Brown sequared syndrome
"Brown-Sequard syndrome"[MeSH Terms]
Brown-Séquard Syndrome
Definition
- Bradley and Daroff's Neurology in Clinical Practice, p. 1306
- Goldman-Cecil Medicine, p. 3847
Anatomy Underlying the Syndrome
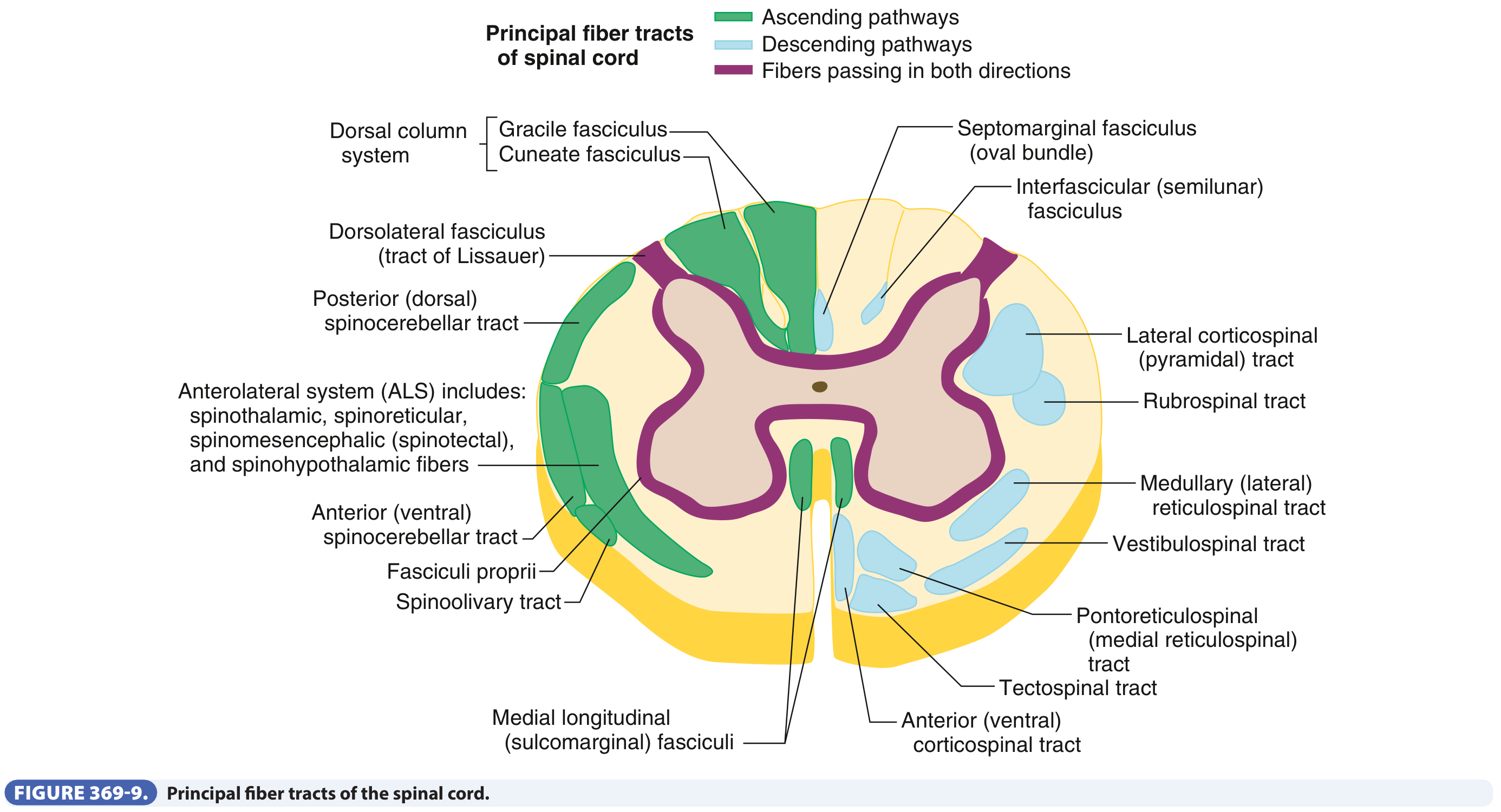
| Tract | Side of cord | Crosses where? |
|---|---|---|
| Lateral corticospinal tract (motor) | Ipsilateral to muscle | Already crossed in medullary pyramids |
| Dorsal columns (proprioception, vibration, 2-point) | Ipsilateral to receptor | Crosses in medulla |
| Spinothalamic tract (pain, temperature) | Contralateral to receptor | Crosses in the anterior white commissure within 1-2 spinal segments of entry |
Classic Clinical Features
1. At the Level of the Lesion (Segmental)
- Ipsilateral lower motor neuron (LMN) signs: paresis, atrophy, fasciculations, areflexia - due to damage to anterior horn cells and ventral roots at that level
- Ipsilateral loss of all sensation in a band - due to damage to the dorsal root entry zone at that segment
2. Below the Lesion - Ipsilateral Side
- Spastic weakness (UMN) with hyperreflexia and extensor plantar response (Babinski sign) - from interruption of the lateral corticospinal tract, which has already crossed above
- Loss of proprioception, vibration, two-point discrimination, and discriminative touch - from interruption of the dorsal column (fasciculus gracilis/cuneatus), whose fibers cross in the medulla
- Ipsilateral anhidrosis (loss of sweating) - from interruption of descending autonomic fibers in the ventral funiculus
- Ipsilateral Horner syndrome (ptosis, miosis, anhidrosis of the face) - if the lesion is in the cervical cord, disrupting the ciliospinal center of Budge (C8-T2)
3. Below the Lesion - Contralateral Side
- Loss of pain and temperature sensation - 1-2 dermatomes below the lesion level - from interruption of the spinothalamic tract, whose fibers have already crossed the midline from the opposite side
- "Crude touch" (poorly localized) is preserved on both sides because partial transmission occurs via both the ipsilateral dorsal column pathway and the crossed spinothalamic tract
4. Contralateral Side at and Above the Lesion
-
No specific deficits (the contralateral cord is intact)
-
Localization in Clinical Neurology, 8e, p. 257
-
Guyton and Hall Textbook of Medical Physiology, p. 615
-
Goldman-Cecil Medicine, p. 3847
Summary Table
| Feature | Side | Tract Involved |
|---|---|---|
| Spastic weakness (UMN) | Ipsilateral below lesion | Lateral corticospinal tract |
| LMN weakness, atrophy, fasciculations | Ipsilateral at level of lesion | Anterior horn cells/ventral root |
| Loss of proprioception, vibration, fine touch | Ipsilateral below lesion | Dorsal columns |
| Loss of pain and temperature | Contralateral (1-2 levels below) | Spinothalamic tract |
| Horner syndrome | Ipsilateral | Ciliospinal center (cervical lesions) |
| Anhidrosis | Ipsilateral below lesion | Descending autonomic fibers |
Classic vs. Brown-Séquard Plus
- Asymmetric hemiplegia
- Hypoalgesia more prominent on the less paretic side
- Bradley and Daroff's Neurology in Clinical Practice, p. 1306
Etiology / Causes
| Category | Examples |
|---|---|
| Trauma (most common) | Penetrating injuries (stab wounds, gunshots), blunt trauma, hyperextension injuries, rotational subluxation, unilateral laminar/pedicle fractures |
| Disc disease | Herniated cervical disc (most common non-traumatic cause) |
| Demyelinating | Multiple sclerosis |
| Neoplastic | Primary or metastatic spinal cord tumors |
| Vascular | Spinal cord ischemia, spinal epidural hematoma, hematomyelia, subdural hematoma |
| Infective/inflammatory | Arachnoiditis, epidural abscess, transverse myelitis |
| Other | Spinal cord herniation, cervical manipulation |
- Localization in Clinical Neurology, 8e, p. 257-258
- Campbell's Operative Orthopaedics 15th Ed 2026, p. 2470
Diagnosis
- Clinical - the pattern is distinctive, but easily missed unless each sensory modality is tested individually
- MRI is the imaging modality of choice - looks for structural or inflammatory causes, cord compression, disc herniation, tumors, or hematoma
- Bradley and Daroff's Neurology, p. 1306
Management
- Urgent decompression (surgical) if cord compression or spinal instability is present - prognosis for recovery is good when treated promptly
- If BSS follows penetrating trauma with anatomic cord sectioning, significant neurologic recovery is unlikely
- General SCI principles apply: airway/respiratory support, blood pressure management (avoid hypotension), bladder/bowel care, DVT prophylaxis, early rehabilitation
- In carefully selected patients, nerve or tendon transfers may offer functional benefit
- Campbell's Operative Orthopaedics 15th Ed 2026, p. 2470
Prognosis
- Gait typically recovers within 6 months
- Bowel and bladder continence is usually regained
- Patients with predominantly more upper extremity weakness (relative to lower extremity) have favorable ambulation outcomes
- Recovery can continue for up to 2 years
- Only BSS and central cord syndrome are statistically associated with improved recovery at 2 years post-injury
- Bradley and Daroff's Neurology in Clinical Practice, p. 1306
- Campbell's Operative Orthopaedics 15th Ed 2026, p. 2470
Comparison with Other Incomplete SCI Syndromes
| Syndrome | Motor loss | Sensory loss (pain/temp) | Sensory loss (proprioception) | Prognosis |
|---|---|---|---|---|
| Brown-Séquard | Ipsilateral UMN | Contralateral | Ipsilateral | Best |
| Central Cord | Arms > Legs (bilateral) | Variable | Variable | Moderate |
| Anterior Cord | Bilateral below | Bilateral below | Preserved | Worst |
| Posterior Cord | Preserved | Preserved | Bilateral below | Good |
- Miller's Review of Orthopaedics 9th Edition
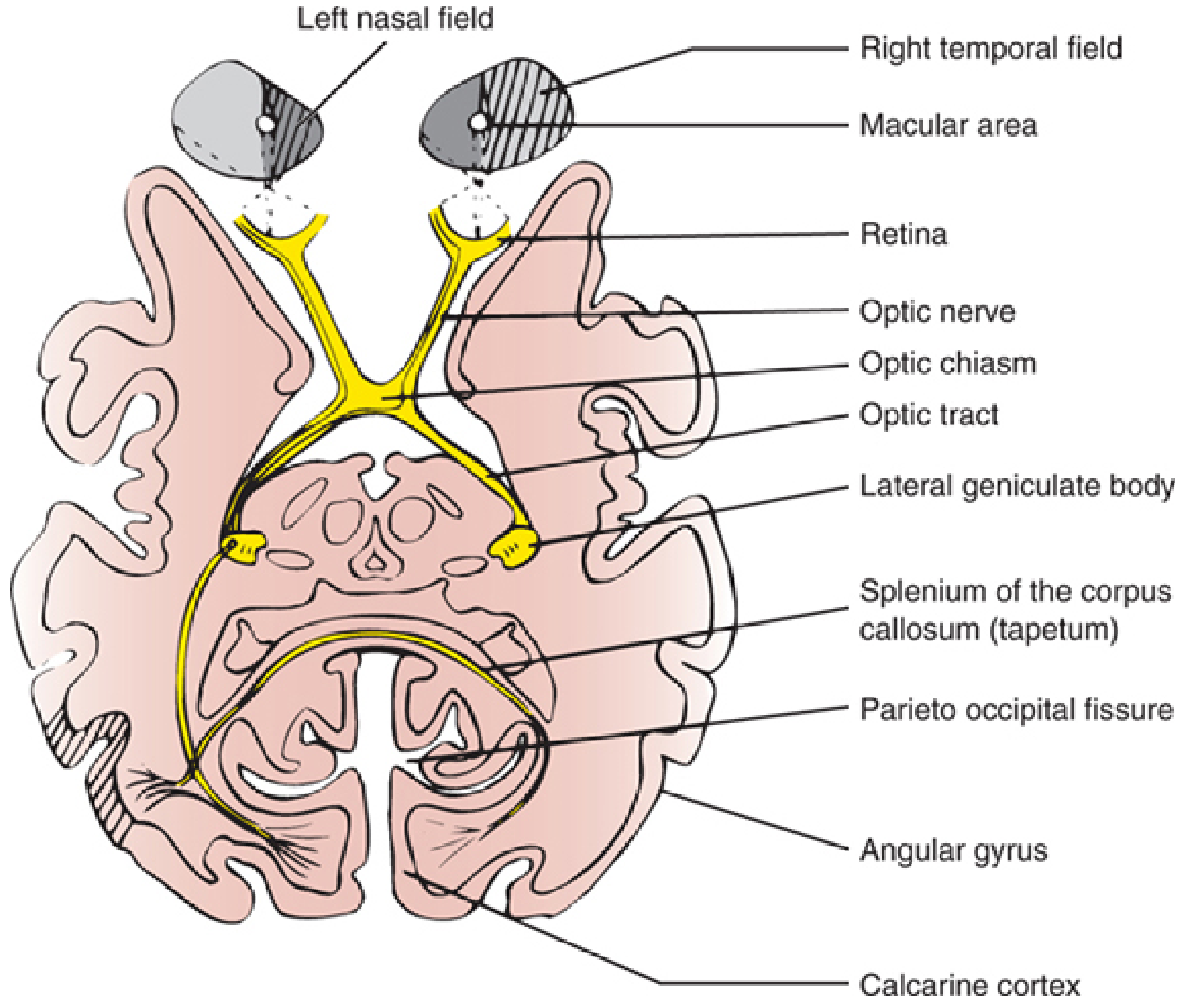
Visual pathway flowchart
Visual Pathway - Complete Flowchart & Notes
Anatomical Diagram
Step-by-Step Flowchart
LIGHT
│
▼
┌─────────────────────────────────────────────────────────┐
│ RETINA │
│ • Photoreceptors → Bipolar cells → Ganglion cells │
│ • Fovea/macula: highest visual acuity (cone-rich) │
│ • ~1.2 million ganglion cell axons converge at disc │
│ Cell types: │
│ M cells (10%) → WHERE / motion / depth / stereopsis │
│ P cells (90%) → WHAT / colour / fine detail │
└───────────────────┬─────────────────────────────────────┘
│ Ganglion cell axons form the
│ nerve fiber layer → optic disc
▼
┌─────────────────────────────────────────────────────────┐
│ OPTIC NERVE (CN II) │
│ • Axons acquire myelin (oligodendrocytes) post-disc │
│ • Covered by cranial meninges → CNS component │
│ • Superior fibers = superior; macular = central core │
│ • Blind spot = optic disc (no photoreceptors) │
└───────────────────┬─────────────────────────────────────┘
│ Both optic nerves converge
▼
┌─────────────────────────────────────────────────────────┐
│ OPTIC CHIASM (at anterior infundibular stalk) │
│ │
│ KEY CROSSING RULE: │
│ Nasal retina fibers (~53%) → CROSS to opposite tract │
│ Temporal retina fibers (~47%) → STAY ipsilateral │
│ │
│ ∴ Each optic TRACT carries the CONTRALATERAL │
│ half-field from BOTH eyes │
│ │
│ Inferior nasal fibers loop forward = Wilbrand knee │
│ (into proximal contralateral optic nerve) │
└──────┬──────────────────────────┬───────────────────────┘
│ Left optic tract │ Right optic tract
│ (right visual field) │ (left visual field)
▼ ▼
┌─────────────────────────────────────────────────────────┐
│ OPTIC TRACT │
│ • Courses around the midbrain │
│ • Small branch → pretectal area & superior colliculus │
│ (pupillary light reflex - does NOT go to LGN) │
│ • Majority → Lateral Geniculate Nucleus (LGN) │
└───────────────────┬─────────────────────────────────────┘
│
▼
┌─────────────────────────────────────────────────────────┐
│ LATERAL GENICULATE NUCLEUS (LGN) of thalamus │
│ 6 laminar layers: │
│ Layers 1-2 = Magnocellular (M cell input) │
│ Layers 3-6 = Parvocellular (P cell input) │
│ Upper retina → medial LGN (→ superior calcarine lip) │
│ Lower retina → lateral LGN (→ inferior calcarine lip) │
└───────────────────┬─────────────────────────────────────┘
│ Optic Radiations
│ (Geniculocalcarine tract)
┌─────────┴─────────┐
│ │
▼ ▼
SUPERIOR FIBERS INFERIOR FIBERS
(upper visual field) (lower visual field)
→ Parietal lobe → Meyer's Loop
→ Superior bank (temporal lobe)
calcarine fissure → Inferior bank
calcarine fissure
│ │
└─────────┬─────────┘
▼
┌─────────────────────────────────────────────────────────┐
│ PRIMARY VISUAL CORTEX (V1) = Area 17 │
│ Striate cortex, banks of calcarine fissure │
│ Occipital lobe │
│ Macular vision → POSTERIOR pole (large representation) │
│ Peripheral vision → ANTERIOR part of calcarine │
└───────────────────┬─────────────────────────────────────┘
│
┌─────────┴────────────┐
▼ ▼
DORSAL STREAM VENTRAL STREAM
("WHERE" pathway) ("WHAT" pathway)
V1 → V2 → MT/V5 V1 → V2 → V4 → IT
Parietal cortex Temporal cortex
Spatial location, Object recognition,
motion, depth colour, form
- Localization in Clinical Neurology, 8e, p. 325-331
- Ganong's Review of Medical Physiology, p. 209-211
- Gray's Anatomy for Students, p. 1346-1347
Visual Field Defects by Lesion Site
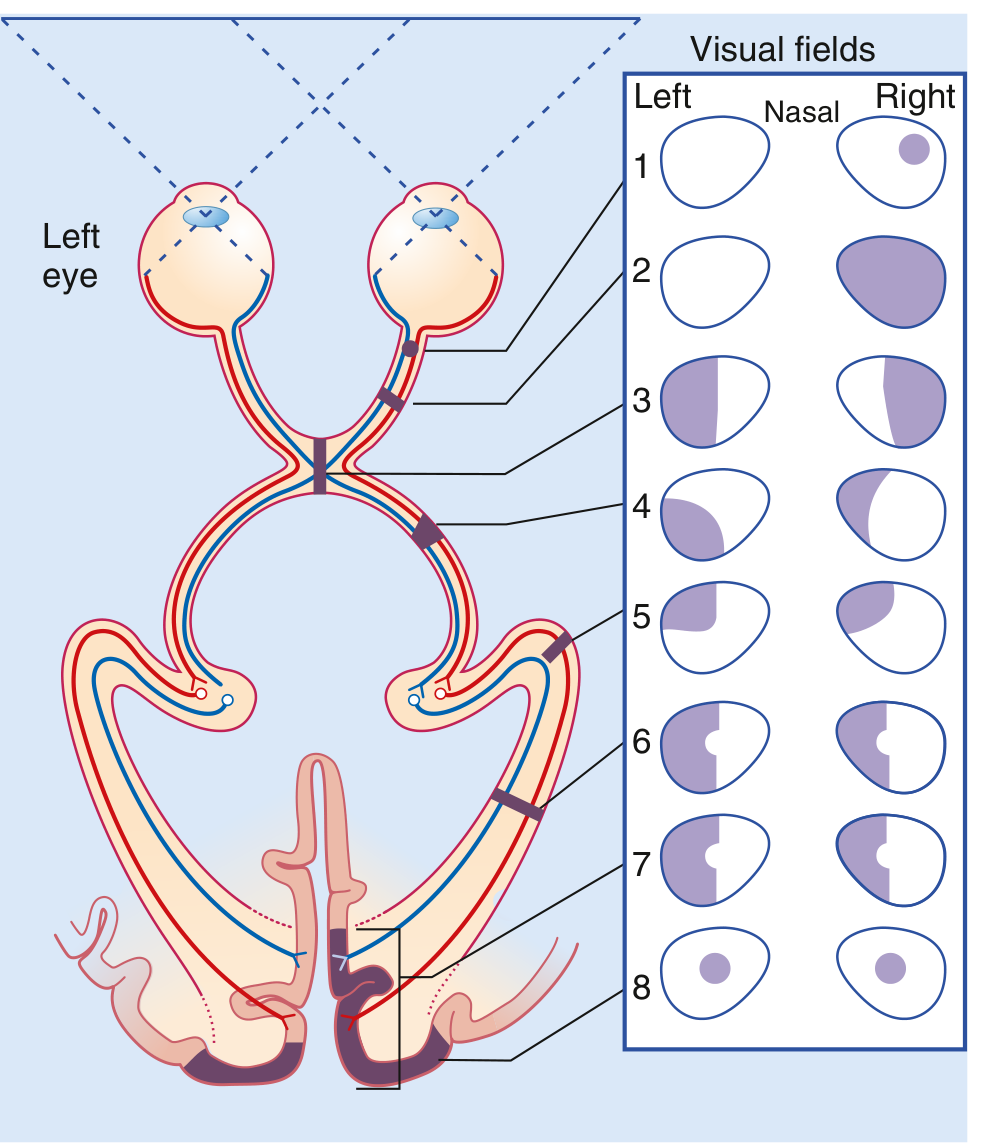
| Site of Lesion | Visual Field Defect | Key Cause |
|---|---|---|
| 1. Optic nerve (pre-chiasmal) | Ipsilateral monocular scotoma / blindness | MS, optic neuritis, trauma |
| 2. Complete optic nerve | Total monocular blindness (one eye) | Ischemic optic neuropathy |
| 3. Optic chiasm (central) | Bitemporal hemianopia (heteronymous) | Pituitary adenoma, craniopharyngioma |
| 4. Optic tract | Contralateral homonymous hemianopia | Stroke, tumor |
| 5. Meyer's Loop (temporal lobe radiation) | Contralateral superior quadrantanopia ("pie in the sky") | Temporal lobectomy, tumor |
| 6/7. Parietal lobe radiation | Contralateral homonymous hemianopia ± macular sparing | Stroke |
| 8. Occipital cortex (V1) | Contralateral homonymous hemianopia with macular sparing | PCA stroke (macula has dual MCA/PCA supply) |
| Bilateral occipital | Bilateral central scotoma / cortical blindness | Bilateral PCA infarcts |
- Ganong's Review of Medical Physiology, p. 210-211
- Gray's Anatomy for Students, p. 1347
Key Concepts to Remember
- M → magnocellular LGN → Layer 4Cα → Area MT → Dorsal "where" stream
- P → parvocellular LGN → Layer 4Cβ → Areas V3/V4 → Ventral "what" stream
Can you give me flowchart for mbbs 1st prof exam
Of visual pathway
A clean, detailed medical flowchart for MBBS 1st year exam on the Visual Pathway. The flowchart flows top to bottom with labeled boxes and arrows. Include these sequential steps with annotations: 1. LIGHT → RETINA (Photoreceptors: Rods & Cones → Bipolar Cells → Ganglion Cells; note: Macula = highest acuity, Fovea = cone-only zone, Blind spot = optic disc) 2. OPTIC NERVE (CN II) - note: myelinated by oligodendrocytes, covered by meninges = CNS structure 3. OPTIC CHIASM - show a split: NASAL retina fibers CROSS (decussate) to opposite side; TEMPORAL retina fibers STAY ipsilateral. Label: "After chiasm: each optic tract = contralateral half visual field from BOTH eyes" 4. OPTIC TRACT - note: small branch to Pretectal nucleus + Superior colliculus (pupillary light reflex branch) 5. LATERAL GENICULATE NUCLEUS (LGN), Thalamus - layers 1-2 Magnocellular (M cells), layers 3-6 Parvocellular (P cells) 6. OPTIC RADIATIONS (Geniculocalcarine tract) - split into two paths: Superior fibers via parietal lobe → superior calcarine bank; Inferior fibers via Meyer's Loop (temporal lobe) → inferior calcarine bank 7. PRIMARY VISUAL CORTEX V1 (Area 17, Calcarine fissure, Occipital lobe) - note: Macular vision = posterior pole (large area) 8. Two output streams: DORSAL STREAM (WHERE - motion, space → parietal) and VENTRAL STREAM (WHAT - colour, form → temporal) On the right side, add a separate column showing LESION → VISUAL FIELD DEFECT: - Optic nerve → Monocular blindness - Optic chiasm (central) → Bitemporal hemianopia - Optic tract → Contralateral homonymous hemianopia - Meyer's Loop (temporal) → Superior quadrantanopia (pie in the sky) - Occipital cortex → Homonymous hemianopia with macular sparing Use a white background, clean sans-serif font, blue boxes for main pathway, yellow for key notes, red for lesion-defect column. Make it suitable for exam revision.
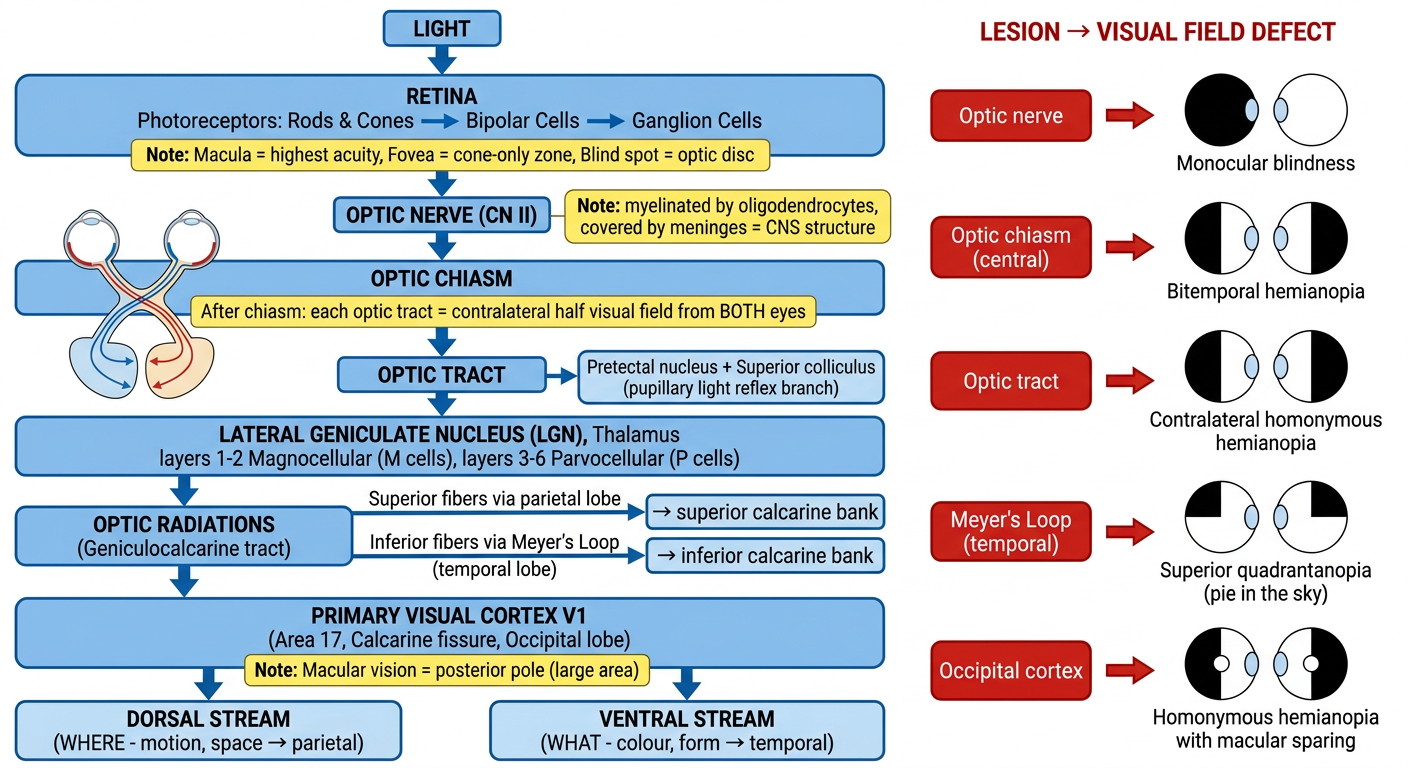
- Nasal fibers cross → temporal fibers stay
- After the chiasm, each optic tract carries the opposite half visual field from both eyes
| Lesion | Defect |
|---|---|
| Optic nerve | Monocular blindness (one eye only) |
| Optic chiasm (centre) | Bitemporal hemianopia (pituitary tumour classic) |
| Optic tract | Contralateral homonymous hemianopia |
| Meyer's loop (temporal lobe) | Superior quadrantanopia - "pie in the sky" |
| Occipital cortex (V1) | Homonymous hemianopia with macular sparing |