parathyroid gland in detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the complete detailed answer.
The Parathyroid Glands - A Detailed Overview
1. Historical Background
The parathyroid glands were first accurately described in 1849 by Sir Richard Owen after autopsy of an Indian rhinoceros. Human parathyroids were not described until 1879 by Swedish medical student Ivar Sandström, who coined the term glandulae parathyroideae. The link between these glands and bone disease (osteitis fibrosa cystica) was recognized in 1903. The first successful parathyroidectomy was performed in 1925 by Felix Mandl on a patient with severe bone pain. - Schwartz's Principles of Surgery, p. 1663
2. Embryology
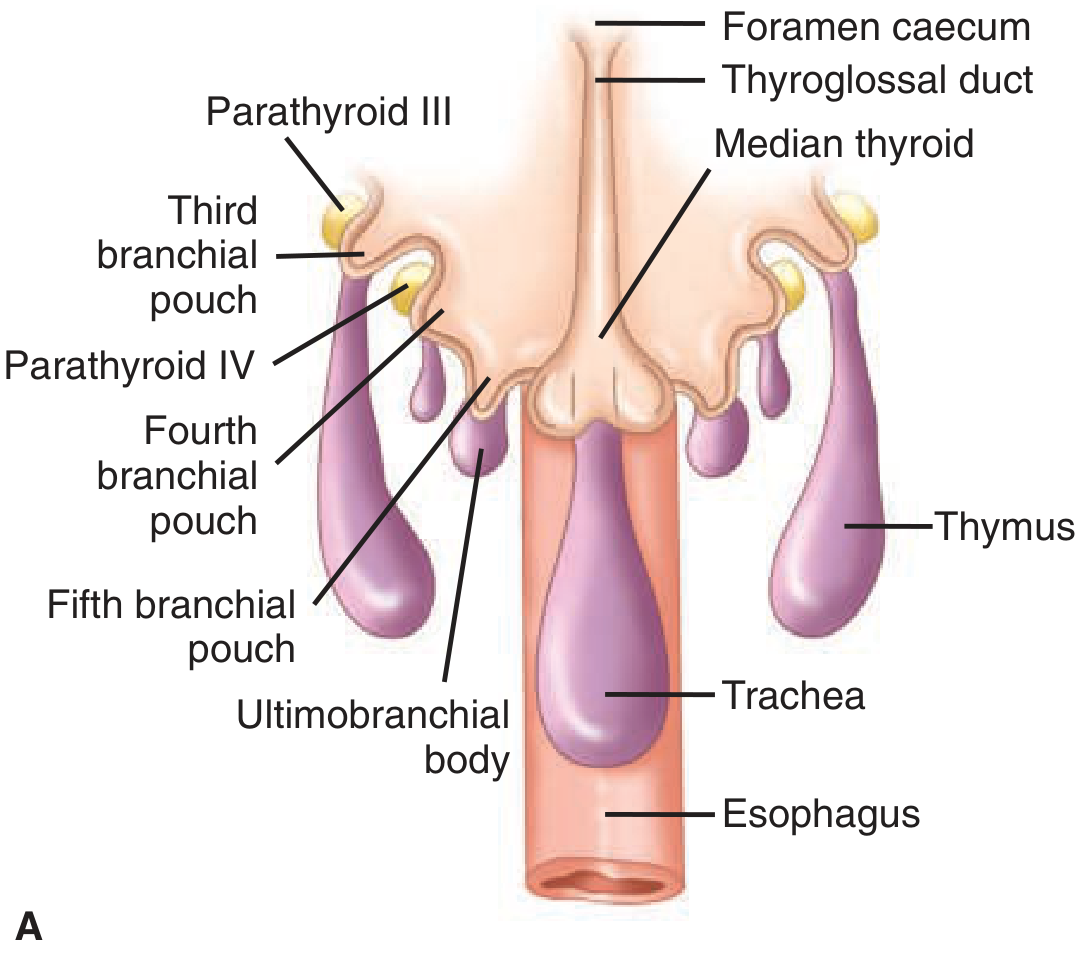
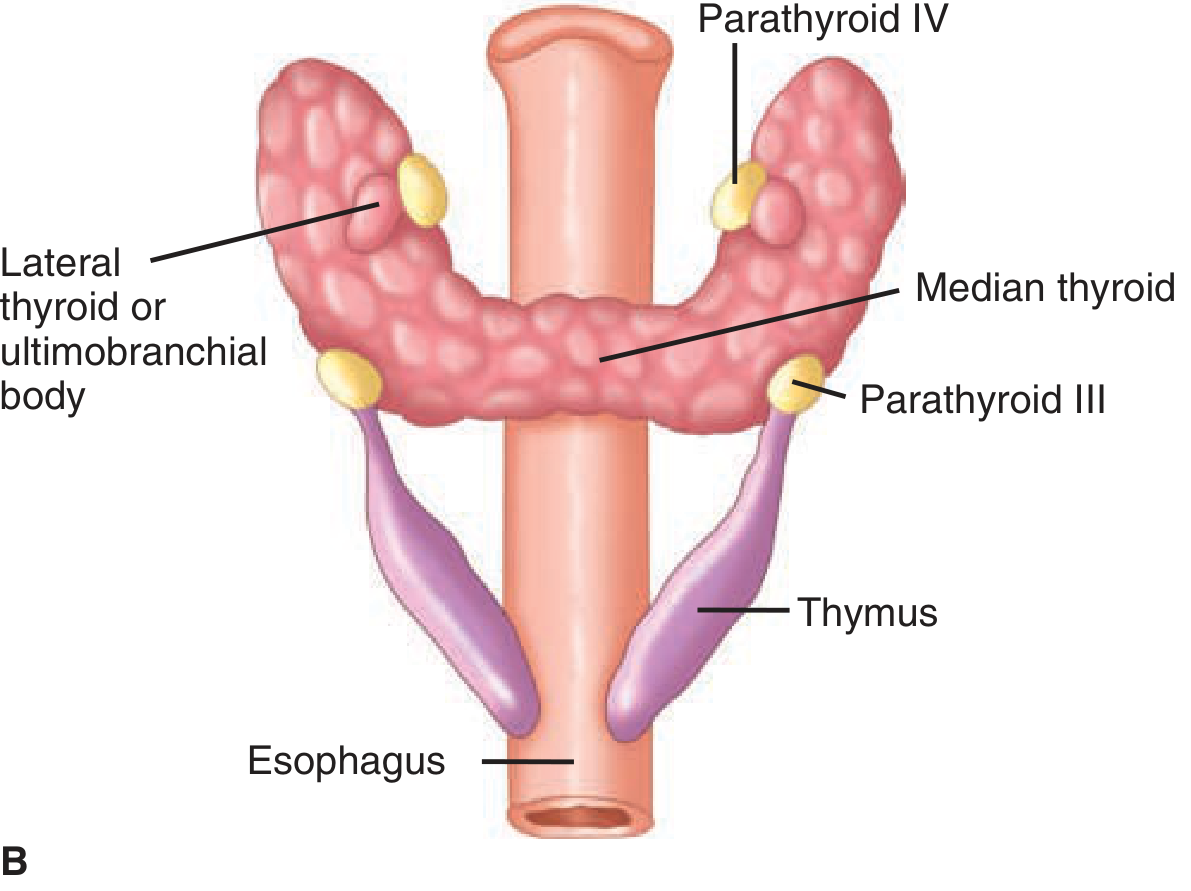
Figure 38-25: Parathyroid embryology. (A) Pharynx of an 8-10mm embryo. (B) Final positions in a 13-14mm embryo. - Schwartz's Principles of Surgery
- Superior parathyroids (Parathyroid IV) arise from the 4th pharyngeal pouch (which also gives rise to the thyroid). Their position is more consistent - 80% found near the posterior surface of the upper thyroid lobes.
- Inferior parathyroids (Parathyroid III) arise from the 3rd pharyngeal pouch (which also gives rise to the thymus). They descend with the thymus and then separate, ending up below the superior glands.
- Failure to separate from the thymus leads to ectopic glands found within the mediastinum or thymic tissue (2-10% of individuals).
- Chief cells differentiate during embryonic development and are functional in fetal calcium regulation. Oxyphil cells differentiate later at puberty. - Histology: A Text and Atlas, p. 2025
3. Gross Anatomy
- There are 4 parathyroid glands in most people (supernumerary glands may exist).
- Each gland is ovoid, measuring a few millimeters in diameter; combined weight < 500 mg.
- Located on the posterior surface of the lateral lobes of the thyroid gland, embedded in connective tissue.
- Blood supply: Inferior thyroid arteries, or anastomoses between superior and inferior thyroid arteries.
- Superior glands are more consistently positioned; inferior glands are more variable in location due to their longer embryological migration.
- Ectopic locations include: intrathyroidal, retro-esophageal, mediastinal, within the thymus, and within the carotid sheath. - Schwartz's Principles of Surgery, p. 1664
4. Histology and Microanatomy
Each gland is enclosed by a thin connective tissue capsule from which septa extend inward to divide it into poorly defined lobules. The connective tissue (including fat cells) becomes more prominent with age, ultimately comprising 60-70% of glandular mass in adults.
Typical of endocrine glands, the parenchyma is surrounded by rich networks of fenestrated capillaries and lymphatics.
Cell Types
1. Principal (Chief) Cells - the dominant functional cell
- Most numerous parenchymal cell type
- Small, polygonal; diameter 7-10 μm; centrally located nucleus
- Pale-staining, slightly acidophilic cytoplasm
- Cytoplasm contains: lipofuscin vesicles, glycogen accumulations, lipid droplets
- Dense membrane-limited vesicles = storage form of PTH
- Responsible for synthesis, storage, and secretion of PTH
2. Oxyphil Cells
- Larger than chief cells
- Characterized by abundant acidophilic (eosinophilic) cytoplasm packed with mitochondria
- Appear at puberty; increase in number with age
- Function is not fully established; thought to be modified/aged chief cells
- May represent hypofunctional cells
3. Fat cells (adipocytes)
- Increase with age; make up the majority of adult glandular mass
- Histology: A Text and Atlas, pp. 2024-2025
5. Physiology - Parathyroid Hormone (PTH)
Structure and Synthesis
- PTH is an 84-amino-acid single-chain peptide hormone
- Initially synthesized as pre-pro-PTH (115 amino acids) on ribosomes of the rough ER
- The 25-amino-acid signal ("pre") sequence is cleaved upon entry into the ER lumen
- Pro-PTH (90 aa) is then cleaved to the mature 84-aa PTH
- The biologically active fragment is the N-terminal 1-34 portion
- Katzung's Basic and Clinical Pharmacology; Medical Physiology (Boron)
Regulation of Secretion
The primary regulator is ionized plasma Ca²⁺ - detected by calcium-sensing receptors (CaSR) on chief cell surfaces:
| Stimulus | Effect on PTH |
|---|---|
| Low plasma Ca²⁺ | Stimulates PTH release |
| High plasma Ca²⁺ | Inhibits PTH release |
| 1,25-Dihydroxyvitamin D | Inhibits PTH gene transcription |
| Hyperphosphatemia | Stimulates PTH release |
| Hypomagnesemia (severe) | Impairs PTH secretion |
- The PTH gene has upstream response elements for vitamins D and A. When occupied by 1,25-dihydroxyvitamin D, the Vitamin D Receptor (VDR)-RXR heterodimer binds and decreases PTH transcription.
- Medical Physiology (Boron & Boulpaep), p. 1552
Actions of PTH
PTH acts through PTH/PTHrP receptors (PTHR1) coupled to G-protein signaling (cAMP/PKA and IP3/Ca²⁺ pathways):
On Bone:
- Increases bone resorption by activating osteoclasts (indirectly - via RANKL expression on osteoblasts)
- Liberates Ca²⁺ and phosphate from hydroxyapatite crystals
- Intermittent low-dose PTH paradoxically stimulates bone formation (basis of teriparatide therapy for osteoporosis)
On the Kidney (3 major actions):
- Stimulates Ca²⁺ reabsorption in the distal convoluted tubule → raises plasma Ca²⁺
- Inhibits phosphate reabsorption in the proximal tubule (phosphaturia) - redistributes NaPi-IIa and NaPi-IIc cotransporters away from the apical membrane
- This prevents precipitation of calcium-phosphate salts when Ca²⁺ is mobilized from bone
- Stimulates 1α-hydroxylase in the proximal tubule → converts 25-OH vitamin D to 1,25-dihydroxyvitamin D (calcitriol), the active form
Via Vitamin D (indirect intestinal action):
- PTH-stimulated calcitriol → enhances intestinal Ca²⁺ and phosphate absorption in the small intestine
- Medical Physiology (Boron), pp. 1552-1553; Schwartz's Principles of Surgery, p. 1664
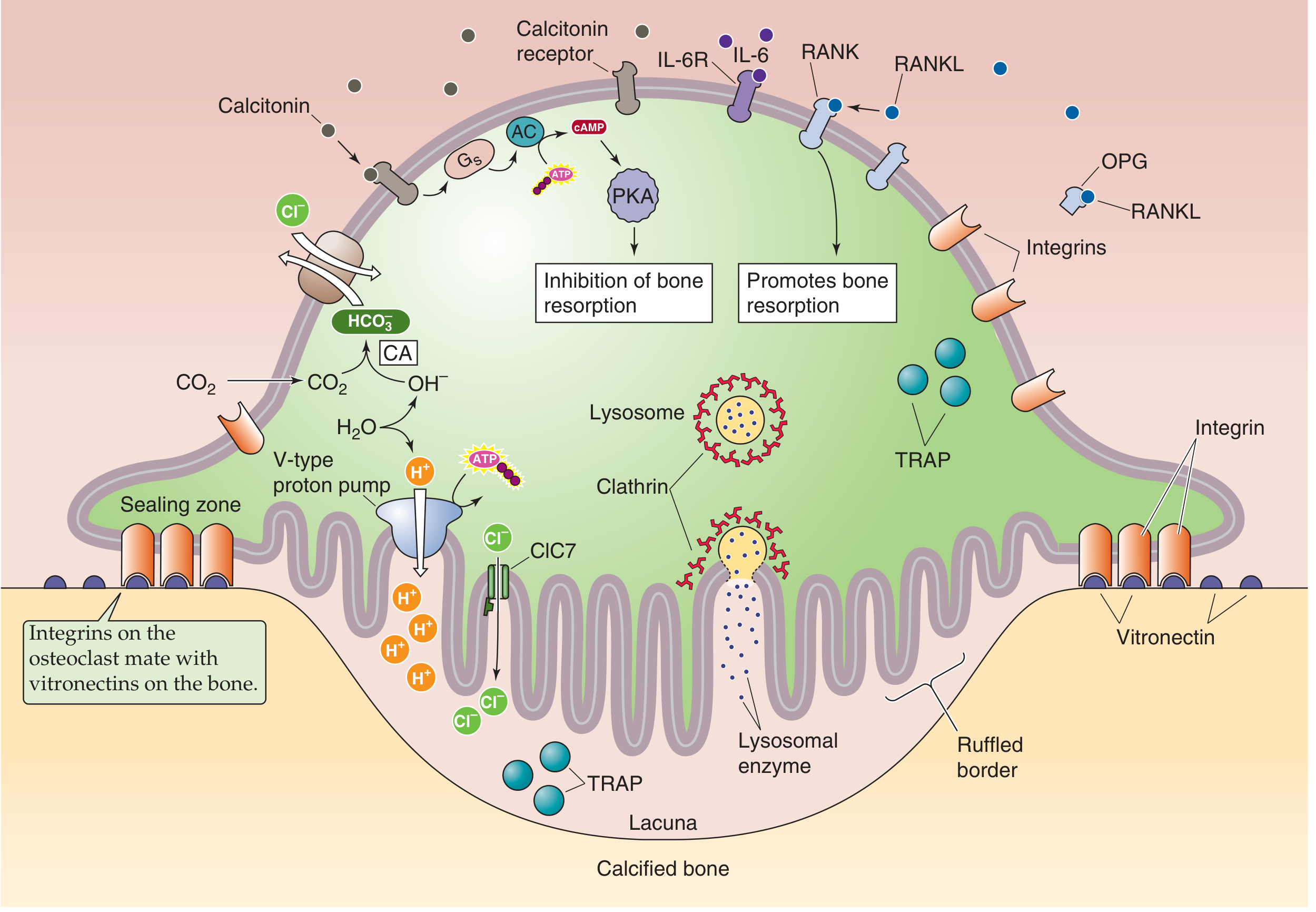
Figure: Osteoclast mechanism of bone resorption - calcitonin inhibits via cAMP/PKA while RANKL promotes resorption via acidification of the lacuna. - Medical Physiology (Boron)
PTH vs. Calcitonin (Opposing Hormone)
- PTH raises blood calcium slowly (peak effect over several hours) - long-term homeostatic action
- Calcitonin (from thyroid C-cells) rapidly lowers blood calcium (peak ~1 hour) - rapid acute action
- Histology: A Text and Atlas, p. 2029
6. Calcium Homeostasis Summary
| Parameter | PTH Effect |
|---|---|
| Serum Ca²⁺ | ↑ (raises) |
| Serum Phosphate | ↓ (lowers via phosphaturia) |
| Urine Ca²⁺ | ↓ (promotes reabsorption) |
| Urine Phosphate | ↑ (phosphaturia) |
| 1,25-(OH)₂ Vitamin D | ↑ (stimulates production) |
| Intestinal Ca²⁺ absorption | ↑ (indirect, via vitamin D) |
7. Disorders of the Parathyroid Gland
A. Hyperparathyroidism (HPT)
Primary HPT (PHPT)
- Most common cause: solitary parathyroid adenoma (~85%)
- Other causes: multiglandular hyperplasia (~15%), parathyroid carcinoma (<1%)
- Associated with: MEN1 (mutation of menin gene), MEN2A, and familial isolated HPT
- Mutations: Inactivation of RB1 gene and the HRPT2/CDC73 gene (encodes parafibromin) seen in carcinoma
- Modern presentation is often asymptomatic, discovered incidentally on routine blood work (hypercalcemia)
Classic pentad: "Bones, Stones, Abdominal Groans, Psychic Moans, and Fatigue Overtones"
Complications:
- Renal: Nephrolithiasis (calcium phosphate/oxalate stones, ~20-25% of patients), nephrocalcinosis, polyuria/polydipsia, hypertension
- Bone: Osteitis fibrosa cystica (subperiosteal resorption on radial aspect of 2nd/3rd finger phalanges, brown tumors, bone cysts), osteoporosis predominantly at cortical sites (distal radius)
- GI: Constipation, nausea, peptic ulcers, pancreatitis
- Neuropsychiatric: Depression, memory loss, fatigue, weakness
Secondary HPT
- PTH secretion is increased in response to chronic hypocalcemia (most commonly chronic kidney disease)
- Parathyroid glands undergo diffuse hyperplasia
- Also occurs in vitamin D deficiency and malabsorption
Tertiary HPT
- Autonomous PTH secretion that persists after correction of the underlying cause (e.g., after renal transplantation)
B. Hypoparathyroidism
Causes:
- Most common: inadvertent removal or devascularization during thyroidectomy or parathyroid surgery
- Autoimmune (autoimmune polyendocrinopathy)
- DiGeorge syndrome (22q11 deletion - failure of 3rd and 4th pharyngeal pouch development)
- Hypomagnesemia (impairs PTH secretion)
- Infiltrative diseases (hemochromatosis, Wilson's disease)
Clinical features of hypocalcemia:
- Paresthesias (lips, hands, feet)
- Tetany - spontaneous muscle spasms
- Chvostek's sign - facial muscle twitch on tapping over facial nerve
- Trousseau's sign - carpal spasm with blood pressure cuff inflation
- Laryngospasm, seizures
- Prolonged QT interval on ECG
- Chronic: cataracts, basal ganglia calcification, dental enamel defects
Treatment: Oral calcium supplementation + calcitriol (active vitamin D)
C. Pseudohypoparathyroidism
- Kidneys do not respond to intact PTH (PTH resistance)
- PTH levels are elevated but hypocalcemia persists
- Associated with Albright hereditary osteodystrophy (short stature, brachydactyly)
8. Clinical Testing
| Test | Interpretation |
|---|---|
| Serum intact PTH (iPTH) | Direct measure of PTH secretion |
| Serum Ca²⁺ (ionized) | Primary regulated parameter |
| 24-hour urine Ca²⁺ | Differentiates PHPT from FHH (familial hypocalciuric hypercalcemia) |
| Serum phosphate | Low in PHPT (phosphaturia) |
| 25-OH Vitamin D | Assess vitamin D stores |
| 1,25-(OH)₂ Vitamin D | Elevated in PHPT |
| Alkaline phosphatase | Elevated with increased bone turnover |
Familial Hypocalciuric Hypercalcemia (FHH): Caused by inactivating mutations of the CaSR gene. Patients have elevated plasma Ca²⁺ but low urinary Ca²⁺ excretion - this distinguishes it from PHPT where urine Ca²⁺ is elevated. - Medical Physiology (Boron), Box 52-1
9. Parathyroid Surgery
Indications for parathyroidectomy in PHPT:
- Symptomatic disease
- Serum Ca²⁺ > 1 mg/dL above upper limit of normal
- Age < 50 years
- Reduced BMD (T-score < -2.5 at any site), fragility fracture
- Creatinine clearance < 60 mL/min, nephrolithiasis, nephrocalcinosis
- 24-hour urinary Ca²⁺ > 400 mg/day
Outcomes: Success rate > 95%. Parathyroidectomy results in:
- 6-8% BMD improvement in first year, up to 12-15% at 15 years
- 50% fracture risk reduction at hip and upper arm
- Resolution of most systemic symptoms
- Schwartz's Principles of Surgery, p. 1698
Medical management: Bisphosphonates (bone protection), calcimimetics (cinacalcet - activates CaSR, reduces Ca²⁺ and PTH levels) for patients who refuse or are unfit for surgery.
Summary Table
| Feature | Detail |
|---|---|
| Number | 4 (occasionally supernumerary) |
| Weight | < 500 mg combined |
| Location | Posterior surface of thyroid lobes |
| Superior origin | 4th pharyngeal pouch |
| Inferior origin | 3rd pharyngeal pouch |
| Cell types | Chief (principal) cells, oxyphil cells |
| Hormone | PTH - 84 amino acid peptide |
| Primary regulator | Ionized Ca²⁺ (via CaSR) |
| Net effect | Raises serum Ca²⁺; lowers serum PO₄³⁻ |
| Key disorder | Hyperparathyroidism (usually adenoma) |
Sources: Histology: A Text and Atlas (Pawlina); Schwartz's Principles of Surgery, 11e; Medical Physiology (Boron & Boulpaep); Katzung's Basic and Clinical Pharmacology, 16e; Guyton and Hall Textbook of Medical Physiology
This is a shared conversation. Sign in to Orris to start your own chat.