Peptic ulcer in very detail with reference to standard textbook
Reading File
Finding Sources
Finding Sources
Searching PubMed
"peptic ulcer"[MeSH Terms] AND "Helicobacter pylori"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have extensive, high-quality content from multiple authoritative textbooks. Let me compile the comprehensive answer.
Peptic Ulcer Disease - A Comprehensive Review
1. Definition
A peptic ulcer is a discrete mucosal defect extending through the muscularis mucosae into the submucosa or deeper, occurring in any part of the gastrointestinal tract exposed to acid-pepsin secretion. Although the name implies pepsin, acid is the true sine qua non - peptic ulcers do not occur in the complete absence of acid, and virtually all can be healed by rendering a patient achlorhydric with proton pump inhibitors (PPIs).
Bailey and Love's Short Practice of Surgery, 28th Edition
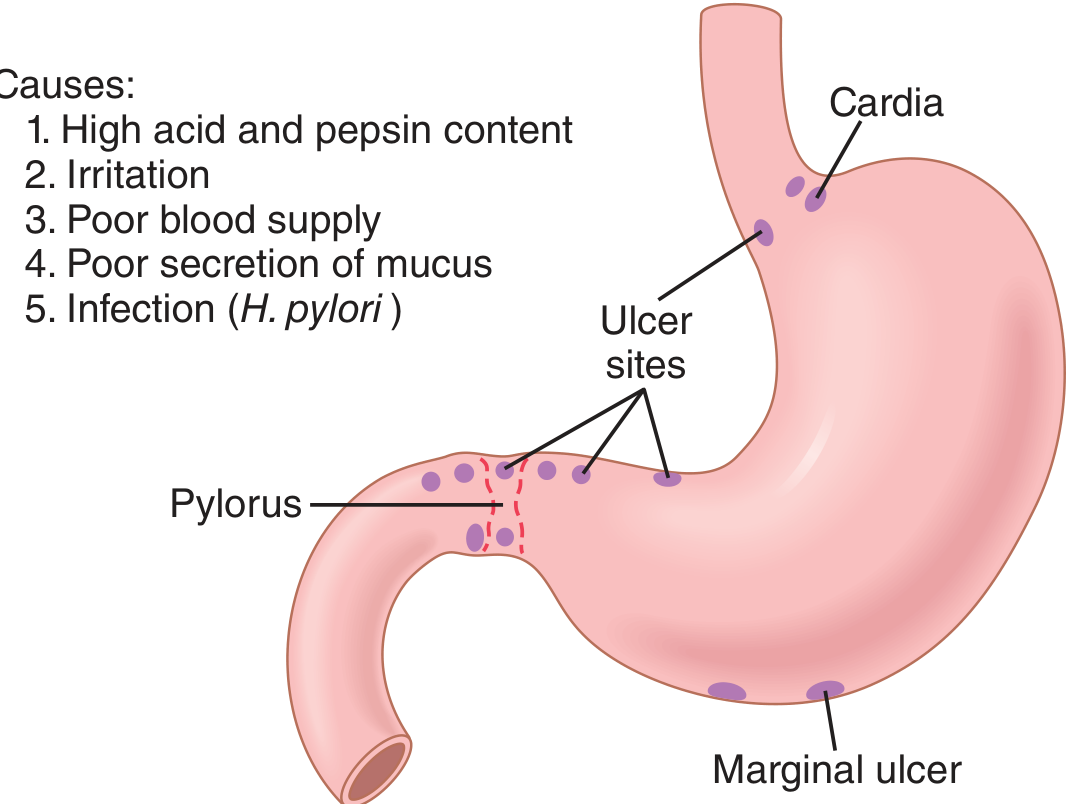
2. Sites of Occurrence
Common sites, in order of frequency:
- First part of the duodenum (most common, ~95% of duodenal ulcers within the duodenal cap)
- Gastric antrum / lesser curvature (especially at or near the angularis incisura)
- Prepyloric region
- Lower oesophagus (due to reflux of acid or ectopic gastric mucosa)
- Stomal (marginal) ulcers at gastrojejunostomy sites
- Meckel's diverticulum containing ectopic gastric epithelium
The ulcer forms at the junction between different epithelial types - where the mucosa is least resistant to acid damage.
3. Epidemiology
- Affects >4 million individuals in the United States annually
- Lifetime risk: approximately 10% for males and 4% for females
- More than 100,000 hospitalizations/year in the US related to bleeding peptic ulcer
- Duodenal ulcers are more common than gastric ulcers
- The incidence of H. pylori-associated ulcers is declining as eradication rates improve; NSAID-related ulcers are proportionally increasing, particularly in the elderly using low-dose aspirin
Robbins & Kumar Basic Pathology; Sleisenger and Fordtran's Gastrointestinal and Liver Disease
4. Aetiology and Risk Factors
4.1 Helicobacter pylori Infection
- >70% of PUD cases are associated with H. pylori infection
- H. pylori colonises the gastric antrum and first portion of the duodenum, causing chronic active gastritis as the background for ulceration
- Only 5-10% of infected individuals develop peptic ulcers, indicating a role for host factors and bacterial strain variation (e.g., CagA, VacA virulence factors)
- Mechanism of injury (Mulholland & Greenfield's Surgery):
- Endocrine effects: increased basal serum gastrin, increased gastrin response to meals, increased responsiveness to gastrin-releasing peptide, production of N-alpha-methylhistamine, decreased somatostatin cell density and mucosal somatostatin content
- Acid hypersecretion: increased basal and pentagastrin-stimulated acid output, abnormal gastric emptying
- Mucosal defense impairment: decreased duodenal bicarbonate production, decreased mucosal prostaglandin production, increased epithelial cell apoptosis, disrupted epithelial barrier function, inhibited epithelial restitution
- The bacterium physically burrows through the mucosal barrier and releases urease, generating ammonium that liquefies the mucous layer and stimulates HCl secretion
- Mucosal inflammatory cells and epithelial cells release cytokines (IL-8, IFN-gamma, TNF-alpha) which stimulate gastrin release from G cells
- After H. pylori eradication: basal acid output returns to normal within 4 weeks; peak acid output declines to normal by 6 months
4.2 NSAIDs and Aspirin
- NSAIDs block cyclooxygenase (COX) enzymes, reducing mucosal prostaglandin synthesis
- Prostaglandins normally stimulate mucus and bicarbonate secretion, maintain mucosal blood flow, and promote epithelial restitution
- NSAID use is now the most common cause of gastric ulcers in the US as H. pylori rates fall
- Low-dose aspirin use in the ageing population is a significant and growing contributor
4.3 Zollinger-Ellison Syndrome (Gastrinoma)
- Gastrin-secreting tumour (usually in the pancreas or duodenal wall) causes massive, constitutive acid hypersecretion
- Results in multiple peptic ulcerations in the stomach, duodenum, and even jejunum
- In gastrinoma, acid hypersecretion is the sole aetiological factor
- High BAO (often >30 mEq/h, consistently >15 mEq/h); BAO:MAO ratio >0.6
4.4 Other Contributing Factors
| Factor | Mechanism |
|---|---|
| Cigarette smoking | Reduces mucosal blood flow, impairs healing, increases nervous stimulation of secretory glands |
| Alcohol | Breaks down the mucosal barrier directly |
| High-dose corticosteroids | Suppress prostaglandin synthesis, impair mucosal repair |
| Alcohol-related cirrhosis | Systemic and local mucosal effects |
| Chronic renal failure | Hypercalcaemia stimulates gastrin production and acid secretion |
| Hyperparathyroidism | Same mechanism - hypercalcaemia drives gastrin and acid hypersecretion |
| Chronic obstructive pulmonary disease | Associated but mechanism unclear |
| Physiological/psychological stress | Impairs mucosal blood flow, gastric motility, and acid secretion |
Robbins & Kumar Basic Pathology; Guyton and Hall Medical Physiology; Mulholland & Greenfield's Surgery
5. Pathogenesis - The Mucosal Defence Model
Peptic ulceration results from an imbalance between aggressive factors and defensive mechanisms:
Aggressive Forces:
- Hydrochloric acid (H+)
- Pepsin
- Bile salts (duodenogastric reflux)
- H. pylori toxins, enzymes (urease, proteases, phospholipases)
- NSAIDs
Defensive Mechanisms:
- Mucous layer - secreted by surface epithelial cells (SECs), acts as a "physiological bandage"
- Bicarbonate secretion - creates a near-neutral pH gradient at the cell surface despite an acidic lumen; lower bicarbonate secretion in proximal duodenum is demonstrated in duodenal ulcer patients
- Mucosal blood flow - delivers nutrients and oxygen; augmented during repair
- Prostaglandins (PGE2, PGI2) - key mediators of mucus/bicarbonate secretion and blood flow
- Epithelial restitution - healthy SECs migrate from the periphery to reconstitute a damaged surface layer within minutes to hours
- Pancreatic bicarbonate - neutralises acid in the duodenum via Brunner's glands and pancreatic secretion
- Duodenal acid feedback - rising duodenal acidity inhibits gastric secretion and emptying via neural and hormonal reflexes (secretin release stimulates pancreatic HCO3-)
Guyton and Hall Medical Physiology; Mulholland & Greenfield's Surgery; Current Surgical Therapy 14e
6. Classification of Gastric Ulcers (Modified Johnson Classification)
| Type | Location | Acid Secretion | Association |
|---|---|---|---|
| Type 1 (most common) | Angularis incisura, lesser curvature (antrum-body junction) | Normal or low | H. pylori, mucosal defect |
| Type 2 | Gastric body + concurrent duodenal ulcer | Increased | H. pylori, acid hypersecretion |
| Type 3 | Prepyloric (within 3 cm of pylorus) | Increased | Resembles duodenal ulcer pathophysiology |
| Type 4 | High lesser curvature, near GE junction | Normal or low | H. pylori |
| Type 5 | Anywhere, toward greater curvature | Normal | NSAID/drug-induced |
Types 2 and 3 are pathophysiologically similar to duodenal ulcers and traditionally included vagotomy in surgical management. Types 1, 4, and 5 do not require vagotomy.
Current Surgical Therapy 14e
7. Pathology (Gross and Microscopic)
Gross Features:
- Sharply punched-out, circular or oval mucosal defect
- Gastric ulcers: typically on the lesser curvature; duodenal ulcers: typically on the anterior or posterior wall of the first part
- Edges are clean-cut, perpendicular (not heaped up or overhanging - features that suggest malignancy)
- Base may show a gray-white fibrinous exudate
- Surrounding mucosa shows folds radiating toward the ulcer margin (in benign ulcers)
Microscopic Features (Robbins Pathology, 4-layer pattern):
- Superficial zone - fibrinopurulent exudate
- Necrotic zone - coagulative necrosis
- Granulation tissue layer - prominent, active
- Fibrotic scar - deepest layer extending into muscularis propria or beyond
Periulcer mucosa shows chronic active gastritis (when H. pylori is the cause), with mononuclear and neutrophilic infiltration.
Robbins & Kumar Basic Pathology
8. Clinical Features
Symptoms:
- Epigastric pain (burning, gnawing, or aching) - the cardinal symptom
- Duodenal ulcer: typically relieved by food (classically: hunger pain, food relief, recurrence 2-4 hours after meals); pain often wakes patient at night (2-4 AM)
- Gastric ulcer: pain precipitated or worsened by food; this distinction is not always reliable
- Nausea and vomiting
- Heartburn / waterbrash
- Weight changes: gastric ulcer patients are often underweight; duodenal ulcer patients may gain weight (eating relieves pain)
- Bleeding: chronic blood loss presenting as microcytic (iron-deficiency) anaemia, or acute haematemesis/melaena
Note on Symptom Overlap:
The symptoms of duodenal and gastric ulcers are often clinically indistinguishable. A significant proportion of patients with endoscopically proven peptic ulcers are asymptomatic (particularly NSAID users and elderly patients).
Clinical Examination:
- Epigastric tenderness on palpation (most common finding)
- Succession splash (in gastric outlet obstruction)
- Peritonism (in perforation)
Bailey and Love's Short Practice of Surgery, 28th Edition; Yamada's Textbook of Gastroenterology
9. Investigation
9.1 Endoscopy (Gastroduodenoscopy) - Gold Standard
- Essential to confirm diagnosis and exclude malignancy (all gastric ulcers must be biopsied - multiple biopsies from the ulcer margin and base)
- Allows CLO (Campylobacter-like organism) test for H. pylori
- Duodenal ulcers in typical location in young patients generally do not require biopsy (very low malignancy risk)
- Follow-up endoscopy at 6-8 weeks mandatory for gastric ulcers to confirm healing
9.2 Tests for H. pylori
| Test | Features |
|---|---|
| CLO (rapid urease) test | Performed on biopsy at endoscopy; quick, cheap |
| Urea breath test (UBT) | Non-invasive; excellent sensitivity and specificity; gold standard for eradication confirmation |
| H. pylori stool antigen (HpSA) | Non-invasive; useful for initial diagnosis and post-treatment confirmation |
| Serology (IgG) | Cannot distinguish active from past infection; not useful for confirming eradication |
| Histology | Biopsy-based; most sensitive; allows assessment of gastritis |
| Culture | Used for antibiotic sensitivity testing in refractory cases |
PPIs and antibiotics must be stopped 2-4 weeks before breath test or stool antigen to avoid false negatives.
9.3 Gastric Acid Analysis (Rarely Used Now)
- Useful when hypergastrinemia or Zollinger-Ellison syndrome is suspected
- Normal BAO >5 mEq/h; MAO 10-15 mEq/h
- Gastrinoma: BAO often >30 mEq/h; BAO:MAO ratio >0.6
9.4 Fasting Serum Gastrin
- Elevated in ZES, chronic atrophic gastritis, renal failure
- Provocation with IV secretin (paradoxical gastrin rise in gastrinoma)
9.5 Barium Meal (Historical)
- Largely replaced by endoscopy but may be used if endoscopy is unavailable
Bailey and Love's Short Practice of Surgery, 28th Edition; Schwartz's Principles of Surgery, 11th Edition
10. Medical Management
10.1 Lifestyle Modification
- Cessation of cigarette smoking
- Avoidance of NSAIDs, aspirin (or use of selective COX-2 inhibitors + PPI cover)
- Alcohol moderation
- These measures alone are insufficient without pharmacological treatment
10.2 Proton Pump Inhibitors (PPIs)
- Standard of care for acid suppression
- Irreversibly inhibit the H+/K+-ATPase proton pump on parietal cells
- Render patients virtually achlorhydric
- Healing rates: duodenal ulcer ~90% at 4 weeks; gastric ulcer ~80-85% at 8 weeks
- Examples: omeprazole, lansoprazole, pantoprazole, esomeprazole, rabeprazole
10.3 H2-Receptor Antagonists
- Block histamine-stimulated acid secretion via H2 receptors on parietal cells
- Reduce acid secretion by 70-80% (ranitidine, famotidine, cimetidine)
- Less effective than PPIs; largely superseded but still used
10.4 Potassium-Competitive Acid Blockers (P-CABs)
- Newer agents (e.g., vonoprazan) that competitively bind the potassium-binding region of the proton pump
- Faster onset and more prolonged acid suppression than PPIs
- Increasingly incorporated into H. pylori eradication regimens
Guyton and Hall Medical Physiology; Bailey and Love's Short Practice of Surgery
11. H. pylori Eradication
Eradication therapy is now the cornerstone of treatment for H. pylori-positive PUD. Indications for testing and treating include:
Established indications (ACG Guidelines):
- Active peptic ulcer disease (gastric or duodenal)
- Confirmed history of PUD not previously treated for H. pylori
- Gastric MALT lymphoma (low grade)
- After endoscopic resection of early gastric cancer
- Uninvestigated dyspepsia (depending on H. pylori prevalence)
Controversial indications:
- Non-ulcer (functional) dyspepsia
- GERD
- NSAID users
- Unexplained iron-deficiency anaemia
- Populations at higher risk for gastric cancer
Eradication Regimens:
Standard Triple Therapy (7-14 days):
- PPI + Clarithromycin + Amoxicillin (or Metronidazole)
- Eradication rates ~70-85% (declining due to clarithromycin resistance)
Bismuth Quadruple Therapy (10-14 days):
- PPI + Bismuth subcitrate + Tetracycline + Metronidazole
- Eradication rates >90%; preferred in areas of high clarithromycin resistance
Concomitant Therapy:
- PPI + Clarithromycin + Amoxicillin + Metronidazole simultaneously
Vonoprazan-based regimens are increasingly used especially for clarithromycin-resistant strains.
Eradication should be confirmed with UBT or HpSA ≥4 weeks after completing therapy.
Schwartz's Principles of Surgery, 11th Edition
12. Complications
12.1 Haemorrhage (Most Common Complication)
- Accounts for ~50% of upper GI bleeds historically
- Presents with: haematemesis, melaena, or iron-deficiency anaemia
- Three-quarters of bleeding peptic ulcers stop spontaneously with acid suppression and bowel rest
- One-quarter continue to bleed or rebleed - these carry nearly all mortality and morbidity
Risk stratification:
- Rockall Score (uses clinical + endoscopic criteria): score ≥3 = high risk for rebleeding/death (see table)
- Blatchford Score (no endoscopy required): score ≤1 = low risk, safe for early discharge
- High-risk endoscopic stigmata: active spurting/oozing, visible vessel (Forrest Ia/Ib/IIa), adherent clot
Management:
- Resuscitation, IV PPI (bolus + infusion)
- Early endoscopy (within 24 hours; within 12 hours for high-risk)
- Endoscopic haemostasis: injection (adrenaline), thermal coagulation (bipolar/heater probe), clips - combination therapy preferred
- Rebleeding despite endoscopic treatment: repeat endoscopy; if fails - interventional radiology (transcatheter arterial embolisation) or surgery
- Surgery: underrunning of the bleeding vessel (for duodenal ulcer) + vagotomy/pyloroplasty
Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Schwartz's Principles of Surgery, 11th Edition
12.2 Perforation (Peritonitis)
- Free perforation of anterior wall ulcers into the peritoneal cavity (especially anterior duodenal ulcers)
- Classical presentation: sudden-onset severe epigastric pain ("board-like" rigidity), peritonism, absent bowel sounds
- Erect chest X-ray: pneumoperitoneum (free gas under the diaphragm) in ~70-80% of cases
- CT abdomen: more sensitive for free gas and peritoneal fluid
- Management:
- Resuscitation (IV fluids, NG decompression, urinary catheter, IV PPI + antibiotics)
- Emergency surgery: laparoscopic or open Graham patch repair (omentoplasty) - oversewing the perforation and covering with an omental patch
- Concurrent H. pylori eradication reduces recurrence
- Definitive acid-reducing surgery (vagotomy) rarely indicated in the modern era unless truly refractory
12.3 Penetration
- Ulcer erodes through the gastric or duodenal wall into an adjacent organ without free perforation
- Posterior duodenal ulcers most commonly penetrate into the pancreas (causing back pain, elevated amylase)
- Other structures: biliary tree (cholecystitis), liver, colon (gastrocolic fistula)
- Gastrocolic fistula: severe diarrhoea after every meal, foul breath, faeculent vomiting, rapid weight loss - treated with surgical repair after nutritional optimisation
12.4 Gastric Outlet Obstruction (Pyloric Stenosis)
- Caused by oedema (acute, reversible) or fibrotic stenosis (chronic, irreversible) due to longstanding ulcer at the pylorus or first part of duodenum
- Presents with: projectile non-bilious vomiting, succession splash, early satiety, profound weight loss
- Metabolic consequence: hypochloraemic, hypokalaemic metabolic alkalosis with paradoxical aciduria
- Investigation: endoscopy (confirms diagnosis, exclude malignancy), barium meal (shows pyloric narrowing), serum electrolytes
- Management:
- Correct fluid/electrolyte imbalance (IV saline + KCl)
- NG decompression and gastric lavage
- H. pylori eradication + PPI
- Endoscopic balloon dilatation (for fibrous stenosis)
- Surgery (gastrojejunostomy or antrectomy with Billroth reconstruction) if endoscopic therapy fails
Bailey and Love's Short Practice of Surgery, 28th Edition
13. Surgical Treatment
Elective surgery for uncomplicated peptic ulceration is now rarely performed owing to the success of H. pylori eradication and PPI therapy. Surgery is reserved for complications.
13.1 Procedures for Acid Reduction:
- Truncal vagotomy - division of both vagal trunks at the oesophageal hiatus; eliminates cephalic-phase acid stimulation; requires drainage procedure (pyloroplasty or gastroenterostomy) because it causes gastric atony
- Selective vagotomy - division of only the gastric branches of the vagus; less morbidity than truncal; also requires drainage
- Highly selective (proximal gastric) vagotomy - denervates only the acid-secreting fundus/corpus, preserving antral/pyloric innervation; no drainage needed; lowest complication rate
- Antrectomy - removes the gastrin-secreting antrum; combined with vagotomy for best results (Billroth I or II reconstruction)
- Pyloroplasty (Heineke-Mikulicz) - full-thickness longitudinal incision through the pylorus closed transversely, used as a drainage procedure accompanying vagotomy
13.2 Post-Surgical Complications ("Post-gastrectomy Syndromes"):
- Dumping syndrome (early/late)
- Diarrhoea (postvagotomy)
- Small stomach syndrome / early satiety
- Recurrent (stomal) ulceration
- Gastrocolic fistula
- Afferent loop syndrome
- Alkaline reflux gastritis
Bailey and Love's Short Practice of Surgery, 28th Edition; Current Surgical Therapy 14e
14. Special Situations
Peptic Ulcer in Pregnancy
- Pregnancy generally has a protective effect on PUD - elevated progesterone reduces acid secretion and motility; higher prostaglandin levels protect the mucosa
- Symptoms often improve during pregnancy and relapse post-partum
- Treatment: antacids, sucralfate (preferred, not absorbed); PPIs if necessary (omeprazole, generally considered safe in 2nd/3rd trimester); H. pylori eradication deferred until after delivery (antibiotics restricted)
Creasy & Resnik's Maternal-Fetal Medicine
Stress Ulcers (Curling's and Cushing's Ulcers)
- Curling's ulcer: stress ulcers associated with severe burns (reduced plasma volume and mucosal ischaemia)
- Cushing's ulcer: stress ulcers associated with head injury or intracranial hypertension (vagally mediated acid hypersecretion)
- Both may perforate and bleed; prophylaxis with PPI or H2 blockers is standard in ICU patients
15. Summary
| Feature | Duodenal Ulcer | Gastric Ulcer |
|---|---|---|
| Frequency | More common | Less common |
| Acid secretion | Usually increased | Normal or reduced |
| H. pylori | ~90-95% association | ~70-80% association |
| Pain | Relieved by food | Worsened by food |
| Weight | Often maintained/increased | Often lost |
| Malignancy risk | Very rare | Must exclude (biopsy all) |
| Recurrence without H. pylori eradication | ~80% at 1 year | ~60% at 1 year |
| Typical surgical lesion | Vagotomy + drainage | Resection (Billroth I or II) |
Key References
- Bailey and Love's Short Practice of Surgery, 28th Edition (Chapter 67 - Peptic Ulceration)
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease (Chapter 20 - UGI Bleeding / Peptic Ulcer)
- Robbins & Kumar Basic Pathology (Chapter 13 - Gastrointestinal Tract)
- Guyton and Hall Textbook of Medical Physiology (Chapter 67 - Peptic Ulcer)
- Schwartz's Principles of Surgery, 11th Edition (Chapter 26 - Stomach and Duodenum)
- Mulholland and Greenfield's Surgery, 7th Edition (Chapter 45 - Peptic Ulcer Disease)
- Current Surgical Therapy, 14th Edition (Benign Gastric Ulcer; Perforated Peptic Ulcer sections)
- Creasy & Resnik's Maternal-Fetal Medicine (Peptic Ulcer Disease in Pregnancy)
Recent Evidence Note (2025-2026): A 2026 systematic review in Gastroenterology (PMID 41236450) quantified the substantial disease burden of H. pylori beyond gastric cancer, including peptic ulcer morbidity and mortality, arguing for wider mass eradication strategies. A 2025 meta-analysis (PMID 40281437) documented the prevalence and patterns of PUD in Africa, highlighting the continued high H. pylori contribution in lower-income regions. These findings reinforce the continued centrality of H. pylori eradication in global PUD management.
This is a shared conversation. Sign in to Orris to start your own chat.