Aortic dissection
Reading File
Finding Sources
Searching PubMed
"aortic dissection"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive material from multiple authoritative sources. Let me compile the complete, well-structured answer.
Aortic Dissection
Definition and Pathophysiology
Aortic dissection occurs when a tear in the aortic intima allows blood under systemic pressure to enter the media and split the laminar planes apart, creating a blood-filled false lumen within the aortic wall. The dissecting column of blood typically propagates distally (most common) but can also propagate proximally, or in both directions. In rare cases, disruption of the vasa vasorum causes an intramural hematoma without an identifiable intimal tear.
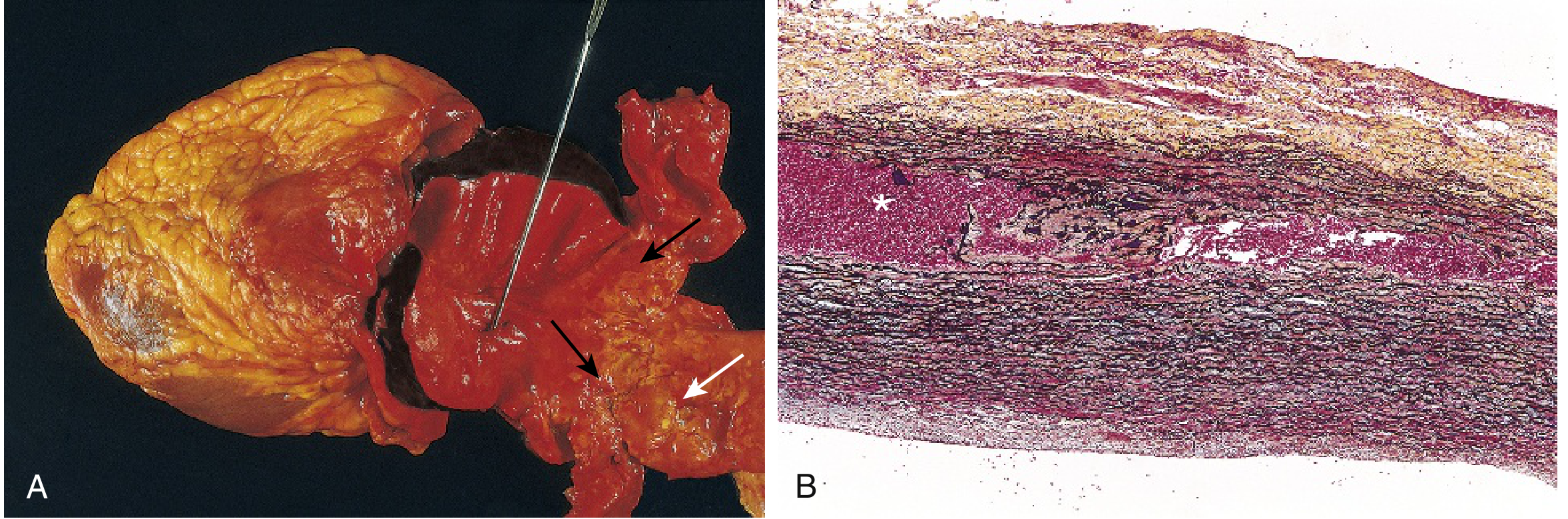
The two most common intimal tear sites are:
- The sinotubular junction of the ascending aorta (50-65% of cases) - where hydraulic shear stress is highest
- Just distal to the left subclavian artery (20-30%) at the junction of the arch and descending aorta
If blood dissects through the adventitia, rupture occurs and is nearly always rapidly fatal.
Epidemiology
- Incidence: 2.9-4.7 cases per 100,000 per year; 22% are undiagnosed prior to death
- Bimodal age distribution:
- Younger patients with connective tissue disorders (Marfan syndrome, Ehlers-Danlos syndrome type IV)
- Patients >50 years with chronic hypertension/atherosclerosis (the dominant group - >90% of cases)
- IRAD data: 65% are male, mean age 63; women present slightly older (mean 67)
- Hypertension coexists in 70% of patients
- Dissection is unusual in the presence of significant atherosclerosis, since medial fibrosis inhibits hematoma propagation
Risk Factors
| Category | Examples |
|---|---|
| Medial degeneration | Marfan syndrome, Ehlers-Danlos syndrome type IV, bicuspid aortic valve, copper metabolism defects |
| Hypertension | Most common (>90% of non-connective tissue cases) |
| Iatrogenic | Arterial cannulation, cardiopulmonary bypass, cardiac catheterization |
| Drugs | Cocaine, amphetamines (abrupt BP increase) |
| Pregnancy | 3rd trimester/perinatal - due to hormonal vascular remodeling + hemodynamic stress (~10-20 cases/million births) |
| Prior aortic surgery | Risk factor for recurrent dissection |
(Robbins & Kumar Basic Pathology, p. 325; Harrison's Principles 22E; Tintinalli's Emergency Medicine)
Classification
Stanford System (most clinically used)
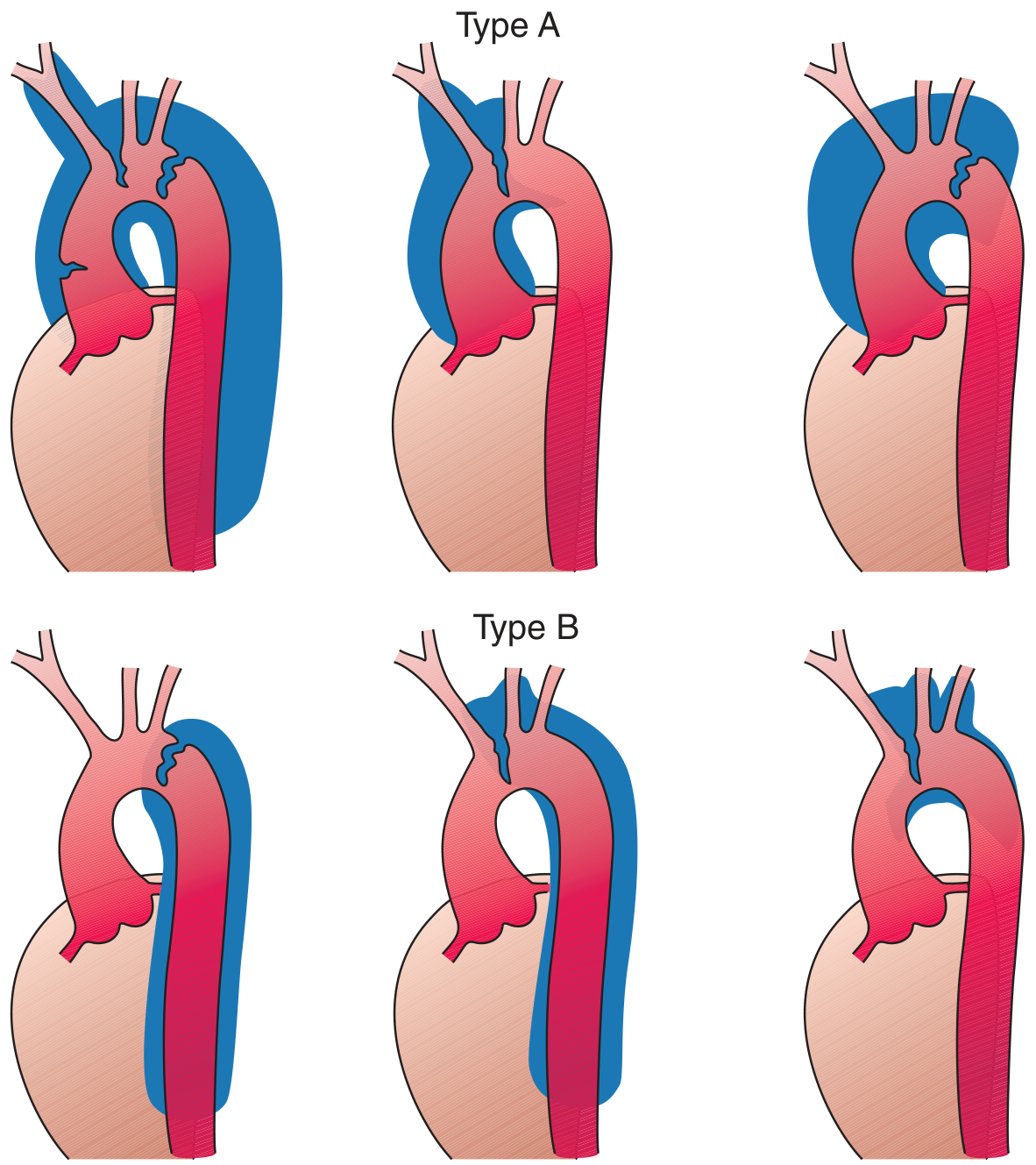
| Type | Definition | Frequency | Management |
|---|---|---|---|
| Type A | Involves the ascending aorta (regardless of tear origin or distal extent) | ~75% of cases | Emergency surgical repair |
| Type B | Limited to arch and/or descending aorta; ascending aorta NOT involved | ~25% of cases | Medical management (surgery/TEVAR for complications) |
DeBakey System
| Type | Description |
|---|---|
| Type I | Intimal tear in ascending aorta; dissection extends to arch and descending aorta (= Stanford A) |
| Type II | Limited to ascending aorta only (= Stanford A) |
| Type IIIa | Origin distal to left subclavian; limited to descending thoracic aorta |
| Type IIIb | Origin distal to left subclavian; extends below the diaphragm |
Stanford A = DeBakey I + II. Stanford B = DeBakey III. The Stanford classification is more practical for management decisions since DeBakey I and II are treated identically.
Clinical Presentation
Symptoms
- Classic presentation: Abrupt, severe "tearing" or "ripping" chest pain, often the worst pain the patient has ever experienced, radiating to the interscapular region
- 60% have anterior chest pain (more common in Type A); abdominal/back pain more common in Type B
- ~40% of patients (particularly in Asian populations) may present without chest pain
- Syncope occurs in ~10% - more common with Type A (tamponade/severe AR)
- Neurologic symptoms (stroke, paraplegia) occur in ~20% of Type A - marks poorer prognosis
Physical Examination Findings
| Finding | Frequency | Significance |
|---|---|---|
| Hypertension | 49% | Most common |
| Hypotension | 18-25% | Ominous - increases mortality |
| Pulse deficit (arm/leg) | 15% | Indicates branch vessel compromise |
| BP differential >20 mmHg between arms | Variable | Independently associated with dissection |
| Aortic insufficiency murmur | 32% | Retrograde propagation to aortic root |
| Neurologic deficit | ~20% (Type A) | Carotid involvement |
| Horner's syndrome, hoarseness, dysphagia | Rare | Compression of sympathetic ganglion, recurrent laryngeal nerve, esophagus |
IRAD Risk Score Categories (Tintinalli's Table 59-1 / AHA guidelines):
- Category 1 - Predisposing condition: Marfan syndrome, family history of aortic disease, bicuspid aortic valve, recent aortic manipulation
- Category 2 - Pain character: Abrupt onset, severe intensity, ripping/tearing quality
- Category 3 - Exam findings: Pulse deficit, focal neuro deficit + chest/back/abdominal pain, new aortic insufficiency murmur, shock/hypotension
(Tintinalli's Emergency Medicine, p. 454)
Acute Aortic Syndromes Spectrum
Aortic dissection is one of four major acute aortic syndromes:
- Aortic dissection - intimal tear with false lumen formation
- Intramural hematoma (IMH) - rupture of vasa vasorum into the media; crescentic/circumferential aortic wall thickening on non-contrast CT; no flow in false lumen; ~10-20% of acute aortic syndromes; majority occur in descending aorta
- Penetrating atherosclerotic ulcer (PAU) - plaque erosion through internal elastic lamina into media; mainly in mid/distal descending thoracic aorta; can progress to IMH, pseudoaneurysm, or rupture
- Aortic rupture - direct full-thickness tear; highly fatal
Diagnosis
Imaging Modalities
| Modality | Role | Notes |
|---|---|---|
| CT Angiography (CTA) | First-line, most widely used | Fast, available 24/7, high accuracy; caution with renal impairment in elderly |
| Transesophageal Echocardiography (TEE) | Alternative to CTA; excellent for ascending aorta and aortic valve involvement | Identifies intimal flap, true vs. false lumen flow, aortic regurgitation, pericardial effusion |
| MRI/MRA | Highest accuracy; used for chronic dissection follow-up | Not ideal in acute unstable patients |
| Transthoracic Echo (TTE) | Limited but useful at bedside | A "negative" TTE does NOT rule out dissection if clinical suspicion is high |
| Aortography | Rarely used; invasive | Largely replaced by CTA |
Echocardiographic diagnosis is secure when there is: (1) a dilated aortic lumen; (2) a linear, mobile echogenic structure (intimal flap) with motion different from the aortic wall; and (3) different color Doppler flow patterns in true vs. false lumen. (Textbook of Clinical Echocardiography)
Key ECG note: CTA should be obtained before thrombolytics in any patient with suspected MI who could have dissection - thrombolytics in the setting of dissection are catastrophic.
Management
Immediate Medical Therapy (All Patients)
The immediate goal is to reduce dP/dt (rate of pressure rise with each cardiac contraction):
Step 1 - Heart rate control first:
- IV beta-blocker (e.g., esmolol - 500 mcg/kg bolus, then 0.05-0.2 mcg/kg/min)
- Target HR <60 bpm
- Beta-blockers must be given BEFORE vasodilators to prevent reflex tachycardia
Step 2 - Blood pressure reduction after HR controlled:
- Target SBP <110-120 mmHg (stricter than other hypertensive emergencies)
- Agents: sodium nitroprusside, nicardipine, or clevidipine - all rapidly titratable
- Labetalol (alpha + beta blocker): acceptable alternative, but long half-life (4-6h) limits titratability
- Diltiazem or verapamil: may be used but not ideal as monotherapy
(Rosen's Emergency Medicine)
Type A Dissection
- Emergency surgical repair is indicated in virtually all patients
- Mortality >50% within 48 hours if untreated
- Fatal complications without surgery: aortic rupture, cardiac tamponade, acute aortic regurgitation, acute MI
- In octogenarians with uncomplicated Type A: surgery associated with 63% 1-year survival vs. 45-62% hospital mortality with medical management alone
- Exception: complicated Type A (neurologic deficit, mesenteric ischemia, or CPR required) - medical management may be preferable
Type B Dissection
Uncomplicated Type B (no rupture, no branch vessel ischemia):
- Medical management preferred
- Maintain HR <60 bpm and SBP 100-120 mmHg with IV beta-blockers
- Both medical and emergency surgery have similar mortality rates in uncomplicated cases
Complicated Type B (persistent pain, progression, rupture, branch ischemia):
- Surgical mortality >50%; endovascular repair (TEVAR) preferred
- IRAD registry shows increasing use of endovascular repair
Endovascular options for Type B:
- Stent-graft placement - covers entry tear, promotes false lumen thrombosis, reduces risk of rupture (20-50% risk within 1-5 years without treatment)
- Stent insertion - for branch vessel ischemia from true lumen collapse
- Fenestration of the intimal flap - now less commonly used since stent grafts were introduced
- Early surgery recommended for Type B dissection in patients with Marfan syndrome
(Grainger & Allison's Diagnostic Radiology; Braunwald's Heart Disease)
Long-Term Follow-Up
- Serial CTA or MRI to monitor false lumen for aneurysmal dilatation and distal extension
- Required in both conservatively managed patients and after endovascular repair
Prognosis
- Without treatment, Type A mortality: >1% per hour in the first 24-48 hours
- 1-, 5-, and 10-year actuarial survival for operative patients: 92%, 77%, 57%
- Cocaine-related dissection: implicated in 0.5-37% of cases; average interval from cocaine use to symptom onset is 12 hours (range 0-24 hours)
- Hypotension at presentation carries an ominous prognosis in both age groups
Key Differentiating Points from Other Causes of Chest Pain
- Aortic dissection pain is maximal at onset (unlike STEMI which builds gradually)
- Pulse deficits and BP differentials between extremities are not seen in ACS
- D-dimer is often elevated but is non-specific; a negative D-dimer with an ADD (Aortic Dissection Detection) Risk Score of 0 may help exclude dissection
- Thrombolytics are contraindicated if dissection is suspected
- CXR may show mediastinal widening (~60%) or abnormal aortic contour, but a normal CXR does not exclude dissection
Sources: Braunwald's Heart Disease (10th ed.) | Harrison's Principles of Internal Medicine 22E | Robbins & Kumar Basic Pathology | Rosen's Emergency Medicine | Tintinalli's Emergency Medicine | Grainger & Allison's Diagnostic Radiology | Textbook of Clinical Echocardiography | Current Surgical Therapy 14e
This is a shared conversation. Sign in to Orris to start your own chat.