
962a4eb8-2a28-490f-a172-866973368049.jpeg
Windkessel effect
analyse_media
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Here is a thorough explanation of the Windkessel effect, drawing directly from your textbook image and the authoritative physiology textbook in the library.
Windkessel Effect
"Windkessel" is a German word meaning "wind chamber" or "air reservoir." The term was introduced by Otto Frank to describe how the aorta and large elastic arteries buffer pulsatile cardiac output into smooth, continuous peripheral flow.
Definition (from your textbook)
"Windkessel effect is the recoiling effect of blood vessels that converts the pulsatile flow of blood into a continuous flow."
Blood vessels that exhibit this are called Windkessel vessels (the aorta and large elastic arteries).
Why It Is Needed: The Problem of Pulsatile Flow
The heart ejects blood intermittently - only during systole. In the aorta:
- During systole: velocity rises to ~120 cm/sec
- During diastole: velocity falls to nearly zero (or even negative)
This variation exists even in large arteries. If this pulsatility were transmitted unchanged to the capillaries and tissues, organ perfusion would be intermittent and inefficient.
Mechanism
The two-model comparison below (from Medical Physiology) explains the mechanism beautifully:
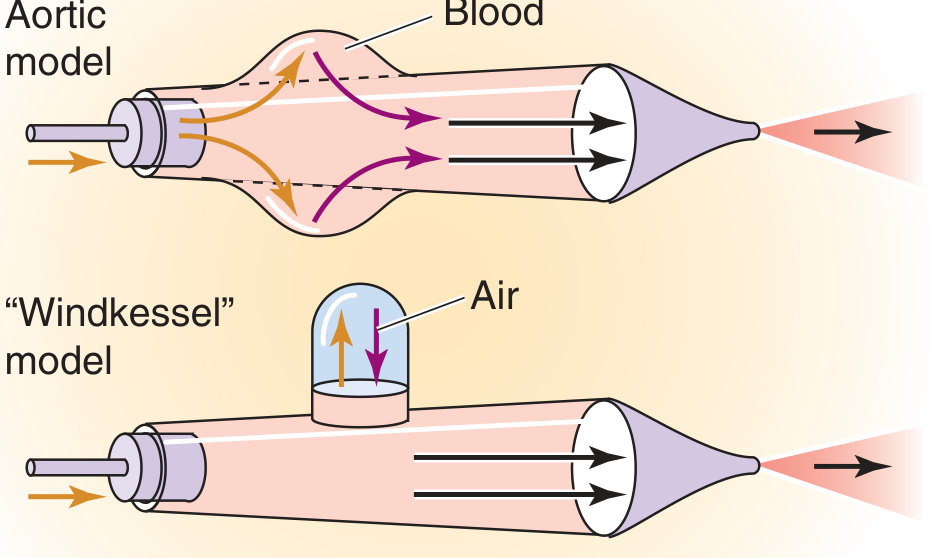
Top (Aortic model): During systole (gold arrows), the aortic wall bulges outward and stores the extra blood volume and energy. During diastole (violet arrows), the vessel recoils inward, pushing stored blood forward - maintaining forward flow even when the heart is not actively ejecting.
Bottom (Windkessel model): The mechanical equivalent - a rigid tube with a compressible air chamber above it. During systole, blood compresses the air (stores energy). During diastole, the compressed air pushes blood forward. The air chamber mimics aortic compliance.
| Phase | Aorta | Effect |
|---|---|---|
| Systole | Wall stretches, stores volume | Dampens peak pressure |
| Diastole | Wall recoils, expels stored blood | Maintains forward flow |
Key Physiological Consequences
-
Pulsatile → Continuous flow conversion: Capillary flow is steady and non-pulsatile, even though cardiac output is intermittent. This is entirely due to the Windkessel action of compliant arteries.
-
The aorta acts as a "second pump": As your textbook states, Windkessel vessels act as a second pump - the first pump being the heart. The aorta effectively extends the ejection period by releasing stored energy during diastole.
-
Improves pump efficiency: The Windkessel action converts phasic flow peaks into more continuous flow, considerably improving cardiac efficiency (Medical Physiology, p.754).
-
Diastolic blood pressure maintenance: The recoil of the aorta during diastole is what maintains diastolic blood pressure (DBP) above zero. Without this, DBP would fall to zero between beats.
The Rubber Tube Analogy (Glass vs. Rubber)
Medical Physiology uses a direct analogy:
- Glass tube (rigid, like a stiff artery): When a square-wave pressure pulse is applied, flow rises and falls instantly - perfectly mirroring the pressure pulse. Flow drops to zero between pulses.
- Rubber tube (compliant, like the aorta): During pressure, the tube slowly dilates and stores fluid. When pressure drops to zero, the expanded tube delivers its stored volume downstream - producing forward flow despite no driving pressure. The time-averaged outflow from the rubber tube actually exceeds that from the glass tube.
The aorta and large vessels behave like the rubber tube.
Effect of Aging on the Windkessel Effect
As arteries stiffen with age (arteriosclerosis):
- Compliance decreases
- Less energy is stored during systole
- Less smoothing of pulsatile flow occurs
- Systolic pressure rises (less damping), diastolic pressure falls (less recoil support)
- Pulse pressure widens - a hallmark of arterial stiffness
The velocity of pressure wave propagation also increases with stiffer walls, since energy can no longer dissipate into vessel expansion.
Mean Velocity of Blood Flow (Table from your textbook)
| Blood Vessel | Mean Velocity (cm/sec) |
|---|---|
| Large arteries | 50.00 |
| Small arteries | 5.00 |
| Arterioles | 0.50 |
| Capillaries | 0.05 |
| Venules | 1.00 |
| Small veins | 2.00 |
| Large veins | (highest among veins) |
Note that velocity is highest in large arteries and slowest at capillaries (despite maximal total cross-sectional area there).
Clinical Relevance
- Pulse pressure = Systolic BP - Diastolic BP. Widened pulse pressure in elderly patients reflects reduced Windkessel compliance.
- Aortic regurgitation: The regurgitant jet during diastole further reduces diastolic pressure - the Windkessel recoil is "wasted" back into the ventricle rather than driving peripheral flow.
- Hypertension treatment: Drugs that improve arterial compliance (e.g., ACE inhibitors, ARBs) partially restore Windkessel function.
- Arterial waveform analysis in anesthesia and ICU monitoring is modeled using Windkessel equations (2-element and 3-element models).
Sources:
- Your textbook image (Section 8: Cardiovascular System, p.556)
- Medical Physiology (Boron & Boulpaep), Box 22-2 "Effect of Aortic Compliance on Blood Flow," p.754-755
- Barash Clinical Anesthesia, 9e, "Principles of Operation" (arterial waveform modeling)
This is a shared conversation. Sign in to Orris to start your own chat.