Acute pancreatitis
Reading File
Finding Sources
Searching PubMed
"acute pancreatitis"[MeSH Terms] AND management
Reading File
Reading File
Searching PubMed
"acute pancreatitis"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I now have all the information needed for a comprehensive, well-illustrated response. Let me compile it.
Acute Pancreatitis
Acute pancreatitis (AP) is a sudden inflammatory condition of the pancreas caused by enzymatic autodigestion of pancreatic tissue. It is the most common pancreatic disease worldwide and a leading cause of gastrointestinal hospitalization in the United States. Severity ranges from mild and self-limited to life-threatening necrotizing disease with multiorgan failure - overall mortality can reach 30% in severe cases, though the trend is improving.
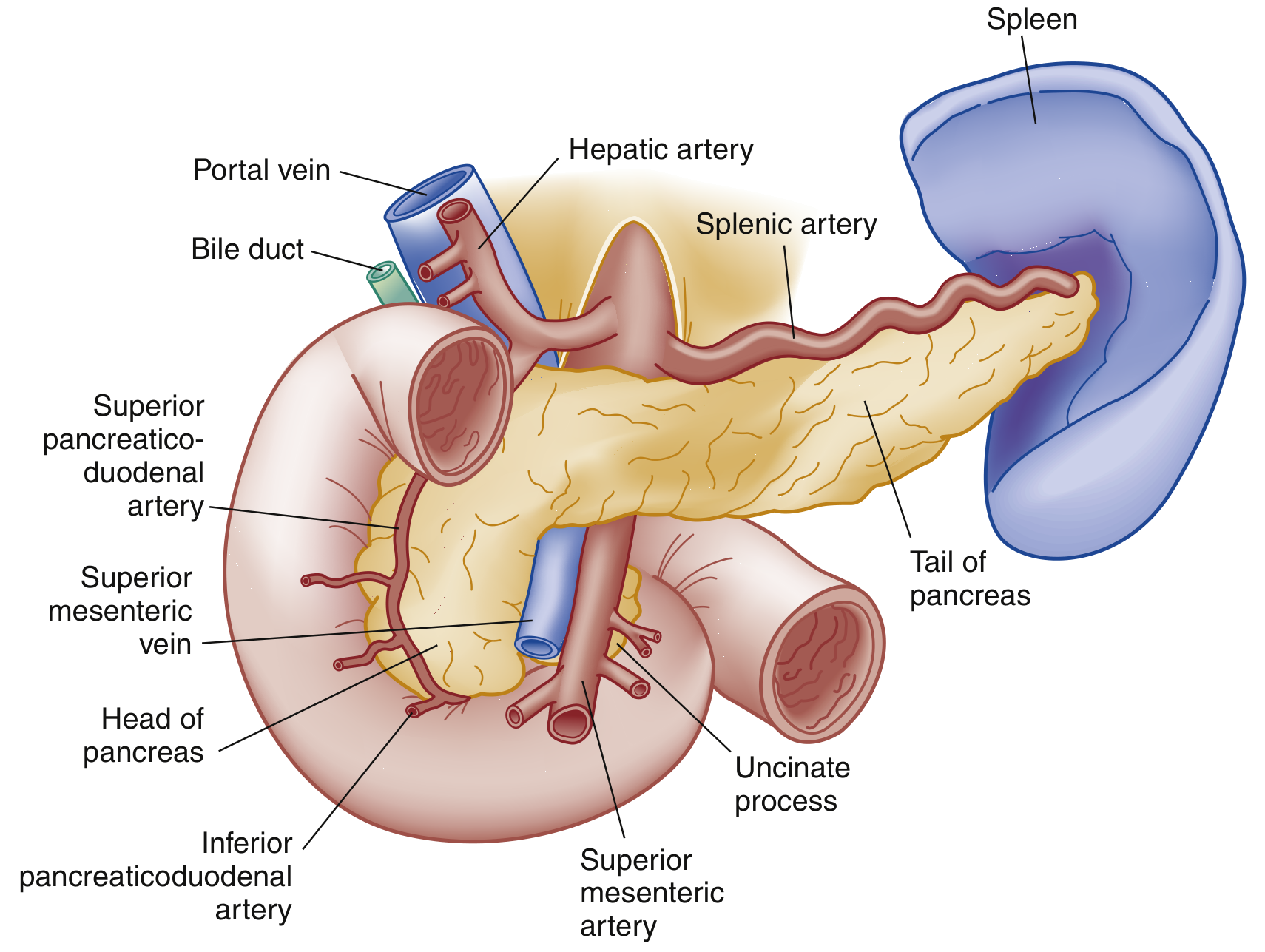
Pancreatic anatomy (anterior view):
Etiology
The two dominant causes account for the vast majority of cases:
- Gallstones: 40-70% of cases (most common cause overall)
- Alcohol: 25-35% of cases
Other important causes include:
| Category | Examples |
|---|---|
| Toxic-Metabolic | Hypertriglyceridemia (>1000 mg/dL), hypercalcemia, uremia, scorpion venom, drugs |
| Mechanical-Obstructive | Post-ERCP (5-10%), ampullary stenosis, pancreas divisum, annular pancreas, tumor |
| Infectious | Viral (mumps, coxsackievirus, HIV, CMV, EBV, varicella); bacterial (TB, Mycoplasma); parasitic (Ascaris) |
| Vascular | Vasculitis, embolism, hypoperfusion, hypercoagulability |
| Other | Idiopathic, hereditary, autoimmune, DKA |
Note: Many "idiopathic" cases are thought to be caused by occult microlithiasis. Smoking and diabetes are independent risk factors.
In children, the distribution differs: trauma, systemic disease, medications (valproate, L-asparaginase, steroids, 6-mercaptopurine), and biliary disease are more prominent causes, with a genetic component (SPINK1, CFTR mutations) in recurrent cases.
Pathophysiology
Regardless of the trigger, AP begins with inappropriate intracellular activation of digestive enzymes - particularly trypsinogen converting to trypsin - within acinar cells. This leads to:
- Autodigestion of pancreatic parenchyma
- Local inflammatory response and microvascular damage
- Release of inflammatory mediators (cytokines, phospholipase A2, elastase)
- Progression to systemic inflammatory response syndrome (SIRS)
- In severe disease: multiorgan failure, pancreatic necrosis, and sepsis
Classification (Revised Atlanta 2012)
By morphological type:
- Interstitial edematous pancreatitis: The majority (~90-95%). Pancreatic edema with preserved perfusion. Usually resolves within the first week.
- Necrotizing pancreatitis: ~5-10% of cases. Involves ischemic necrosis of pancreatic parenchyma and/or surrounding peripancreatic tissue. Necrosis may remain sterile or become infected; infected necrosis carries significantly higher morbidity.
By severity:
- Mild: No organ failure, no local or systemic complications
- Moderately severe: Transient organ failure (<48 hours) and/or local complications
- Severe: Persistent organ failure (>48 hours), single or multiorgan
Local complications (by fluid collection type):
| Type | Timing | Features |
|---|---|---|
| Acute peripancreatic fluid collection | <4 weeks | Homogeneous fluid adjacent to pancreas (interstitial) |
| Pancreatic pseudocyst | >4 weeks | Homogeneous with well-defined wall (interstitial) |
| Acute necrotic collection | <4 weeks | Heterogeneous fluid + necrosis (necrotizing) |
| Walled-off necrosis | >4 weeks | Heterogeneous with well-defined wall (necrotizing) |
Clinical Features
Symptoms:
- Persistent, moderate-to-severe epigastric or left upper quadrant pain
- Radiation to the back, chest, or flanks (classic "boring" quality)
- Pain may be relieved by leaning forward
- Nausea, vomiting, and anorexia
- Pain is exacerbated by oral intake
Signs:
- Tachycardia, fever (inflammatory response)
- Hypotension/shock in severe disease (fluid shifts, volume loss)
- Epigastric tenderness ± guarding
- Diminished or absent bowel sounds (paralytic ileus)
- Jaundice suggests biliary/obstructive etiology
- Cullen sign: Periumbilical bluish discoloration (hemoperitoneum) - rare, poor prognosis
- Grey Turner sign: Reddish-brown flank discoloration (retroperitoneal hemorrhage) - rare, poor prognosis
- Basilar crackles or decreased breath sounds (pulmonary complications)
- Right upper quadrant tenderness + Murphy sign in gallstone pancreatitis
Systemic complications:
- Pulmonary: pleural effusions (up to 50%, predominantly left-sided), ARDS, atelectasis
- Cardiovascular: shock from fluid shifts and third-spacing
- Renal failure: hypoperfusion + inflammatory mediators
- Coagulopathy/DIC: cytokine-mediated coagulation cascade activation
- Metabolic: hyperglycemia (decreased insulin), hypocalcemia (low albumin + magnesium)
Diagnosis
AP is diagnosed when at least 2 of 3 criteria are met:
- Abdominal pain characteristic of AP
- Serum lipase or amylase ≥3x upper limit of normal
- Characteristic findings on imaging
Laboratory tests:
| Test | Notes |
|---|---|
| Lipase | Preferred - more sensitive and specific than amylase. Peaks earlier, stays elevated ~1-2 weeks. Use this preferentially. |
| Amylase | Less specific (elevated in salivary disease, renal failure, appendicitis, cholecystitis, bowel obstruction). Stays elevated ~3-5 days. May be falsely normal in alcohol/hypertriglyceridemia-induced AP. |
| ALT | PPV ~95% for biliary pancreatitis when elevated |
| Bilirubin, AST | Evaluate for obstructive cause |
| Triglycerides | Check if no gallstones or alcohol history |
| Calcium | Elevated may be causative; low indicates severity |
| CBC, BMP | Evaluate SIRS, organ failure |
Testing both lipase AND amylase does not improve diagnostic accuracy. Enzyme levels do NOT correlate with severity.
Imaging
Abdominal Ultrasound - should be performed in all patients:
- Limited direct pancreatic visualization (bowel gas obstruction)
- First-line to evaluate for biliary etiology (gallstones, ductal dilation)
- Normal ultrasound does NOT exclude AP
Contrast-Enhanced CT (CECT) - gold standard for severity assessment:
-
90% sensitivity and specificity
- Indicated when diagnosis is uncertain, or to assess severity/complications
- Best done 48-72 hours after onset (early CT may underestimate necrosis)
- Normal CT in 15-30% of mild cases
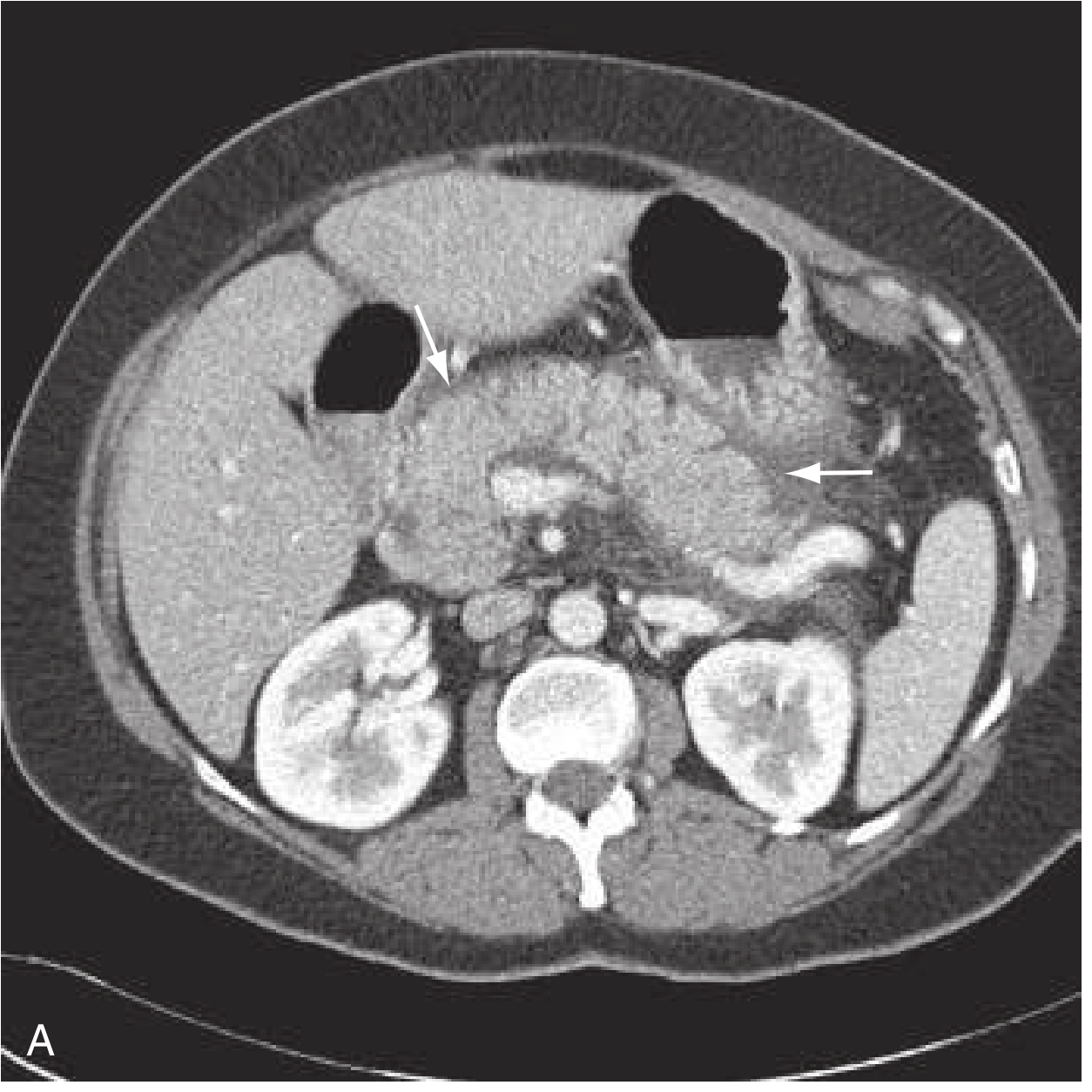
CT findings of interstitial edematous pancreatitis (peripancreatic fat stranding, mild fluid):
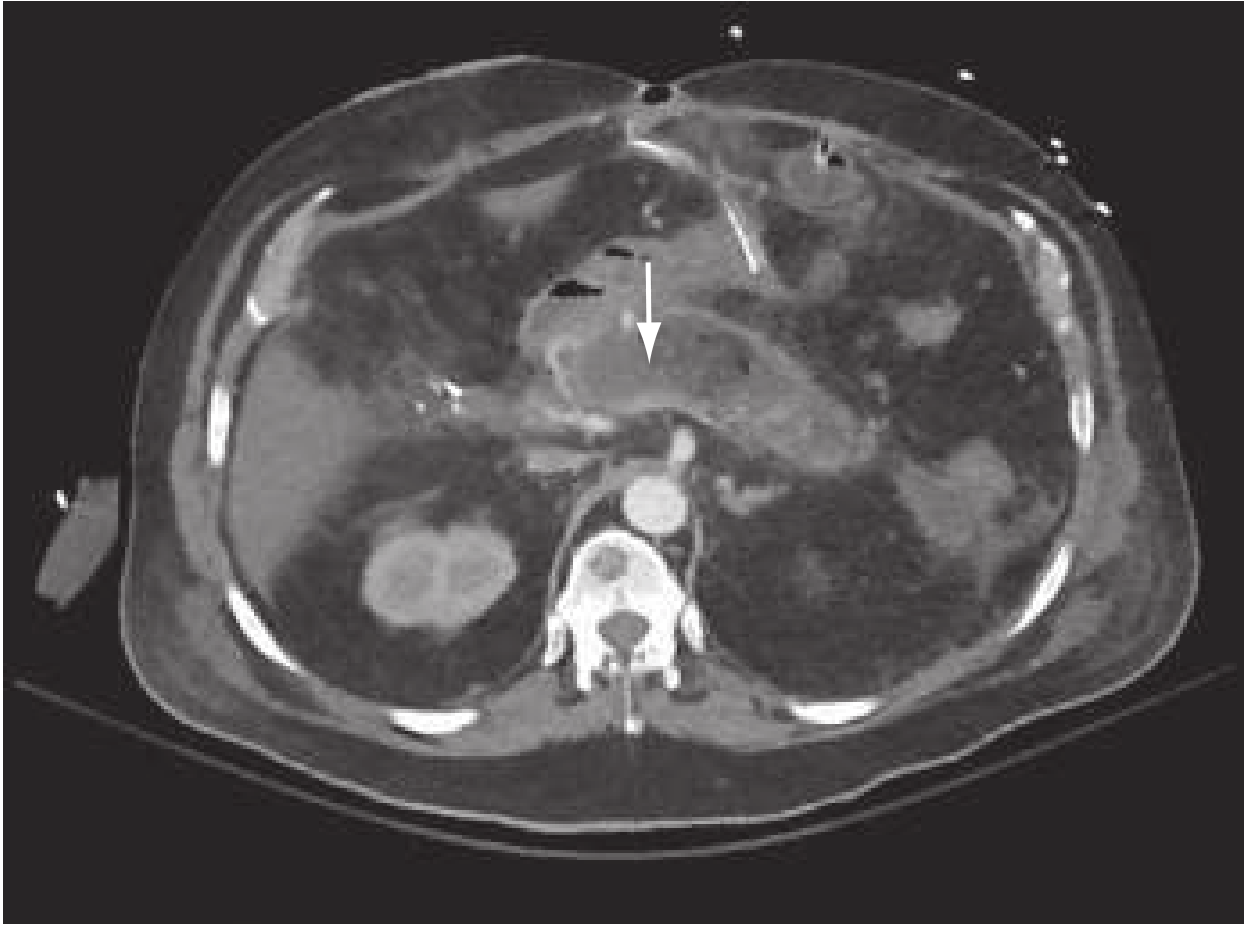
CT findings of necrotizing pancreatitis (area of non-enhancement, arrow):
MRI/MRCP: Superior for biliary tract imaging, equal diagnostic value to CT; preferred when contrast is contraindicated or for duct evaluation. MRCP has largely replaced diagnostic ERCP.
CT Severity Index (CTSI / Balthazar score): Grades from A-E based on pancreatic inflammation + degree of necrosis. Scores ≥7 carry ~17% mortality and 92% morbidity.
Severity Scoring Systems
Several scoring systems predict disease severity, though no single system is ideal for ED use:
| Score | Parameters | Notes |
|---|---|---|
| BISAP (Bedside Index for Severity in AP) | BUN >25, impaired mental status, SIRS, age >60, pleural effusion | Simpler, ED-friendly; score ≥3 predicts severe AP |
| Ranson criteria | 11 parameters over 48 hours | Classic but requires 48-hr assessment |
| APACHE II | Multiple physiologic variables | Validated, used in ICU |
| Revised Atlanta | Clinical + radiologic | Current standard classification |
Management
Initial resuscitation
- IV fluid resuscitation is the cornerstone of initial therapy
- Lactated Ringer's solution preferred over normal saline (NS associated with hyperchloremic acidosis and worse outcomes in some studies)
- Goal-directed: 250-500 mL/hr initially; reassess at 6 hours
- Avoid aggressive over-resuscitation (worsens pulmonary complications)
- Continuous monitoring: urine output, BUN, hematocrit, vital signs
Pain management
- Aggressive analgesia required - IV opioids (morphine, hydromorphone, fentanyl) are acceptable and do not worsen outcomes
- NSAIDs/ketorolac useful adjuncts
- Avoid withholding analgesia out of concern for masking symptoms
Nutrition
- Mild AP: Oral feeding as tolerated - initiate early (within 24-48 hours when pain improves and tolerated)
- Severe AP: Enteral feeding preferred over parenteral (maintains gut barrier, reduces infectious complications)
- Nasojejunal or nasogastric tube feeding if oral route not possible
- Total parenteral nutrition (TPN) is a last resort
- NPO is no longer recommended as standard practice for mild AP; early refeeding improves outcomes
Antibiotics
- NOT indicated prophylactically in sterile necrosis
- Indicated only for proven or strongly suspected infected pancreatic necrosis or concurrent infection (cholangitis, etc.)
- Agents: carbapenems, fluoroquinolones, or metronidazole combinations (good pancreatic penetration)
Biliary pancreatitis - specific interventions
- ERCP with sphincterotomy: Indicated within 24-48 hours if concurrent acute cholangitis or biliary obstruction (NOT for uncomplicated gallstone pancreatitis)
- Cholecystectomy: Should be performed during the same admission in mild biliary AP (reduces recurrence risk); can be deferred in severe AP
Necrotizing pancreatitis
- Sterile necrosis: Conservative management; antibiotics NOT indicated
- Infected necrosis (suspected when clinical deterioration after day 7-10, fever, leukocytosis):
- CT-guided fine needle aspiration (FNA) for culture (though diagnosis increasingly made clinically)
- Step-up approach is now standard:
- Percutaneous or endoscopic drainage first
- Video-assisted retroperitoneal debridement (VARD) or endoscopic necrosectomy if drainage fails
- Open surgical necrosectomy (last resort - high mortality)
- Surgery delayed at least 4 weeks to allow "walled-off necrosis" to mature
ICU care
Patients with severe AP (persistent organ failure) require ICU-level monitoring for:
- Respiratory: supplemental O2, may need mechanical ventilation for ARDS
- Cardiovascular: vasopressors for shock refractory to fluids
- Renal: renal replacement therapy for AKI
Differential Diagnosis
- Peptic ulcer disease / perforated viscus
- Cholecystitis, cholangitis, choledocholithiasis
- Mesenteric ischemia
- Bowel obstruction
- Myocardial infarction (especially inferior MI)
- Aortic dissection / AAA
- Pericarditis
- Diabetic ketoacidosis
- Sickle cell crisis
Prognosis & Complications
- Majority (~80%) have mild disease and recover within 1-2 weeks
- ~20% develop severe AP; mortality ~30% in this group
- Overall mortality has decreased despite rising hospitalization rates
Late complications:
- Pancreatic pseudocyst (most common fluid complication)
- Walled-off necrosis
- Splenic or portal vein thrombosis
- Gastrointestinal bleeding
- Gastric outlet obstruction
- Exocrine insufficiency and endocrine insufficiency (diabetes) - especially after recurrent or necrotizing disease
- Recurrent AP can progress to chronic pancreatitis (fibrosis, ductal changes, exocrine/endocrine failure)
Sources: Rosen's Emergency Medicine, 9e (Ch. 77); Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Grainger & Allison's Diagnostic Radiology, 6e (Ch. 25)
This is a shared conversation. Sign in to Orris to start your own chat.