., "cardiology review awaited", "INR to be rechecked")
- Plan: "Proceed / Delay / Optimize and reschedule"
Sources:
- Schwartz's Principles of Surgery, 11e - Chapter 46 (Anesthesia for the Surgical Patient)
- Miller's Anesthesia, 10e - Chapter 29 (Preoperative)
Types of fever
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Here is a complete, structured overview of the Types of Fever as taught in clinical medicine:
Types of Fever
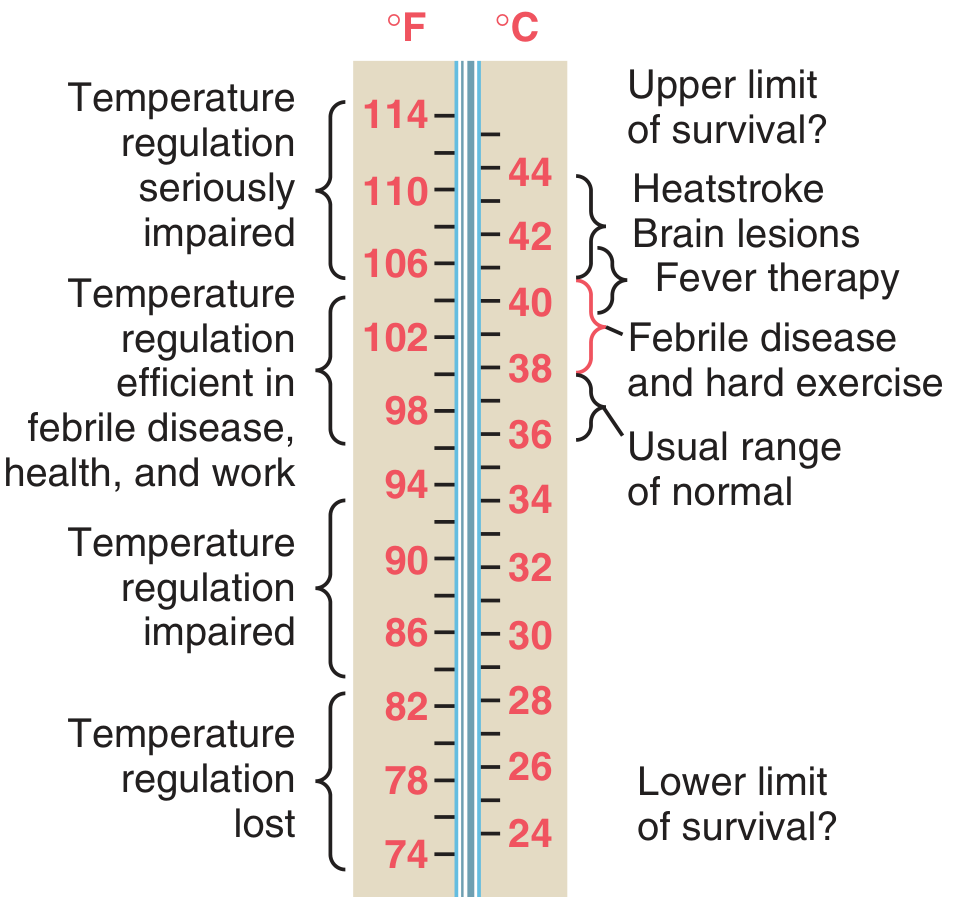
Definition
Fever (pyrexia) is a body temperature above the normal range (36-37.2°C / 97-99°F). The hypothalamus acts as a thermostat; when pyrogens (exogenous such as bacterial LPS, or endogenous such as IL-1, IL-6, TNF-alpha) raise the set point, the body generates heat through vasoconstriction and shivering to reach this new level.
The mechanism: Pyrogens --> macrophage activation --> release of IL-1, PGE2 --> hypothalamic set point raised --> fever.
Fever is distinct from hyperthermia, where body temperature rises uncontrolled without a raised hypothalamic set point (e.g., heatstroke, malignant hyperthermia, NMS).
A. Classification by Temperature Degree
| Grade | Temperature |
|---|---|
| Low-grade fever | 37.3 - 38°C (99.1 - 100.4°F) |
| Moderate fever | 38 - 39°C (100.4 - 102.2°F) |
| High fever | 39 - 40°C (102.2 - 104°F) |
| Hyperpyrexia | >41°C (>105.8°F) - medical emergency |
B. Classification by Fever Pattern (Most Important Clinically)
The pattern of fever charted over time on a temperature chart provides diagnostic clues. This is the most commonly tested classification in surgery and medicine.
1. Continuous (Sustained) Fever
- Temperature remains elevated throughout the day with diurnal variation of less than 1°C (i.e., never touches normal)
- Does NOT touch the normal baseline
- Examples: Lobar pneumonia, typhoid fever (classical), urinary tract infection, rickettsial infections
- Temperature typically 39-40°C throughout
2. Remittent Fever
- Temperature remains elevated throughout the day but diurnal variation exceeds 1°C
- Still does NOT touch normal baseline
- The most common type of fever seen in clinical practice
- Examples: Typhoid fever (more commonly), infective endocarditis, viral fevers, most bacterial infections
3. Intermittent Fever
- Temperature rises above normal and then comes down to normal (or below normal) every day
- The key feature: temperature touches the normal baseline between spikes
- Sub-types based on periodicity:
- Quotidian - fever spike every 24 hours (daily) - seen in Plasmodium falciparum malaria (also some cases of P. vivax), pyogenic abscesses
- Tertian - fever every 48 hours (3rd day cycle) - seen in P. vivax and P. ovale malaria
- Quartan - fever every 72 hours (4th day cycle) - seen in P. malariae malaria
4. Hectic (Septic / Swinging) Fever
- A very wide diurnal variation in temperature (>2°C), with the fever going very high and then coming down to normal or subnormal
- Usually accompanied by rigors (when rising) and profuse sweating (when falling)
- Characteristic of pyogenic (pus-forming) infections
- Examples: Pyogenic abscesses (liver abscess, subphrenic abscess), bacteraemia/septicaemia, tuberculosis (miliary or cavitating), infective endocarditis
5. Relapsing (Periodic) Fever
- Fever present for several days, followed by an afebrile period of several days, then fever returns
- Also called "undulant fever"
- Examples:
- Borrelia infections (relapsing fever) - fever lasts 3-6 days, then 7 days afebrile, then recurs
- Brucellosis (undulant fever) - classic undulating pattern
- Malaria (if untreated, can relapse)
- Hodgkin's lymphoma (Pel-Ebstein fever - a specific type of relapsing pattern)
6. Pel-Ebstein Fever
- A specific relapsing pattern: days to weeks of high fever alternating with days to weeks of normal temperature
- Classically described in Hodgkin's lymphoma
- Considered pathognomonic (though now recognized as uncommon even in Hodgkin's)
7. Inverse (Reverse) Fever
- Temperature is higher in the morning than in the evening
- The reverse of the normal diurnal pattern (normally, body temp is lowest in early morning and highest in late afternoon)
- Examples: Miliary tuberculosis, gram-negative septicaemia, liver abscess (occasionally)
C. Classification by Duration
| Type | Duration | Examples |
|---|---|---|
| Acute fever | <7 days | Viral URTI, malaria, UTI |
| Sub-acute fever | 7-21 days | Typhoid fever, brucellosis |
| Chronic / prolonged fever | >3 weeks | Tuberculosis, infective endocarditis, malignancy |
| Pyrexia of Unknown Origin (PUO) | >3 weeks, documented >38.3°C on multiple occasions, no diagnosis after 1 week of hospital investigation | TB, lymphoma, connective tissue diseases, occult infections |
D. Special / Named Fever Patterns
| Name | Disease |
|---|---|
| Saddle-back (biphasic) fever | Dengue fever - initial fever 3-5 days, brief remission, then second rise |
| Camel-back fever | Brucellosis |
| Undulant fever | Brucellosis |
| Pel-Ebstein fever | Hodgkin's lymphoma |
| Quotidian fever | P. falciparum malaria, JIA (systemic juvenile idiopathic arthritis) |
| Autumn fever | Leptospirosis |
E. Fever in the Surgical Context (Post-operative Fever)
Per Bailey and Love's Short Practice of Surgery (28e), about 40% of patients develop pyrexia after major surgery. The causes follow a classic time-based pattern remembered as the "5 W's":
| Post-op Day | Cause | Mnemonic |
|---|---|---|
| Day 1-2 | Wind - Atelectasis, chest infection | W |
| Day 3-5 | Water - Urinary tract infection | W |
| Day 4-6 | Wound - Surgical site infection | W |
| Day 5-7 | Walking - Deep vein thrombosis | W |
| Day 7+ | Wonder drugs - Drug fever, transfusion reaction | W |
Non-infective causes include: DVT, transfusion reactions, wound haematomas, atelectasis, and drug reactions.
F. Fever vs. Hyperthermia - Key Distinction
| Feature | Fever | Hyperthermia |
|---|---|---|
| Hypothalamic set point | Raised | Normal |
| Cause | Pyrogens (infection, inflammation) | Heat gain exceeds heat loss |
| Response to antipyretics | Yes - NSAIDs/paracetamol work | No - antipyretics ineffective |
| Examples | Infections, malignancy, autoimmune | Heatstroke, malignant hyperthermia, NMS |
| Treatment | Treat underlying cause + antipyretics | Cooling measures primarily |
Malignant hyperthermia (triggered by inhalational anaesthetics/suxamethonium), Neuroleptic Malignant Syndrome (NMS - from antipsychotics), and Serotonin Syndrome are important drug-induced hyperthermic states in the surgical and psychiatric contexts. (Bradley and Daroff's Neurology, p. 1058)
Sources:
- Guyton and Hall Textbook of Medical Physiology - Chapter 74 (Body Temperature Regulation and Fever)
- Bradley and Daroff's Neurology in Clinical Practice - Chapter 50 (Fever and Hyperthermia)
- Bailey and Love's Short Practice of Surgery, 28e - Chapter 24 (Post-operative fever)
Make a notes on Colo rectal cancer pathology 2nd year MBBS
Reading File
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.