I now have comprehensive content from multiple authoritative textbooks plus 6 real clinical images. Let me now deliver the complete, fully structured MS General Surgery long case.
LOWER LIMB PERIPHERAL VASCULAR DISEASE
MS General Surgery Long Case - University Examination Standard
Professor of General Surgery | Vascular Surgeon | University Examiner
Based on Bailey & Love 28th Ed, Sabiston, Schwartz, Rutherford's Vascular Surgery, Goldman-Cecil, Harrison's, S. Das, SRB Manual, Bedside Clinics - Makhan Lal Saha, plus SVS/ESVS/AHA/ACC/NICE Guidelines
SECTION 1: CLINICAL SCENARIO
The University Long Case Patient
Mr. Ramprakash Yadav, 58 years, Male, Farmer
Chief Complaints:
- Pain in both calves on walking - 2 years
- Pain in right foot at rest, worse at night - 3 months
- Non-healing ulcer right great toe - 6 weeks
History of Presenting Illness:
Mr. Yadav first noticed cramp-like pain in his right calf after walking about 200 metres, which subsided completely within 5 minutes of rest. Over two years this progressed: the claudication distance fell from 200 m to 50 m, and 3 months ago he developed constant burning pain in the right foot, worse at night, partially relieved by hanging the leg dependently over the bedside. Six weeks ago a small blister appeared on the tip of the right great toe following minor trauma from his farm work; it has not healed and has gradually enlarged.
Risk Factor Profile:
- Smoker: 25 pack-years (currently 1 pack/day)
- Type 2 Diabetes Mellitus: 8 years, on oral hypoglycaemics, poorly controlled (HbA1c 9.2%)
- Hypertension: 6 years, on amlodipine
- Dyslipidaemia: detected 2 years ago, on atorvastatin
- No prior vascular intervention
- Father died of "heart attack" at age 62
Drug History: Metformin 500 mg BD, Glipizide 5 mg BD, Amlodipine 5 mg OD, Atorvastatin 40 mg OD
Occupational History: Works barefoot in fields; repetitive minor trauma likely
Examination Findings
General: Middle-aged male, anxious, thin build, pallor +, nicotine stains on fingers
Vital Signs: BP 154/92 mmHg (right arm), PR 86/min regular, RR 16/min, Temp 98.6°F
Right Lower Limb (Affected Limb):
- Inspection: Limb pale in horizontal position; dependent rubor (Buerger's sign positive); hair loss below knee; thickened dystrophic toenails; 1.5 × 1.5 cm punched-out ulcer right great toe tip, sloughy base, no granulation, surrounding cellulitis; no oedema
- Skin temperature: Cool from mid-calf downwards; temperature gradient present
- Capillary refill: Right toes >5 seconds; left >3 seconds
- Pulses: Right femoral: present, reduced; right popliteal: absent; right posterior tibial: absent; right dorsalis pedis: absent
- Buerger's angle: 20° (normal >90°); positive Buerger's test
- Neurological: Reduced sensation right foot (stocking distribution - diabetic neuropathy)
Left Lower Limb: Femoral present, popliteal faint, posterior tibial faint, dorsalis pedis absent - asymptomatic contralateral PAD
Cardiovascular Examination: Irregular rhythm absent; no carotid bruits; mild aortoiliac bruit present on auscultation; aortic aneurysm not palpable
Working Diagnosis: Chronic Limb-Threatening Ischemia (CLTI) - Right lower limb. Rutherford Category 5, Fontaine Stage IV. WIfI: W2 I3 fI2. Background: atherosclerotic PAD with diabetic macrovascular and microvascular disease.
SECTION 2: RELEVANT SURGICAL ANATOMY
2.1 Arterial Anatomy of the Lower Limb
AORTA (Bifurcates at L4 - level of umbilicus)
|
COMMON ILIAC ARTERY
|
┌─────┴─────┐
INTERNAL EXTERNAL ILIAC
ILIAC ARTERY
(pelvic) |
FEMORAL ARTERY
(enters femoral triangle)
|
┌─────────┴──────────┐
PROFUNDA SUPERFICIAL
FEMORIS FEMORAL ARTERY (SFA)
(deep femoral) → runs in adductor canal
→ becomes POPLITEAL
at adductor hiatus
|
┌───────────────┼───────────────┐
ANTERIOR POSTERIOR PERONEAL
TIBIAL TIBIAL ARTERY
(→ Dorsal (→ Plantar
pedis) arteries)
Key Surface Anatomy Points:
- Femoral artery: Midpoint of inguinal ligament (midway between ASIS and pubic symphysis) - NOT the mid-inguinal point
- Popliteal artery: Midline of popliteal fossa, deepest structure; palpated with knee semi-flexed
- Posterior tibial: Midway between medial malleolus and medial border of Achilles tendon
- Dorsalis pedis: Between 1st and 2nd extensor tendons on dorsum of foot
Examiner Alert: "What is the difference between mid-inguinal point and midpoint of inguinal ligament?" - The femoral artery lies at the midpoint of the inguinal ligament (between ASIS and pubic symphysis). The mid-inguinal point (midway between ASIS and pubic symphysis) is where the deep inguinal ring lies and where the femoral nerve is located (just lateral to the artery). These two points are essentially the same - this is a classic examiner trap.
Profunda Femoris Artery: The most important collateral pathway. Arises 3-4 cm below inguinal ligament from the posterolateral aspect of the common femoral artery. Its branches (medial and lateral circumflex femoral) form critical collaterals around the hip and thigh when SFA is occluded.
Adductor (Hunter's) Canal: The SFA traverses this fibromuscular canal in the medial thigh from the apex of the femoral triangle to the adductor hiatus. It is bounded anteriorly by vastus medialis, posteriorly by adductor longus/magnus, and medially by the sartorius (roof). The SFA becomes the popliteal artery as it emerges through the adductor hiatus.
Angiosomes of the Foot (Taylor & Palmer concept):
| Angiosome | Source Artery | Territory |
|---|
| 1 | Calcaneal branch (posterior tibial) | Medial heel |
| 2 | Medial plantar artery | Medial sole |
| 3 | Lateral plantar artery | Lateral sole, plantar forefoot |
| 4 | Anterior perforating branch (peroneal) | Anterior ankle |
| 5 | Dorsalis pedis | Dorsum of foot, toes |
| 6 | Calcaneal branch (peroneal) | Lateral heel |
Clinical Significance (Viva favourite): Angiosome-directed revascularization - bypass/angioplasty targeting the vessel supplying the ischemic territory achieves better wound healing than indirect revascularization. Plantar foot wounds = target posterior tibial; dorsal wounds = target anterior tibial/dorsalis pedis.
2.2 Venous Anatomy
Superficial System
GREAT SAPHENOUS VEIN (GSV)
Origin: Medial aspect of dorsal venous arch
Route: Medial malleolus → medial leg → medial thigh
Terminates: Saphenofemoral junction (SFJ) at cribriform fascia
4 cm below & lateral to pubic tubercle
SHORT SAPHENOUS VEIN (SSV)
Origin: Lateral aspect of dorsal venous arch
Route: Behind lateral malleolus → midline of calf
Terminates: Saphenopopliteal junction (SPJ) - variable (60-70% at popliteal fossa level)
Deep System (follows arteries)
- Common femoral → Superficial femoral (FV) → Popliteal → Tibial veins (paired)
- All veins have bicuspid valves directing flow from superficial → deep and caudal → cranial
Perforating (Hunterian/Cockett) Veins
| Name | Location | Clinical Importance |
|---|
| Cockett I, II, III | 6, 12, 18 cm above medial malleolus | Most commonly incompetent; cause gaiter ulcers |
| Boyd's perforator | Upper medial calf | |
| Dodd's perforator | Lower thigh | |
| Hunterian | Mid-thigh | |
Direct perforators: connect axial superficial trunk to deep system. Indirect: connect muscular tributaries. Incompetent perforators drive venous hypertension.
2.3 Lymphatic Drainage
- Superficial lymphatics run with GSV → superficial inguinal nodes (horizontal group: drain perineum/gluteal region; vertical group: drain lower limb)
- Deep lymphatics run with deep vessels → deep inguinal nodes (medial to femoral vein, below cribriform fascia) → external iliac nodes
- Cloquet's (Rosenmüller's) node: Highest deep inguinal node in femoral canal - important in metastatic spread
- Stemmer's sign: Inability to pinch a fold of skin at base of second toe = positive = indicates lymphoedema
2.4 Peripheral Nerves (Clinically Critical)
| Nerve | Origin | Territory | Relevance in Vascular Disease |
|---|
| Femoral nerve | L2-L4 | Anterior thigh, medial leg (saphenous) | Adjacent to femoral artery - at risk in femoral cutdown |
| Sciatic nerve | L4-S3 | Posterior thigh, all of leg below knee | Ischemic neuropathy in severe PAD |
| Sural nerve | S1-S2 | Lateral foot | At risk in SSV surgery |
| Saphenous nerve | L3-L4 | Medial ankle/foot | At risk in GSV harvesting |
| Common peroneal | L4-S1 | Lateral calf, dorsum foot | Compression neuropathy in below-knee casts; injured in knee dislocation causing acute limb ischemia |
SECTION 3: CLASSIFICATIONS
3.1 ARTERIAL DISEASE CLASSIFICATIONS
Fontaine Classification (PAD/Chronic Ischemia)
┌──────────┬──────────────────────────────────────────────────────┐
│ Stage │ Clinical Features │
├──────────┼──────────────────────────────────────────────────────┤
│ I │ Asymptomatic PAD (ABI abnormal, no symptoms) │
├──────────┼──────────────────────────────────────────────────────┤
│ IIa │ Mild claudication (>200 m walking distance) │
├──────────┼──────────────────────────────────────────────────────┤
│ IIb │ Moderate-severe claudication (<200 m) │
├──────────┼──────────────────────────────────────────────────────┤
│ III │ Rest pain (ischemic rest pain) │
├──────────┼──────────────────────────────────────────────────────┤
│ IV │ Tissue loss (ulceration, gangrene) │
└──────────┴──────────────────────────────────────────────────────┘
Rutherford Classification (PAD - More Detailed)
| Category | Grade | Description |
|---|
| 0 | 0 | Asymptomatic |
| 1 | I | Mild claudication |
| 2 | I | Moderate claudication |
| 3 | I | Severe claudication |
| 4 | II | Ischemic rest pain |
| 5 | III | Minor tissue loss |
| 6 | III | Major tissue loss |
"CLTI" (Chronic Limb-Threatening Ischemia) = Rutherford 4, 5, 6 = Fontaine III-IV. The older term "Critical Limb Ischemia" has been replaced by CLTI in SVS/ESVS Global Vascular Guidelines 2019.
Rutherford Classification of ACUTE Limb Ischemia (Sabiston, Table 103.4)
| Category | Description | Sensory Loss | Muscle Weakness | Arterial Doppler | Venous Doppler |
|---|
| I - Viable | Not immediately threatened | None | None | Audible | Audible |
| IIa - Marginally threatened | Salvageable if promptly treated | Minimal (toes)/none | None | Absent | Audible |
| IIb - Immediately threatened | Requires immediate revascularization | More than toes + rest pain | Mild-moderate | Absent | Audible |
| III - Irreversible | Major tissue loss/permanent damage | Profound, anesthetic | Profound paralysis (rigor) | Absent | Absent |
(Modified from Rutherford et al., J Vasc Surg. 1997)
Viva Point: Category III ALI = PRIMARY AMPUTATION. Do NOT attempt revascularization - reperfusion of an irreversibly ischemic limb causes lethal reperfusion injury, myoglobinuria, acute renal failure, and multiorgan failure.
WIfI Classification (SVS 2014 - for CLTI wound staging)
W = Wound (0-3: none → gangrene/major tissue loss)
I = Ischemia (0-3: ABI >0.8 → ABI <0.4 or TBI <0.25)
fI = Foot Infection (0-3: none → severe/limb-threatening)
Used to stratify amputation risk vs. benefit of revascularization.
Embolism vs Thrombosis in Acute Limb Ischemia
| Feature | Embolism | In-situ Thrombosis |
|---|
| Onset | Sudden, catastrophic | Gradual (hours/days) |
| Prior claudication | Absent (normal artery) | Present (pre-existing PAD) |
| Contralateral pulses | Normal | Reduced/absent |
| Source | AF, MI, valvular disease, proximal aneurysm | Atherosclerotic plaque, graft, popliteal aneurysm |
| Skin changes | Marble-white to mottling | Mottled from outset |
| Treatment | Fogarty embolectomy (usually) | Thrombolysis / bypass preferred |
| Cardiac history | Often present | Less common |
| Atrial fibrillation | Common | Less common |
3.2 VENOUS DISEASE CLASSIFICATIONS
CEAP Classification (Bailey & Love 28th Edition)
C - CLINICAL CLASS
C0 = No signs
C1 = Telangiectasia/reticular veins
C2 = Varicose veins
C3 = Oedema
C4a = Pigmentation or eczema
C4b = Lipodermatosclerosis or atrophie blanche
C4c = Corona phlebectatica
C5 = Healed venous ulcer
C6 = Active venous ulcer
(suffix 's' = symptomatic, 'a' = asymptomatic, 'r' = recurrent)
E - AETIOLOGICAL
Ec = Congenital
Ep = Primary (no known cause)
Es = Secondary (post-thrombotic)
En = No venous cause identified
A - ANATOMICAL
As = Superficial
Ap = Perforator
Ad = Deep
An = No venous location identified
P - PATHOPHYSIOLOGICAL
Pr = Reflux
Po = Obstruction
Pr,o = Reflux + obstruction
Pn = No pathophysiology identifiable
Example: A patient with active venous ulcer due to post-thrombotic SFJ incompetence with great saphenous reflux:
CEAP: C6s, Ep, As,p, Pr
Villalta Scale (Post-Thrombotic Syndrome)
Scores 5 symptoms (pain, cramps, heaviness, paraesthesia, pruritus) and 6 signs (pretibial oedema, skin induration, hyperpigmentation, redness, pain on calf compression, new varicose veins) each 0-3:
- Score 0-4: No PTS
- Score 5-9: Mild PTS
- Score 10-14: Moderate PTS
- Score ≥15 or ulcer: Severe PTS
3.3 LYMPHATIC DISEASE CLASSIFICATION
Primary Lymphoedema
| Type | Onset | Genetics | Features |
|---|
| Milroy's disease | Congenital | VEGFR-3 mutation | Bilateral leg oedema from birth |
| Lymphoedema praecox | Puberty - <35 yrs | Often sporadic | Most common primary type; unilateral |
| Lymphoedema tarda | >35 years | - | Bilateral; M=F |
Secondary Lymphoedema
- Filariasis (Wuchereria bancrofti) - most common worldwide cause
- Malignancy/node dissection (breast, pelvic)
- Radiation fibrosis
- Infection/recurrent cellulitis
- Trauma
SECTION 4: COMPLETE HISTORY TAKING
Systematic History for Vascular Long Case
4.1 Claudication History
Ask:
- Where is the pain? (Site = level of occlusion)
- What brings it on? (Walking, stairs?)
- How far can you walk before pain starts? (Claudication distance in metres)
- Does it stop you? (Absolute claudication distance)
- What do you do? (Must STOP and rest)
- How long to recover? (Complete relief = arterial; incomplete = venous/neurogenic)
- Does it worsen uphill or carrying loads? (Arterial claudication does)
- Has the distance changed? (Progressive = worsening disease)
Anatomical localisation of claudication:
Buttock + thigh claudication = Aortoiliac (Leriche syndrome)
Thigh + calf = CFA/SFA disease
Calf only = SFA/popliteal disease ← MOST COMMON
Foot claudication = Tibial/pedal disease
Cross-questions:
- Q: What is the difference between arterial claudication and neurogenic (spinal stenosis) claudication?
| Feature | Arterial Claudication | Neurogenic Claudication |
|---|
| Site | Calf/buttock | Both legs + back |
| Relief | Standing still | Sitting/leaning forward |
| Walking uphill | Worse | Better (spine extended = better) |
| Cycling | Normal | Better (spine flexed) |
| Pulses | Reduced/absent | Normal |
| ABI | Reduced | Normal |
4.2 Rest Pain History
Characteristics:
- Constant, severe burning/aching pain in foot and toes (not calf)
- Worse at night - recumbency removes gravity-assisted flow
- Relieved by dependency - hanging leg out of bed (gravity increases perfusion pressure)
- May sleep in chair with leg dependent
- Patients walk at night to get relief
Viva Q: Why is rest pain worse at night?
Answer: Loss of gravity-assisted flow in recumbency, decreased cardiac output during sleep, and increased sympathetic vasomotor tone at night all reduce perfusion pressure below the threshold required to maintain tissue viability in a critically ischemic limb.
4.3 Tissue Loss / Ulcer / Gangrene History
- Duration, onset (spontaneous vs traumatic)
- Progressive or static?
- Depth (superficial vs deep)
- Surrounding skin changes
- Discharge (serous/purulent/foul-smelling)
- Previous similar ulcers?
- Treated previously?
4.4 Venous History
- Visible veins on legs (standing)
- Aching, heaviness, throbbing worse at end of day (improves with elevation)
- Ankle swelling (pitting)
- Skin changes: itching, eczema, pigmentation
- Previous DVT or pulmonary embolism
- Family history of varicose veins
- Pregnancy history (women)
- Occupational history (prolonged standing)
4.5 Risk Factor Interrogation
| Risk Factor | Questions to Ask |
|---|
| Smoking | Duration (years), packs/day, pack-years, current/ex-smoker, age started |
| Diabetes | Duration, type, treatment (OHA/insulin), control (latest HbA1c), complications |
| Hypertension | Duration, treatment, blood pressure control |
| Dyslipidaemia | When diagnosed, on statins, lipid values |
| Cardiac disease | AF (embolic source!), MI, angina, cardiac surgery, valve disease, CCF |
| Stroke/TIA | Carotid disease, previous episodes |
| CKD | Relevant for contrast nephropathy in angiography; affects anticoagulation |
| Family history | PVD, MI, stroke, aortic aneurysm |
Examiner Cross-Questions:
Q: What is Leriche Syndrome? How do you diagnose it clinically?
Answer: Leriche syndrome (aortoiliac occlusive disease) = triad of:
- Bilateral buttock and thigh claudication
- Impotence (due to internal iliac artery occlusion)
- Absent/reduced femoral pulses bilaterally
Named after René Leriche, described in 1940.
Q: Name the cardiac conditions that can cause acute limb ischemia by embolism.
Answer: Atrial fibrillation (most common, 50% of emboli), recent MI with mural thrombus, prosthetic heart valves, infective endocarditis, dilated cardiomyopathy, left atrial myxoma, paradoxical embolism through PFO.
SECTION 5: COMPLETE CLINICAL EXAMINATION
5.1 General Examination
Expose patient adequately: Both lower limbs fully exposed; patient in supine position; good lighting
| System | What to Look For | Significance |
|---|
| Build | Thin, wasted | Chronic disease, malnutrition, malignancy |
| Pallor | Anaemia | Contributes to ischemia |
| Nicotine staining | Fingers | Active smoker |
| Xanthelasma, arcus | Periorbital | Dyslipidaemia |
| Fundoscopy | Hypertensive/diabetic retinopathy | Systemic vascular disease |
| Pulse | Rate, rhythm (AF?) | AF = embolic source |
| BP | Both arms | Subclavian disease; hypertension |
| Carotid bruits | Stethoscope to neck | Associated carotid disease |
| Abdominal aorta | Midline pulsatile mass | AAA - coexistent |
| Aortic bruit | Epigastric auscultation | Aortoiliac disease |
5.2 Local Examination of the Lower Limb
INSPECTION (Always from feet to groin, both sides, standing AND lying)
Standing Examination:
- Varicose veins (only visible standing - collapse on lying)
- Distribution: GSV territory (medial leg) vs SSV territory (posterior calf)
- Saphena varix (expansile cough impulse at SFJ)
Lying Examination (supine):
| Sign | Description | Significance |
|---|
| Pallor | Limb pale horizontally | Arterial insufficiency |
| Dependent rubor | Deep red-purple colour on dependency | Severe PAD - maximal vasodilatation; Buerger's positive |
| Venous guttering | Veins collapse flat on elevation | Arterial; not venous |
| Hair loss | Below knee | Chronic ischemia |
| Nail changes | Thickened, brittle, dystrophic | Chronic ischemia |
| Skin atrophy | Shiny, taut skin | Chronic ischemia |
| Pigmentation | Haemosiderosis - brown ankles | CVI/post-thrombotic |
| Lipodermatosclerosis | Woody, indurated lower leg | Advanced CVI |
| Atrophie blanche | White atrophic skin patches | CVI |
| Eczema | Erythema, weeping | Venous eczema (CVI) |
| Oedema | Pitting vs non-pitting | Venous (pitting) vs lymphoedema (non-pitting) |
| Ulcer | Site, size, edge, base, depth, surrounding skin | Arterial vs venous vs neuropathic |
ULCER COMPARISON TABLE (Examiner Favourite)
| Feature | Arterial Ulcer | Venous Ulcer | Neuropathic Ulcer |
|---|
| Site | Tips of toes, heel, pressure points, between toes | Gaiter area (medial ankle) | Pressure points (ball of foot, heel) |
| Margin | Punched-out, well-defined | Sloping, irregular | Punched-out |
| Base | Pale, necrotic, no granulation | Granulation tissue, red/yellow slough | Variable, may be deep |
| Depth | Deep, may expose tendon/bone | Shallow | May be deep (Mal perforant) |
| Edge | Punched-out | Irregular, undermined | Punched-out |
| Surrounding skin | Pale, cold, atrophic | Pigmentation, eczema, LDS | Callous |
| Pain | Very painful (severe) | Moderate (relieved by elevation) | Painless (anaesthetic) |
| Pulses | Absent | Present (unless mixed) | Present (unless diabetic) |
| Bleeding | Minimal | Bleeds readily | Variable |
| Discharge | Scanty | Copious, serous/purulent | Variable |
REAL CLINICAL IMAGES FROM BAILEY & LOVE 28TH EDITION:
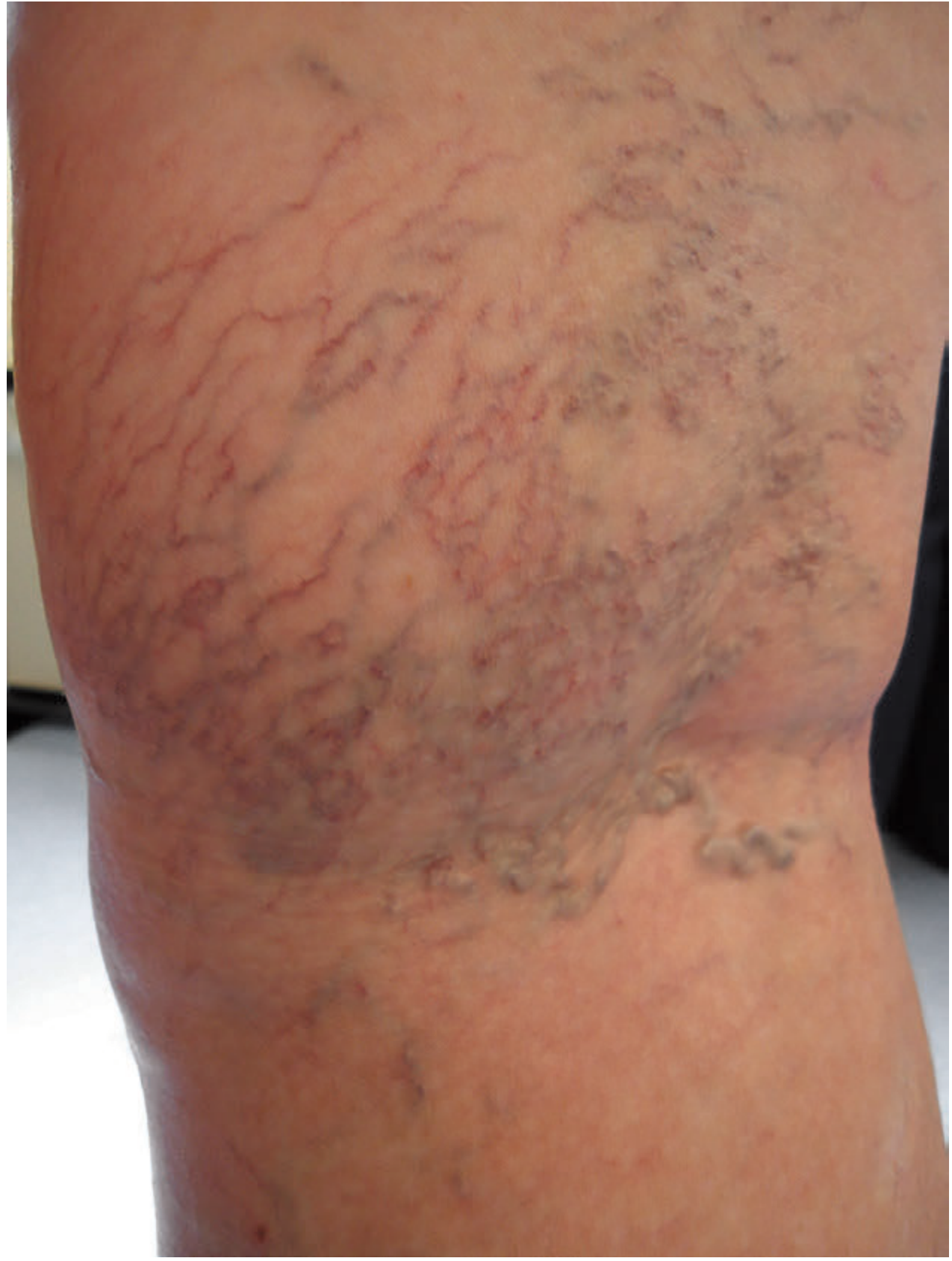
Telangiectasia and reticular veins (CEAP C1):
Figure 62.4 - Bailey & Love 28e: Telangiectasia and reticular veins. These small-vessel dilations represent CEAP C1 disease. They appear as fine red/purple branching networks just below the skin surface.
Advanced chronic venous skin changes - Lipodermatosclerosis, eczema, and atrophie blanche (CEAP C4b):
Figure 62.6 - Bailey & Love 28e: Advanced skin changes - lipodermatosclerosis (woody induration), eczema (erythematous dermatitis), and atrophie blanche (white atrophic patches). This represents CEAP C4b - severe chronic venous disease.
Pigmentation (haemosiderosis) and mild eczema (CEAP C4a):
Figure 62.9 - Bailey & Love 28e: Haemosiderosis (brown pigmentation) and mild lipodermatosclerosis of calf skin - CEAP C4a. The brown discolouration results from breakdown of red blood cells and deposition of haemosiderin in the dermis due to chronic venous hypertension.
Active venous ulcer (CEAP C6):
Figure 62.10 - Bailey & Love 28e: Active venous ulcer of the ankle/gaiter area. Note the irregular, sloping margins, granulating but sloughy base, surrounding haemosiderosis, and location in the classic gaiter zone over incompetent Cockett perforators. This is CEAP C6.
Pigmentation and haemosiderosis (bilateral comparison):
Figure 62.7 - Bailey & Love 28e: Comparison showing haemosiderosis and pigmentation (CEAP C4a) on one leg vs the normal contralateral limb. The marked brownish discolouration in the gaiter area represents chronic venous insufficiency with post-thrombotic changes.
5.3 PALPATION
Temperature Assessment:
- Use dorsum of hand (more sensitive than palmar surface)
- Start distally and move proximally
- Identify the level of temperature change (level of occlusion is typically one level above the thermal gradient)
- Compare both limbs
Tenderness:
- Homan's sign (calf pain on dorsiflexion) - DVT screening (sensitivity 50%, specificity 40% - unreliable, do not rely on it alone)
- Calf tenderness on palpation (DVT)
- Perimalleolar tenderness (venous/lymphatic)
Peripheral Pulses:
| Artery | Technique | Normal Finding |
|---|
| Femoral | Midpoint of inguinal ligament; use two fingers | Strong, bounding |
| Popliteal | Knee semi-flexed 30°; both thumbs anteriorly, fingers meet in midline of fossa | Deep, difficult - requires practice |
| Posterior tibial | Between medial malleolus and medial Achilles tendon; 2-3 fingers | Easily palpable |
| Dorsalis pedis | Lateral to EHL tendon, between 1st and 2nd metatarsals | Present in 90%; absent in 10% normal population |
Grading of Pulses:
- 0: Absent
- 1+: Diminished/barely palpable
- 2+: Normal
- 3+: Increased/bounding (aneurysm?)
- 4+: Markedly bounding
SECTION 6: PULSE EXAMINATION IN DETAIL
6.1 Femoral Pulse
Surface Anatomy: Midpoint of the inguinal ligament (midway between anterior superior iliac spine and pubic symphysis)
Technique:
- Patient supine, hip slightly externally rotated
- Press firmly with 2-3 fingers at the midpoint of inguinal ligament
- Feel for rhythmic pulsation; assess strength and character
- Auscultate over femoral artery for bruits (indicate stenosis)
Clinical Significance:
- Absent: Aortoiliac occlusion or common femoral artery occlusion
- Bruit: Significant stenosis (60-80%)
- Reduced: Proximal disease
- Aneurysmal: Pulsatile, expansile mass → Femoral artery aneurysm
Common Viva Questions:
- Q: What is a femoral aneurysm? How do you diagnose it? - Abnormal dilatation >1.5x normal; diagnosed on duplex; >2 cm = treat; bilateral in 50%; associated with AAA in 85%
- Q: What does an absent femoral pulse indicate? - Aortoiliac occlusive disease (tailor treatment accordingly: aortobifemoral bypass or aortofemoral bypass/iliac stenting)
6.2 Popliteal Pulse
Surface Anatomy: Midline of popliteal fossa, posterior to knee joint
Technique (Two methods):
- Prone method: Patient prone, knee flexed 30°; palpate with both thumbs on either side while fingers cup the fossa; press deeply in the midline
- Supine method: Knee flexed 30°; both hands cup the popliteal fossa; fingertips meet in the midline and press deeply
Clinical Significance:
- Easiest pulse to miss - presses deeply in the fossa
- Prominent popliteal pulse in an elderly patient = Popliteal Artery Aneurysm until proven otherwise (bilateral in 50%; associated with AAA; thromboembolism is the presenting complication)
- Absent: SFA/popliteal disease
- Hyperextension test (for popliteal entrapment in young athlete)
Common Viva Questions:
- Q: What is the most common peripheral arterial aneurysm? - Popliteal artery aneurysm (>50% of all peripheral aneurysms). Note: femoral is second most common.
- Q: What are the complications of popliteal aneurysm? - Distal thromboembolism (most common complication, can cause acute limb ischemia), local compression (DVT, nerve compression), rupture (rare)
6.3 Posterior Tibial Pulse
Surface Anatomy: Posterior to medial malleolus, in the groove between malleolus and medial border of tendo Achillis
Technique:
- Patient supine, foot relaxed
- Place 3 fingers in the groove behind medial malleolus
- Press against the posterior surface of the tibia
Clinical Significance:
- Most reliable below-knee pulse
- Absent in posterior tibial artery occlusion (tibial disease, often in diabetics)
- Always present in normal individuals (not absent in 10% like DP)
6.4 Dorsalis Pedis Pulse
Surface Anatomy: Dorsum of foot, in the groove between the tendons of extensor hallucis longus and extensor digitorum longus, at level of 1st-2nd metatarsal space
Technique:
- Foot relaxed, not plantarflexed
- Palpate with 2-3 fingers, light pressure
Clinical Significance:
- Absent in 10% of normal population (anatomical variant - replaced by peroneal perforator)
- If absent, DP is absent but PT may be present - check both
- Absent both DP and PT = significant tibial disease
Pearl: Before labelling dorsalis pedis as absent, confirm by auscultation with hand-held Doppler. Doppler signal present = vessel patent despite non-palpable pulse.
SECTION 7: SPECIAL CLINICAL TESTS
7.1 BUERGER'S TEST (Most Important Arterial Test at Bedside)
Indication: Assessment of arterial insufficiency of the lower limb
Technique:
- Elevation test: Patient supine; elevate both lower limbs to 45° for 1-2 minutes; observe foot colour
- Dependency test: Ask patient to sit up quickly and hang legs dependently; observe colour changes
Interpretation:
- Normal: Foot remains pink throughout; dependency causes no change
- Positive Buerger's test: Elevation causes pallor (Buerger's angle <20° = severe); dependency causes reactive hyperaemia (dusky red/purple "sunset foot")
- Buerger's angle: The angle of elevation at which pallor first appears
-
45°: Normal
- 20-45°: Moderate ischemia
- <20°: Severe ischemia (CLTI)
- Venous filling time: >15 seconds on going from elevation to dependency = significant ischemia (normal <10 sec)
Viva Questions:
- Q: What is the pathophysiology of dependent rubor in Buerger's test? - In severe ischemia, the arterioles are maximally vasodilated to maintain perfusion. On dependency, gravity increases the hydrostatic head but the stagnant, deoxygenated blood in maximally dilated capillaries produces the characteristic dusky red colour (dependent rubor = Buerger's sign = vasodilatory response exhausted).
7.2 ANKLE-BRACHIAL INDEX (ABI)
The most important non-invasive vascular test.
Technique:
- Patient supine, rested 10 minutes
- Place BP cuff on calf above ankle
- Locate dorsalis pedis or posterior tibial pulse with hand-held Doppler probe (8 MHz)
- Inflate cuff until signal disappears; deflate slowly; record pressure when signal returns
- Measure brachial systolic pressure (both arms; use higher)
- ABI = Ankle systolic pressure / Highest brachial systolic pressure
Interpretation:
| ABI Value | Interpretation |
|---|
| >1.3 | Non-compressible vessels (calcified; diabetics/ESRD) - use TBI |
| 0.9-1.3 | Normal |
| 0.7-0.9 | Mild PAD (often asymptomatic or mild claudication) |
| 0.5-0.7 | Moderate PAD (claudication) |
| 0.3-0.5 | Severe PAD (rest pain likely) |
| <0.3 | Critical ischemia/CLTI |
| <0.4 | Resting ankle pressure <50 mmHg = CLTI criterion |
Toe-Brachial Index (TBI): Used when ABI is falsely elevated (calcified vessels). TBI <0.7 = abnormal; TBI <0.3 = CLTI.
Limitations of ABI:
- Falsely elevated in diabetics and CKD (medial calcification = non-compressible vessels)
- Cannot differentiate level of disease
- Poorly correlated with symptoms in diabetics (due to neuropathy)
- Solution: Use TBI, segmental pressures, or pulse volume recordings
7.3 VENOUS SPECIAL TESTS
Trendelenburg Test (Brodie-Trendelenburg Test)
Purpose: Identifies incompetence at saphenofemoral junction (SFJ)
Technique:
- Patient supine; elevate leg to drain varicosities
- Apply tourniquet at groin (upper thigh) to compress SFJ
- Ask patient to stand
- Observe filling pattern:
- Negative test (normal): Veins fill slowly from below over 30 seconds (competent SFJ; perforators normal)
- Tourniquet controls filling: SFJ incompetence (release tourniquet → rapid filling = SFJ incompetent)
- Filling occurs despite tourniquet: Incompetent perforators below tourniquet
- Both above: SFJ + perforator incompetence
Multiple Tourniquet Test
Purpose: Identifies level of perforator incompetence
Apply tourniquets at: (1) Groin, (2) Upper thigh, (3) Below knee, (4) Upper calf
Patient stands: filling between tourniquets = perforators at that level
Perthes' Test
Purpose: Assesses deep vein patency before GSV ligation
Technique: Apply tourniquet below knee; ask patient to walk 1-2 minutes
- Normal deep system: Varicosities empty (deep veins competent; tourniquet compresses SV)
- Positive Perthes' test: Varicosities become MORE engorged and painful on walking → DO NOT OPERATE (deep system obstructed; GSV is the collateral; stripping would cause severe chronic venous insufficiency)
Schwartz Test
Purpose: Detects incompetent saphenofemoral junction clinically
Technique: Tap on varicosity in calf while palpating SFJ in groin
- Positive: Fluid impulse transmitted upwards = incompetent valves in GSV (no valves between tap point and SFJ)
Fegan's Test
Purpose: Maps location of incompetent perforating veins
Technique: Elevate leg; tap along course of varicosity; feel for fascial defects (blow-outs in deep fascia) and tenderness over incompetent perforators
Stemmer's Sign (Lymphoedema)
Technique: Attempt to pinch a fold of skin at the base of the second toe
- Positive (Stemmer's sign): Cannot pinch a fold = lymphoedema (fibrosis of dermis)
- Negative: Normal or venous oedema
Viva Q: What is the difference between pitting and non-pitting oedema?
- Pitting: Venous/cardiac/hepatic/renal (fluid easily displaced)
- Non-pitting: Lymphoedema (protein-rich fluid + fibrosis); myxoedema
- Positive Stemmer = lymphoedema confirmed
SECTION 8: DIFFERENTIAL DIAGNOSIS
8.1 Arterial vs Venous vs Neuropathic vs Lymphatic Disease
| Feature | Arterial | Venous | Neuropathic | Lymphatic |
|---|
| Dominant symptom | Pain (claudication/rest) | Aching, heaviness | Painless deformity | Swelling |
| Swelling | Absent (or dependent rubor) | Pitting oedema | Absent (or neuropathic joint) | Non-pitting oedema |
| Skin colour | Pale (elevation), red (dependency) | Brown pigmented | Normal/callused | Normal |
| Skin temperature | Cold | Normal/warm | Normal | Normal |
| Pulses | Reduced/absent | Present | Present | Present |
| Ulcer site | Tips of toes/heel | Gaiter zone (medial ankle) | Pressure points (plantar) | Rare |
| Ulcer pain | Very painful | Moderate | Painless | |
| Hair loss | Present | Absent | Absent | Absent |
| ABI | Reduced | Normal | Normal/high (calcified) | Normal |
| Oedema type | None | Pitting | None | Non-pitting |
| Varicosities | Absent | Present | Absent | Absent |
8.2 DVT vs Cellulitis vs Lymphoedema
| Feature | DVT | Cellulitis | Lymphoedema |
|---|
| Onset | Sudden | Sudden (fever/entry wound) | Chronic/progressive |
| Fever | Low-grade | High fever | Absent |
| Tenderness | Calf, along vein | Diffuse, skin | Absent initially |
| Erythema | Mild, dusky | Bright red, warm, spreading | Absent unless infected |
| Oedema type | Pitting | Pitting | Non-pitting |
| Stemmer's sign | Negative | Negative | Positive |
| D-dimer | Elevated | Normal/mildly elevated | Normal |
| Duplex | Thrombus in vein | Normal veins | Normal veins |
| Skin | Dilated superficial veins | Hot, erythematous | Thickened, verrucous |
| Wells score | Calculate (DVT likely if ≥2) | Not applicable | Not applicable |
SECTION 9: UNIVERSITY LONG CASE PRESENTATION (5 minutes)
How to Present:
"Sir/Madam, I would like to present Mr. Ramprakash Yadav, a 58-year-old male farmer, with a significant vascular history and current presentation of chronic limb-threatening ischemia of the right lower limb.
Presenting complaints: He presents with a two-year history of right calf claudication, progressive in nature, now occurring at less than 50 metres walking distance. Over the last three months he has developed rest pain in the right foot, constant, burning in character, worse at night, and partially relieved by hanging the leg over the bedside. Six weeks ago he developed a non-healing ulcer at the tip of the right great toe following minor trauma.
Relevant risk factors: He is a 25 pack-year active smoker. He has poorly-controlled Type 2 Diabetes Mellitus for 8 years, Hypertension for 6 years, and Dyslipidaemia for 2 years.
Examination findings: On general examination, he is thin, anxious, with nicotine-stained fingers and mild pallor. His blood pressure is 154/92 mmHg with a regular pulse of 86 per minute.
On local examination of the right lower limb, inspection shows a pale limb with dependent rubor, hair loss below the knee, thickened dystrophic toenails, and a 1.5 cm punched-out ulcer at the tip of the right great toe with a sloughy base and surrounding cellulitis. Buerger's angle is less than 20 degrees. All pulses below the right femoral are absent - the popliteal, posterior tibial, and dorsalis pedis are not palpable. Capillary refill time in the right toes exceeds 5 seconds. Skin temperature is cool from mid-calf downwards.
The left limb shows faint popliteal and posterior tibial pulses with absent dorsalis pedis - suggesting asymptomatic contralateral PAD.
Neurological examination reveals a stocking-distribution sensory deficit in the right foot consistent with diabetic peripheral neuropathy.
Working diagnosis: This patient has Chronic Limb-Threatening Ischemia of the right lower limb, Rutherford Category 5, Fontaine Stage IV, most likely on the basis of atherosclerotic peripheral arterial disease against a background of diabetes, hypertension, dyslipidaemia, and heavy smoking.
My planned investigations are: ABI/TBI measurement, duplex Doppler ultrasound, CT angiography for anatomical delineation, and a full metabolic screen including HbA1c, fasting lipids, renal function, and 12-lead ECG. Echocardiography would be performed if an embolic source needs to be excluded.
My management plan: Urgent risk factor control - smoking cessation, strict glycaemic control, blood pressure optimisation, and statin therapy. I would discuss this case in a multidisciplinary vascular meeting to plan revascularization - either endovascular (angioplasty/stenting) or open surgical (femoro-distal bypass preferably with autologous great saphenous vein conduit). Wound care with debridement and treatment of the surrounding cellulitis with antibiotics. The goal is limb salvage."
SECTION 10: INVESTIGATIONS
10.1 Basic Blood Investigations
| Investigation | Purpose | Key Values |
|---|
| CBC | Anaemia (worsens ischemia), polycythaemia (thrombosis risk), thrombocytosis | Hb, WBC, platelets |
| Blood glucose / HbA1c | Diabetic control | HbA1c target <7% |
| Fasting lipid profile | LDL target <70 mg/dL in PAD | LDL, HDL, TGs |
| Renal function (BMP) | CKD - contrast nephropathy risk; affects drug dosing | Creatinine, eGFR |
| Coagulation profile | Pre-op; thrombophilia workup | PT, aPTT, INR |
| ECG | AF (embolic source), prior MI, LVH | Rhythm, ischemic changes |
| Chest X-ray | Cardiac size, pulmonary infiltrates | - |
10.2 Thrombophilia/Hypercoagulable Workup
When to order: Young patient (<45y) with arterial or venous thrombosis without obvious risk factors, recurrent DVT, or unusual sites
| Test | Condition |
|---|
| Protein C, Protein S | Deficiency → venous thrombosis |
| Antithrombin III | Deficiency → heparin resistance |
| Factor V Leiden | Most common inherited thrombophilia |
| Prothrombin G20210A | Second most common |
| Antiphospholipid antibodies | Antiphospholipid syndrome (Hughes syndrome) - arterial + venous |
| Homocysteine | Hyperhomocysteinaemia - early atherosclerosis |
| ANCA | Buerger's disease (negative) |
10.3 Non-Invasive Vascular Studies
Duplex Doppler Ultrasound
The gold standard first-line investigation for both arterial and venous disease.
Arterial Duplex:
- B-mode: visualises plaque, stenosis, aneurysm
- Colour Doppler: flow direction and turbulence
- Spectral Doppler: waveform analysis
Normal Doppler Waveforms:
TRIPHASIC (normal lower limb artery):
___
/ \
/ \___ (reverse flow component)
___ (forward diastolic component)
BIPHASIC (moderate disease):
___
/ \
/ \_____ (forward flow only, no reverse)
MONOPHASIC (severe disease/stenosis):
____
/ \________ (blunted, slow, forward flow only)
Venous Duplex Criteria for DVT:
- Non-compressibility of vein (most sensitive criterion)
- Absent spontaneous flow
- Absent augmentation
- Absent phasic flow with respiration
CT Angiography (CTA)
Gold standard pre-operative anatomical mapping for revascularization planning.
- Images aorta to foot in one scan
- Identifies: occlusion level, calcification, run-off vessels, aneurysms
- Contrast nephropathy risk: Hydrate pre-contrast; stop metformin 24-48h before; monitor creatinine
- Calcium blooms obscure vessel lumen in heavily calcified tibial arteries (limitation)
MR Angiography (MRA)
- No ionising radiation, no iodinated contrast (use gadolinium)
- Better soft-tissue contrast
- Tends to overestimate stenosis
- Contraindicated with metallic implants, claustrophobia
- Preferred in CKD (no nephrotoxic iodinated contrast) - but gadolinium can cause nephrogenic systemic fibrosis in eGFR <30
Digital Subtraction Angiography (DSA)
- Gold standard for intervention - allows simultaneous diagnosis and treatment
- Subtraction removes bony background, showing pure vascular anatomy
- Risk: Contrast nephrotoxicity, arterial access site complications, embolisation
- Used when CTA/MRA inconclusive or immediately before/during endovascular intervention
10.4 Investigation Algorithm
SUSPECTED LOWER LIMB ISCHEMIA
│
┌──────┴──────┐
ACUTE (<2wks) CHRONIC (>2wks)
│ │
▼ ▼
Immediate CTA ABI Measurement
or urgent DSA │
│ ┌────┴────┐
▼ ABI ≤0.9 ABI >1.3
Emergency (PAD) (Calcified)
management │ │
Duplex Toe-Brachial
Doppler Index (TBI)
│
Asymptomatic Symptomatic
│ │
Treat risk Duplex for anatomy
factors +
CTA/MRA if revascular-
ization planned
SECTION 11: EVIDENCE-BASED MANAGEMENT
11.1 Medical Management (All Stages)
Smoking Cessation
The single most important intervention in PAD (Bailey & Love, Sabiston, SVS guidelines all agree)
- Increases claudication distance more than any drug
- Reduces progression to CLTI
- Reduces amputation rate
- Reduces cardiovascular mortality
- NRT, varenicline, bupropion; referral to cessation services
Antiplatelet Therapy
- Aspirin 75-100 mg daily OR Clopidogrel 75 mg daily (slightly superior in CAPRIE trial)
- Dual antiplatelet (DAPT) for 1-3 months post-endovascular stenting
- SVS 2016 Guidelines: Clopidogrel monotherapy preferred for symptomatic PAD
Statins
- Target LDL <70 mg/dL (or 50% reduction) - AHA/ACC 2018
- Atorvastatin 40-80 mg; Rosuvastatin 20-40 mg
- Anti-inflammatory + lipid-lowering + pleiotropic effects
- Reduces cardiovascular events AND limb events
Blood Pressure Control
- Target <130/80 mmHg (AHA/ACC 2017)
- ACE inhibitor/ARB preferred in diabetics
- Avoid beta-blockers in severe PAD (peripheral vasoconstriction worsens claudication) - though in practice cardioselective beta-blockers are used if indicated for cardiac reasons
Glycaemic Control
- HbA1c target <7% (diabetics)
- Strict control reduces microvascular complications
- SGLT2 inhibitors (empagliflozin) have cardioprotective benefit
Exercise Therapy
- Supervised exercise programme = first-line for claudication (Class IA evidence, AHA/ACC, NICE)
- 30-45 minutes walking, 3 times/week, for at least 12 weeks
- Promotes collateral development, increases claudication distance by 100-150%
- More effective than angioplasty for claudication in most trials (CLEVER trial)
Cilostazol
- Phosphodiesterase III inhibitor; vasodilatory + antiplatelet
- Increases pain-free and maximum walking distance by 40-50%
- Contraindicated in heart failure
- 100 mg BD; drug of choice for claudication pharmacotherapy
Anticoagulation
- Not routinely used in chronic PAD
- Indicated for: AF (DOACs), acute DVT, post-bypass graft thrombosis, antiphospholipid syndrome
- Low-dose rivaroxaban 2.5 mg BD + aspirin 100 mg (COMPASS trial) - reduces MACE and MALE in PAD
11.2 Endovascular Management
Principles
TASC II (Trans-Atlantic Inter-Society Consensus) classification guides morphology-based decision:
| TASC Class | Aortoiliac Lesion | Recommendation |
|---|
| A | Short (<3 cm) single stenosis | Endovascular first |
| B | Multiple <3 cm or single 3-10 cm | Endovascular preferred |
| C | Single >5 cm, bilateral >3 cm, unilateral iliac | Surgery preferred |
| D | Occlusions >2 cm, bilateral CFA, diffuse disease | Open surgery |
Balloon Angioplasty (PTA)
- Wire crosses lesion; balloon inflated to dilate stenosis/occlusion
- Best results: Iliac > SFA > tibial vessels
- Primary patency: Iliac ~70-85% at 5 years; SFA ~50% at 1 year
Drug-Coated Balloons (DCB)
- Paclitaxel-coated balloon inhibits neointimal hyperplasia
- Superior to plain balloon angioplasty in SFA disease (IN.PACT Admiral trial)
- Reduces re-stenosis rates
- Currently used for femoropopliteal segment
Stenting
- Self-expanding nitinol stents for SFA/iliac
- Bare metal stents → Drug-eluting stents (DES) for tibial vessels
- Stenting reserved for: failed/recoil after PTA, residual stenosis >30%, flow-limiting dissection
Atherectomy
- Directional, rotational, orbital, or laser atherectomy
- Removes plaque rather than dilating it
- Useful in heavily calcified lesions
- High re-stenosis rates - usually combined with DCB
Catheter-Directed Thrombolysis (CDT)
- For acute/subacute limb ischemia (ALI - Rutherford IIa/IIb)
- Infuse tPA into thrombus via catheter over 12-24 hours
- Advantages: Opens occluded grafts/bypasses; reveals underlying stenosis treatable by PTA; lower morbidity than open surgery
- Contraindications: Stroke within 3 months, active bleeding, major surgery within 10 days, Category III ALI
- Complication: Haemorrhage (intracranial haemorrhage 1%)
11.3 Open Surgical Management
Embolectomy (Fogarty Catheter Technique)
Indication: Arterial embolism (Rutherford IIa/IIb), failed thrombolysis
Fogarty Balloon Catheter - Steps:
- Groin incision; expose common, superficial, and profunda femoral arteries
- Systemic heparin 5000 IU IV
- Arteriotomy (transverse preferred to avoid narrowing)
- Pass Fogarty catheter distally (2F-4F) through tibial vessels to remove distal clot
- Pass Fogarty catheter proximally to remove proximal clot
- Irrigate with heparinised saline
- Check back-bleeding (venous) and forward-bleeding (arterial pulsation)
- Confirm flow with intraoperative Doppler or angiogram
- Close arteriotomy with patch if needed; 6-0 prolene continuous suture
- Four-compartment fasciotomy if ischemia >4-6 hours
Viva Q: Name the sizes and use of Fogarty catheters.
- 2F: Tibial vessels
- 3F: Popliteal, tibial
- 4F: SFA, popliteal
- 5-6F: Common femoral, iliac
- 7F: Aorta
Femoropopliteal Bypass
Indications: CLTI (Rutherford 4-6), severe claudication resistant to medical/endovascular therapy, failed angioplasty
Conduit Choice:
- First choice: Autologous great saphenous vein (GSV) - Reversed or in-situ
- Superior long-term patency (5-year patency 70-80%)
- Resistant to infection
- Ideal for below-knee anastomosis
- Alternative: PTFE (polytetrafluoroethylene) prosthetic graft
- Above-knee popliteal bypass: PTFE acceptable (5-year patency 50-60%)
- Below-knee: inferior results with PTFE; vein strongly preferred
In-situ Bypass (Hall technique):
- GSV left in situ; valves destroyed with valvulotome
- GSV tributaries ligated
- Proximal and distal anastomoses
- Advantage: Better size match between vein and artery at each end
Reversed Vein Bypass:
- GSV harvested, reversed (so valves don't obstruct flow), anastomosed
- Traditional technique
Operative Steps (Above-knee Femoropopliteal Bypass):
- Supine; padding under knee; thigh externally rotated
- Groin incision: expose CFA, SFA origin, PFA
- Medial thigh incision: expose above-knee popliteal artery at adductor hiatus
- Harvest GSV from same or opposite leg
- Systemic heparin 5000 IU IV
- Clamp SFA; proximal anastomosis: end-to-side with 5-0 prolene
- Tunnel graft through subsartorial plane
- Distal anastomosis: end-to-side to above-knee popliteal with 6-0 prolene
- Release clamps; check graft pulsation and Doppler signal
- Achieve haemostasis; close wounds in layers
Anastomotic Technique Points:
- Always end-to-side anastomoses (preserves native circulation)
- Prolene suture (monofilament, non-absorbable)
- Parachute technique for posterior wall of anastomosis
- Suture bites: 1-2 mm from edge, 1-2 mm apart
- No tension; adequate mobilisation of vessels
Aortobifemoral Bypass
Indication: Aortoiliac occlusive disease (Leriche syndrome); TASC C-D lesions
Conduit: Dacron bifurcated graft (16×8 mm or 14×7 mm most common)
Operative Steps:
- Supine; transperitoneal or retroperitoneal approach
- Expose infrarenal aorta (between renal arteries and IMA)
- Expose both common femoral arteries through groin incisions
- Systemic heparin 5000 IU IV
- Proximal clamp below renal arteries; distal clamp on aorta
- Proximal anastomosis: end-to-end (aortic occlusion) or end-to-side (aortic stenosis)
- Tunnel each limb of graft retro-peritoneally to respective groin
- Distal anastomoses: end-to-side to CFAs
- Close retroperitoneum to cover graft (prevents aortoenteric fistula)
5-year patency: 80-85%
Fasciotomy
Indications:
- Compartment syndrome following revascularization
- Ischemia time >4-6 hours before reperfusion
- Prophylactic after embolectomy in severely ischemic limb
Four-Compartment Fasciotomy of Leg:
TWO-INCISION TECHNIQUE:
Lateral incision (fibula):
- Opens anterior compartment (between fibula and tibia anteriorly)
- Opens lateral compartment (between fibula and lateral skin)
Medial incision (medial calf):
- Opens superficial posterior compartment
- Opens deep posterior compartment
Compartment pressure >30 mmHg, or within 20-30 mmHg of diastolic pressure = Fasciotomy indicated
Amputation Decision-Making
AMPUTATION DECISION ALGORITHM
│
IRREVERSIBLE ISCHEMIA
(Rutherford III)
OR
Failed all revascularization
OR
No suitable conduit/runoff
OR
Life expectancy poor / non-ambulatory
│
┌──────┴──────┐
Viable Not viable
below-knee below-knee
tissues tissues
│ │
Below-knee Above-knee
amputation amputation
(BKA) (AKA)
│
Goal: Preserve knee joint
(functional prosthetic)
Stump length: 12-15 cm
below tibial tuberosity
Amputation Levels:
- Toe/ray amputation: Single digit; for localised gangrene
- Transmetatarsal: Forefoot gangrene
- Syme's amputation: Through ankle joint
- Below-knee (BKA): Ideal if knee can be preserved; best functional outcome
- Knee disarticulation: Rarely used
- Above-knee (AKA): When BKA not viable; higher mortality, poorer prosthetic outcome
- Hip disarticulation: Extreme tissue loss/sepsis
Key Pearl: A healed BKA is far superior to an AKA. Preserve the knee if possible - a BKA with a good prosthesis allows near-normal walking; AKA requires 60-80% more energy expenditure.
SECTION 12: OPERATIVE DISCUSSION
Fogarty Catheter Embolectomy - Complete Operative Description
Instruments
- Standard vascular set
- Fogarty balloon catheters (2F, 3F, 4F)
- Vessel loops (red for artery, yellow for vein)
- Bulldog clamps (DeBakey, Cooley)
- Vascular clamps (Satinsky, Potts)
- 5-0 and 6-0 Prolene sutures on BV needles
- Heparinised saline syringe
- Doppler probe (sterile)
Pitfalls
- Vigorous balloon inflation causes intimal injury/dissection - inflate gently
- Failure to check for distal clot - always pass catheter to level of foot
- Missing underlying stenosis - always do intraoperative angiogram
- Not considering compartment syndrome - prophylactic fasciotomy in prolonged ischemia
Complications
- Haemorrhage
- Vessel injury / intimal tear
- Distal embolisation
- Re-thrombosis
- Compartment syndrome / reperfusion injury
- Wound infection
- Lymphocele
SECTION 13: COMPLICATIONS AND MANAGEMENT FLOWCHARTS
Reperfusion Injury
Mechanism: Reintroduction of oxygenated blood to ischemic tissue generates reactive oxygen species (ROS); neutrophil activation; endothelial damage; systemic inflammatory response
Systemic effects:
- Myoglobinuria → Acute renal failure
- Hyperkalaemia (from ischemic muscle)
- Metabolic acidosis
- Cardiac arrhythmias
- ARDS / SIRS / MODS
Management:
- IV hydration pre- and post-reperfusion
- Sodium bicarbonate to alkalinise urine (reduces myoglobin precipitation)
- Monitor urine output (target >1 mL/kg/hr)
- Monitor ECG for arrhythmias
- Consider prophylactic fasciotomy
Graft Occlusion
GRAFT OCCLUSION
│
┌───┴───┐
Early Late
(<30 days) (>2 years)
│ │
Technical Intimal
failure hyperplasia
Thrombosis Neo-atherosclerosis
│ │
▼ ▼
Re-explore Thrombolysis
or or
Thrombolysis Re-do bypass
SECTION 14: COMPLETE VIVA SECTION
100+ Examiner Questions with Model Answers
ANATOMY VIVA
Q1. Where do you palpate the femoral pulse?
Midpoint of the inguinal ligament - halfway between the anterior superior iliac spine (ASIS) and the pubic symphysis.
Q2. What are the contents of the femoral triangle from lateral to medial?
Lateral to medial: Femoral NERVE, Femoral ARTERY, Femoral VEIN, Lymphatics. Mnemonic: NAVAL - Nerve, Artery, Vein, And Lymphatics (lateral to medial, with the empty space of femoral canal medial to the vein).
Q3. What is Hunter's canal? What passes through it?
The adductor (subsartorial) canal in the medial thigh, bounded anteriorly by vastus medialis, posteriorly by adductor longus and magnus, medially by the sartorius (roof). Contents: Superficial femoral artery and vein, saphenous nerve, nerve to vastus medialis.
Q4. What is the adductor hiatus?
Opening in adductor magnus through which the SFA passes to become the popliteal artery, at the junction of the middle and lower thirds of the thigh.
Q5. Name the branches of the popliteal artery.
In order: Superior lateral genicular, superior medial genicular, middle genicular (to knee joint), inferior lateral genicular, inferior medial genicular, then terminal branches: anterior tibial (passes through interosseous membrane) and tibioperoneal trunk (which divides into posterior tibial and peroneal arteries).
Q6. What is the angiosome concept and its clinical relevance?
Taylor and Palmer (1987): Angiosomes are 3D vascular territories supplied by a named source artery. In CLTI, directing revascularization to the vessel supplying the ischemic territory (angiosome-directed revascularization) results in better wound healing compared to indirect revascularization. For example, a plantar heel ulcer is supplied by the calcaneal branch of the posterior tibial artery - so target the posterior tibial artery.
EXAMINATION VIVA
Q7. How do you perform Buerger's test? What does it demonstrate?
Elevate both lower limbs to 45° for 1-2 minutes; observe for pallor (positive if pallor appears at <45° elevation). Then lower legs to the dependent position; positive test shows reactive hyperaemia (dependent rubor - dusky red/purple colour). It demonstrates severe arterial insufficiency. Buerger's angle <20° = severe CLTI.
Q8. What is Buerger's angle?
The angle of elevation of the lower limb at which blanching/pallor first appears. Normal >45°. Severity: <20° = severe ischemia.
Q9. What is the significance of venous guttering?
On elevation of the ischemic limb, the superficial veins appear as guttered (collapsed) grooves under the skin. This indicates severe arterial insufficiency, where there is insufficient arterial inflow to maintain venous filling even at rest. Normal limbs maintain venous filling up to a significant angle of elevation.
Q10. How does Trendelenburg test differ in meaning between varicose veins and DVT?
In VARICOSE VEINS: Trendelenburg test identifies SFJ incompetence. In DVT: not the same test - for DVT we use clinical probability scoring (Wells) + D-dimer + compression duplex ultrasound.
Q11. What is a positive Perthes' test and what does it mean?
Positive = varicosities become more distended and painful on walking with tourniquet applied below knee. Indicates deep vein obstruction (patient is using superficial veins as a collateral). Do NOT strip or ligate the great saphenous vein in this patient - it is serving as the main drainage channel.
Q12. What is the significance of absence of dorsalis pedis pulse?
The dorsalis pedis is absent in 10% of normal individuals as an anatomical variant (replaced by a perforating branch of the peroneal artery). Do not conclude arterial disease from DP absence alone - always check the posterior tibial pulse as well. Both absent = significant tibial disease.
INVESTIGATION VIVA
Q13. What is ABI? How do you measure it?
Ankle-Brachial Index = Ankle systolic pressure / Highest brachial systolic pressure. Measured using cuff at ankle + hand-held continuous-wave Doppler. Normal: 0.9-1.3. <0.9 = PAD. <0.4 = CLTI.
Q14. Why is ABI falsely elevated in diabetics?
Medial artery calcification (Monckeberg sclerosis) makes the vessel wall non-compressible. The cuff cannot occlude a calcified vessel, so the measured ankle pressure is falsely high (sometimes >1.4), giving a falsely elevated ABI. Solution: Use toe-brachial index (TBI) - digital vessels are rarely calcified in diabetes.
Q15. What does a triphasic Doppler waveform indicate?
Normal arterial flow in a peripheral artery. The three components represent: (1) forward systolic flow, (2) brief reverse flow due to peripheral vascular resistance in diastole, and (3) forward diastolic flow. Loss of the reverse component (biphasic) and then loss of diastolic component (monophasic) indicate progressive PAD.
Q16. What is the Wells score for DVT?
Clinical prediction score; ≥2 = DVT likely. Key variables (+1 each): Active cancer, paralysis/immobilisation, bedridden >3 days or surgery in 12 weeks, localised tenderness along deep vein system, entire leg swelling, calf swelling >3 cm compared to contralateral, pitting oedema greater in symptomatic leg, collateral superficial veins, previous DVT. (-2): Alternative diagnosis at least as likely as DVT.
Q17. What is D-dimer? When is it useful and when is it NOT?
D-dimer is a fibrin degradation product elevated when any clot is forming/lysing anywhere in the body. It is highly sensitive but NOT specific. Use: RULE OUT DVT/PE in LOW probability patients (if negative D-dimer in low-probability patient = no further workup needed). NOT useful in: High-probability patients (always do duplex regardless), post-surgery, cancer, pregnancy, infection, inflammation (all elevate D-dimer).
CLASSIFICATION VIVA
Q18. What is the CEAP classification?
Clinical-Aetiological-Anatomical-Pathophysiological classification for chronic venous disorders. C0-C6 (clinical severity), E (primary/secondary/congenital), A (superficial/perforator/deep), P (reflux/obstruction/both).
Q19. What is the difference between Fontaine and Rutherford classifications?
Fontaine: Older, simpler, 4 stages (I-IV): asymptomatic, claudication, rest pain, tissue loss. Rutherford: More detailed, 7 categories (0-6): asymptomatic, mild/moderate/severe claudication, rest pain, minor tissue loss, major tissue loss. Rutherford is now preferred in research and clinical practice.
Q20. What is CLTI?
Chronic Limb-Threatening Ischemia - the current preferred term (SVS/ESVS Global Vascular Guidelines 2019) replacing "critical limb ischemia." Defined as >2 weeks of ischemic rest pain, ulceration, or gangrene with objective evidence of PAD. Encompasses Rutherford categories 4, 5, 6 / Fontaine stages III-IV.
Q21. Classify varicose veins.
CEAP classification is the standard. Clinically: (1) Primary (idiopathic SFJ incompetence); (2) Secondary (post-thrombotic, pregnancy, pelvic mass); (3) Recurrent (after previous treatment). By distribution: Great saphenous (medial), short saphenous (posterior), non-saphenous (uncommon).
MANAGEMENT VIVA
Q22. What is the first-line treatment for claudication?
Supervised exercise programme (30-45 min, 3×/week, ≥12 weeks) PLUS cardiovascular risk factor modification (smoking cessation, statin, antiplatelet, BP control, glycaemic control). Cilostazol 100 mg BD can be added for pharmacological benefit. Angioplasty is not first-line for claudication alone.
Q23. When do you operate for varicose veins?
Indications: (1) Symptomatic varicose veins (pain, heaviness, thrombophlebitis) after failed conservative measures; (2) Complications: active or healed venous ulcer, bleeding varicosities, superficial thrombophlebitis; (3) NICE guidelines: treat symptomatic C2+ before ulcer develops. Cosmetic indication alone is not an NHS indication.
Q24. Name the treatment options for varicose veins in order of evidence.
1. Endothermal ablation (EVLA/RFA): Gold standard, outpatient, local anaesthesia, highest quality-of-life evidence. 2. Ultrasound-guided foam sclerotherapy (UGFS): For residual tributaries, complex recurrence. 3. Surgical ligation + stripping: Still effective; general/spinal anaesthesia; now third-line (Bailey & Love 28e). 4. Compression sclerotherapy: For small veins/telangiectasias.
Q25. How do you manage acute DVT?
According to Bailey & Love 28e: Confirm diagnosis with duplex ultrasound ± D-dimer. Anticoagulation with LMWH (or DOAC directly in many guidelines). Then oral anticoagulation for ≥3 months (DOAC preferred: rivaroxaban/apixaban for DVT-PE). IVC filter if anticoagulation contraindicated. Thrombolysis/catheter-directed thrombolysis for massive ilio-femoral DVT to prevent post-thrombotic syndrome.
Q26. What is the conduit of choice for femoropopliteal bypass?
Autologous great saphenous vein (GSV) is the first choice, whether reversed or in-situ technique. 5-year patency 70-80% for below-knee bypass. PTFE is used for above-knee bypass when GSV is unavailable, with acceptable 5-year patency of 50-60%, but gives inferior results for below-knee anastomosis.
Q27. What is the indication for amputation in PAD?
Primary amputation: (1) Rutherford Category III ALI (irreversible ischemia - rigor, profound sensory/motor loss, absent venous Doppler), (2) Non-reconstructable disease (no distal runoff vessels), (3) Failed all revascularization attempts, (4) Extensive infection/sepsis with tissue destruction, (5) Non-ambulatory patient where revascularization risk exceeds benefit.
EMERGENCY VASCULAR VIVA
Q28. A patient presents with sudden cold, pale, pulseless, painful right leg. What do you do?
This is Acute Limb Ischemia (ALI). Management:
1. IV access, bloods (FBC, U&E, coagulation, X-match, glucose), ECG, CXR
2. Immediate IV heparin 5000-10000 IU bolus (prevents propagation)
3. Urgent vascular surgical assessment
4. Classify by Rutherford: Viable (I) → imaging then plan; Threatened (IIa/b) → urgent CTA then revascularization; Irreversible (III) → primary amputation
5. Determine cause: embolism (AF, cardiac source) or thrombosis (prior PAD)
6. Embolism → Fogarty embolectomy; Thrombosis → CDT or bypass
7. Fasciotomy if ischemia >4-6 hours
Q29. What is the "rule of six" for acute limb ischemia?
After 6 hours of complete ischemia: irreversible nerve and muscle damage occurs. Therefore revascularization should be performed within 4-6 hours to save the limb. Beyond 6 hours: increasing risk of reperfusion injury, compartment syndrome, and limb loss.
Q30. What is compartment syndrome? How do you diagnose and treat it?
Compartment syndrome = increased pressure within a closed fascial compartment → compromise of perfusion → ischemia of enclosed tissues. Diagnosis: Clinical (pain out of proportion, pain on passive stretch, tense compartment, paraesthesias) + compartment pressure measurement (>30 mmHg or within 20-30 mmHg of diastolic pressure). Treatment: Emergency four-compartment fasciotomy of leg (two-incision technique).
OPERATIVE VIVA
Q31. What are the complications of femoral artery cutdown?
Haemorrhage, thrombosis, false aneurysm, AV fistula, wound infection, lymphocele, lymphoedema (disruption of lymphatics at groin), femoral nerve injury, DVT.
Q32. What is the principle of the in-situ saphenous vein bypass?
The great saphenous vein is left in its normal anatomical bed (not harvested). The valves (which normally prevent downward flow) are destroyed using a valvulotome passed through the lumen. The tributaries are ligated (AV fistulas would otherwise form). The proximal anastomosis is to the common/superficial femoral artery, and distal anastomosis to the target artery. The advantage is that the vein tapers naturally to match the smaller distal artery, and the vasa vasorum remain intact.
Q33. What suture material do you use for vascular anastomosis?
Polypropylene (Prolene) monofilament non-absorbable sutures. Sizes: 3-0/4-0 for aortic anastomosis; 5-0 for femoral; 6-0 for popliteal and tibial; 7-0/8-0 for pedal bypass.
Q34. What is a patch angioplasty? When is it used?
Widening of the arteriotomy closure using a patch of autologous vein (GSV), bovine pericardium, or PTFE. Used to: (1) Close an arteriotomy without narrowing the lumen (femoral endarterectomy, embolectomy); (2) Carotid endarterectomy closure; (3) When direct closure would create stenosis.
IMAGE-BASED VIVA
Q35. What does this image show (telangiectasia)? What CEAP class is this?
[Image: Fine red/purple branching vessels under skin surface]
Telangiectasia - CEAP C1. These are dilated intradermal venules <1 mm diameter. Part of chronic venous disease spectrum. Treated by sclerotherapy or laser.
Q36. Describe the skin changes shown (lipodermatosclerosis)? What are the consequences?
[Image: Indurated, erythematous, woody lower leg]
Lipodermatosclerosis - CEAP C4b. Chronic inflammation and fibrosis of skin and subcutaneous tissues. The leg has an "inverted champagne bottle" or "inverted bowling pin" shape - upper oedema, woody lower leg. Consequences: (1) Ulceration (C5-C6), (2) Achilles tendon contracture, (3) Difficult wound healing.
Q37. This patient has a venous ulcer. What are the FOUR pillars of venous ulcer management?
1. Compression: Four-layer compression bandage or compression stockings (class 3, 25-35 mmHg) - the most important treatment
2. Debridement of slough (surgical, enzymatic, larval, autolytic)
3. Treat underlying venous incompetence (EVLA/RFA of incompetent truncal veins accelerates healing and reduces recurrence)
4. Wound care: appropriate dressings (hydrocolloid, foam, silver if infected)
DOPPLER VIVA
Q38. What is the difference between duplex and triplex ultrasound?
Duplex = B-mode (grey scale anatomical imaging) + colour/spectral Doppler (flow assessment). Triplex = Duplex + Power Doppler. Duplex is the standard vascular investigation term; "triplex" is a marketing term. Both provide the same information.
Q39. What finding on compression duplex confirms DVT?
The most sensitive and specific finding is non-compressibility of the vein. When the transducer compresses the vein, a normal vein collapses completely while a thrombosed vein is incompressible. Additionally: absent spontaneous flow, absent respiratory variation, absent augmentation with distal compression.
INSTRUMENT VIVA
Q40. Name this instrument and describe its use. (Fogarty catheter)
The Fogarty embolectomy catheter is a balloon-tipped catheter invented by Thomas Fogarty in 1963. It consists of a flexible catheter with an inflatable balloon at the tip. Technique: passed beyond the thrombus/embolus, balloon inflated, catheter withdrawn - balloon drags the clot out. Available in 2F (tibial) to 7F (aortic) sizes.
Q41. What is a Satinsky clamp used for?
A partial occlusion vascular clamp that allows side-clamping of a vessel to create an anastomosis while blood continues to flow through the main lumen. Essential for creating end-to-side anastomoses and for controlling bleeding from large vessels without complete occlusion.
Q42. Name instruments used in vascular surgery?
Bulldog clamps (DeBakey), Satinsky partial occlusion clamp, Potts angled scissors, DeBakey tissue forceps (non-crushing), Vessel loops (silicone), Fogarty catheters, Valvulotome (for in-situ bypass), Tunnelling device (for graft passage), Handheld 8 MHz Doppler probe, Pruitt-Inahara shunt (carotid endarterectomy), Hemoclips.
SECTION 15: IMAGE-BASED DISCUSSION
Images from Bailey & Love 28th Edition (Authentic Textbook Images)
Image Gallery with Clinical Teaching Points
1. Telangiectasia and Reticular Veins (CEAP C1)
Teaching: Fine, branching, red/purple vessels <1mm (telangiectasia) and blue reticular veins (1-3mm). First sign of chronic venous disease. Treated with sclerotherapy/laser.
2. Advanced Skin Changes - Lipodermatosclerosis + Eczema + Atrophie Blanche (CEAP C4b)
Teaching: The "inverted champagne bottle" lower leg. Red-brown discolouration from haemosiderosis. White patches = atrophie blanche (areas of avascular scar). Painful. Pre-ulcerative. Treat underlying venous hypertension urgently.
3. Haemosiderosis (CEAP C4a) - Bilateral Comparison
Teaching: Dark brownish pigmentation of the gaiter zone from haemosiderin deposition (breakdown of RBCs extravasated through capillaries under venous hypertension). Compare affected vs normal limb.
4. Active Venous Ulcer (CEAP C6)
Teaching: Classic gaiter-zone venous ulcer. Irregular sloping margins. Sloughy, moist base. Surrounding haemosiderosis and LDS. Over incompetent medial perforators. Management: compression + wound care + treat venous reflux.
5. Chronic Venous Insufficiency with Pigmentation (CEAP C4a/5)
Teaching: Advanced post-thrombotic changes with bilateral lower limb discolouration and haemosiderosis. Note the gaiter-zone distribution. The normal contralateral limb shows the stark contrast.
SECTION 16: FLOWCHARTS
Flowchart 1: Approach to Lower Limb Ischaemia
PATIENT WITH LOWER LIMB ISCHAEMIA
│
┌──────────┴──────────┐
ACUTE (<2 wks) CHRONIC (>2 wks)
│ │
6 Ps present Claudication / Rest pain /
(Pain, Pale, Tissue loss / Ulcer
Pulseless, │
Paralysis, ABI Measurement
Paresthesia, │
Poikilothermia) ┌─────┴──────┐
│ ABI ABI
│ ≤0.9 >1.3
│ (PAD) (Calcified)
│ │ │
│ Risk factor Toe-Brachial
Rutherford modification Index (TBI)
Classification │
│ Asymptomatic Symptomatic PAD
│ │ │
│ Observe & ┌────┴────┐
Cat I: CTA treat risks Claudication CLTI
then plan │ │
Cat IIa: CDT Exercise + Duplex +
Cilostazol CTA/MRA →
Cat IIb: ± PTA if Revascularization
Urgent TASC A-B planning
revascularize
Cat III:
Primary
amputation
Flowchart 2: DVT Diagnosis and Management (Bailey & Love / NICE)
SUSPECTED DVT
│
Calculate Two-Level Wells Score
│
┌───┴───┐
≥2 <2
(Likely) (Unlikely)
│ │
Duplex D-Dimer
Ultrasound │
│ ┌──┴──┐
Positive Neg Pos
│ │ │
Treat No DVT Duplex US
│ │
DOAC ×3m Positive → Treat
(rivaroxaban Negative → No DVT
/apixaban)
│
LMWH bridge
if cancer
Flowchart 3: Varicose Vein Management (NICE CG168)
VARICOSE VEINS
│
Clinical Assessment + CEAP
│
Asymptomatic C2 Symptomatic C2+ Complications
(Cosmetic only) (ulcer, bleed, SVT)
│ │ │
Conservative Duplex US PRIORITY
(compression) Mapping referral
│
┌─────────┼─────────┐
EVLA/RFA UGFS Surgery (3rd line)
(1st line) (2nd) Ligation + stripping
│
Perforator disease?
│
Ultrasound-guided
perforator ablation
Flowchart 4: Revascularization Strategy for PAD
SYMPTOMATIC PAD - REVASCULARIZATION DECISION
│
Duplex/CTA Anatomy
│
┌────────┴────────┐
TASC A/B TASC C/D
(focal disease) (diffuse disease)
│ │
Endovascular Open Surgery
First Preferred
│ │
PTA ± stent Aortoiliac: Aortobifemoral bypass
± DCB Fem-Popliteal: Bypass with GSV
Femoro-tibial: GSV bypass
Profundaplasty
│
Failed endo
│
Open Surgery
SECTION 17: MIND MAPS
Mind Map 1: Acute Limb Ischemia
ACUTE LIMB ISCHEMIA
│
┌──────────────┼──────────────┐
CAUSES 6 Ps CLASSIFY
│ │ (Rutherford)
Embolism (50%) Pain │
Thrombosis (40%) Pallor I-Viable
Trauma (5%) Pulseless IIa-Marginally
Iatrogenic (5%) Paralysis IIb-Immediately
│ Paresthesia III-Irreversible
│ Poikilothermia
│
EMBOLISM vs THROMBOSIS
(see comparison table)
│
MANAGEMENT
│
┌────┴────┐
Medical Surgical
Heparin Fogarty / CDT /
IV Bypass / Amputation
Mind Map 2: Varicose Veins (SMARTER)
VARICOSE VEINS
│
┌─────────────┼─────────────┐
ANATOMY CLINICAL TREATMENT
│ │ │
SFJ/SPJ CEAP EVLA/RFA
Perforators C0-C6 UGFS
Great/Small E,A,P Surgery
Saphenous Classification Sclerotherapy
│
TESTS
│
Trendelenburg
Perthes
Schwartz
Fegan
Doppler duplex
Mind Map 3: PAD Risk Factors (HEADS)
H - Hypertension
E - Everything lipid (dyslipidaemia)
A - Atherosclerosis / Age / Arrhythmia (AF)
D - Diabetes Mellitus
S - Smoking (most important modifiable risk factor)
Additional:
C - CKD
O - Obesity
F - Family history
H - Hyperhomocysteinaemia
SECTION 18: HIGH-YIELD MS/DNB PEARLS
Commonly Asked Long-Case Questions (MS/DNB India)
- "Present the case." - Practise the 5-minute presentation format; include all risk factors
- "What is your working diagnosis?" - Commit to a specific diagnosis with Fontaine/Rutherford stage
- "How will you investigate this patient?" - Start with bedside (ABI), then duplex, then CTA
- "What is your management plan?" - Medical first, then revascularization; MDT approach
- "Why is vein graft preferred over PTFE?" - Patency, resistance to infection, size matching
Examiner's Favourite Cross-Questions
- "What is the ABI? How does diabetes affect it?"
- "Classify this patient's varicose veins using CEAP."
- "What is Leriche syndrome?"
- "What is the first-line treatment for claudication?" (Exercise - not surgery!)
- "Why does this patient have rest pain worse at night?"
- "What is Buerger's disease? How does it differ from atherosclerotic PAD?"
- "Name the complications of DVT."
- "What is post-thrombotic syndrome? How do you prevent it?"
Common Candidate Mistakes
| Mistake | Correct Approach |
|---|
| Saying "varicose veins are dilated veins" only | CEAP classify; discuss SFJ, duplex, treatment |
| Examining pulses in wrong position | Femoral supine; popliteal semi-flexed; DP with relaxed foot |
| Missing contralateral limb examination | Always examine BOTH limbs |
| Not classifying ALI (Rutherford) | Always state category - determines management |
| Not checking for AF when asked cause of ALI | AF is the most common source of peripheral embolism |
| Recommending immediate surgery for claudication | Medical + exercise therapy first |
| Listing "heparin" as treatment for acute limb ischemia without specifying route/dose | IV unfractionated heparin 5000-10000 IU bolus immediately |
| Not mentioning fasciotomy after embolectomy | Always consider fasciotomy for ischemia >4-6 hours |
Buerger's Disease (TAO) - High Yield Points
- Thromboangiitis obliterans (Buerger's disease): Inflammatory segmental occlusion of small/medium arteries and veins in young smokers
- Classic triad: Young male (<45 yrs), heavy smoker, distal limb ischemia (hands AND feet involved)
- Diagnostic criteria (Shionoya): Onset <50 yrs, tobacco use history, infrapopliteal occlusive disease, upper limb involvement or phlebitis migrans, no atherosclerotic risk factors except smoking
- Angiography: "Corkscrew" collaterals; tapering segmental occlusions of distal vessels
- Treatment: The ONLY effective treatment is COMPLETE AND PERMANENT smoking cessation. No bypass (small vessels; no good runoff). Prostaglandins (iloprost) for pain relief. Amputation if gangrene develops.
- Key difference from atherosclerosis: Young age, involves upper limbs, superficial phlebitis migrans, no diabetes/hypertension/dyslipidaemia, completely different angiographic appearance
Mnemonics
6 Ps of Acute Limb Ischemia:
Pain, Pallor, Pulselessness, Paresthesia, Paralysis, Poikilothermia (coolness)
Contents of Femoral Triangle (lateral to medial):
NAVY: Nerve, Artery, Vein, Y-fronts (lymphatics/empty space)
Fontaine Stages:
Innocent (asymptomatic), IIt hurts when I Walk, III = Rest pain, IV = Tissue loss (IV = dead tissue)
CEAP Clinical Classes:
Can We Visit Old Patients Here Under Skies - C0(can) W(we) V(visit) O(old) P(patients) H(here) U(under) S(skies) - C0=no signs, C1=telangiectasia, C2=varicosities, C3=oedema, C4=skin changes, C5=healed ulcer, C6=active ulcer
Embolism vs Thrombosis:
Embolism = Emergency (sudden onset, NO prior symptoms, cardiac source, Fogarty)
Thrombosis = Thick background (pre-existing PAD, slower onset, requires bypass)
SECTION 19: FINAL RAPID REVISION
One-Page Rapid Revision Sheet
╔══════════════════════════════════════════════════════════════════╗
║ LOWER LIMB PVD - RAPID REVISION ║
╠══════════════════════════════════════════════════════════════════╣
║ PULSE SITES ║
║ Femoral: Midpoint inguinal ligament ║
║ Popliteal: Midline fossa, knee semi-flexed ║
║ Post tibial: Behind medial malleolus ║
║ Dorsalis pedis: Between EHL and EDL tendons ║
╠══════════════════════════════════════════════════════════════════╣
║ ABI VALUES ║
║ >1.3=calcified, 0.9-1.3=normal, 0.7-0.9=mild, 0.5-0.7=moderate ║
║ 0.3-0.5=severe PAD, <0.3=CLTI ║
╠══════════════════════════════════════════════════════════════════╣
║ RUTHERFORD ALI: I=viable, IIa=marginal, IIb=immediate, III=dead ║
║ FONTAINE: I=asymp, II=claud, III=rest pain, IV=tissue loss ║
╠══════════════════════════════════════════════════════════════════╣
║ CEAP: C0=none, C1=telang, C2=varix, C3=oedema, ║
║ C4=skin, C5=healed ulcer, C6=active ulcer ║
╠══════════════════════════════════════════════════════════════════╣
║ EMBOLISM vs THROMBOSIS ║
║ Embolism: Sudden, no PAD history, AF source, Fogarty ║
║ Thrombosis: Gradual, prior claudication, bypass/CDT ║
╠══════════════════════════════════════════════════════════════════╣
║ TREATMENT HIERARCHY ║
║ Claudication: Exercise > Cilostazol > PTA (TASC A/B) ║
║ CLTI: Risk factor control + Revascularization (endo or open) ║
║ ALI: Heparin → Fogarty/CDT → Fasciotomy ║
║ DVT: DOAC ≥3 months (LMWH → oral) ║
║ VV: EVLA/RFA > UGFS > Surgery ║
╠══════════════════════════════════════════════════════════════════╣
║ GRAFT CHOICE: GSV >> PTFE (especially below-knee) ║
║ FOGARTY: 2F=tibial, 3F=popliteal, 4F=SFA, 5F=iliac ║
╚══════════════════════════════════════════════════════════════════╝
Top 50 Viva Questions (Final Revision)
- Where is the femoral pulse palpated?
- What are the contents of the femoral triangle?
- What is Hunter's canal?
- What is the angiosome concept?
- Name the branches of the popliteal artery.
- What are the 6 Ps of ALI?
- Classify ALI using Rutherford.
- Differentiate embolism from thrombosis.
- What is Leriche syndrome?
- What is the ABI? Normal values?
- Why is ABI falsely elevated in diabetics?
- What is TBI? When used?
- Describe Buerger's test.
- What is Buerger's angle?
- What is the CEAP classification?
- What is Fontaine classification?
- What is CLTI?
- Describe Trendelenburg test.
- What is Perthes' test? Significance?
- What is Stemmer's sign?
- Compare arterial vs venous vs neuropathic ulcer.
- What is venous guttering?
- What is dependent rubor?
- What is lipodermatosclerosis?
- What is atrophie blanche?
- What is a saphena varix?
- What are Cockett perforators?
- First-line treatment for claudication?
- What is cilostazol? Contraindications?
- Graft of choice for femoropopliteal bypass?
- In-situ vs reversed vein bypass?
- What is fasciotomy? Indications?
- Compartment syndrome - diagnosis?
- Fogarty catheter - describe and sizes?
- What is a patch angioplasty?
- When to amputate vs revascularize?
- BKA vs AKA - which is preferred?
- What is DVT Wells score?
- Treatment of acute DVT?
- What is post-thrombotic syndrome?
- What is the Villalta score?
- What is Buerger's disease (TAO)?
- How to treat Buerger's disease?
- What is a popliteal aneurysm? Complications?
- What is aortoenteric fistula?
- What sutures in vascular anastomosis?
- What is TASC classification?
- What is CDT? Contraindications?
- What is reperfusion injury?
- What is DCB (drug-coated balloon)?
Top 20 One-Liners
- Femoral pulse: Midpoint of inguinal ligament (NOT mid-inguinal point)
- Most common peripheral arterial aneurysm: Popliteal artery aneurysm
- Most common cause of peripheral arterial embolism: Atrial fibrillation
- Gold standard first-line investigation: Duplex Doppler ultrasound
- ABI falsely elevated because: Medial calcinosis (Monckeberg sclerosis) in diabetics
- First-line treatment for claudication: Supervised exercise programme
- Graft of choice below knee: Autologous great saphenous vein
- Fogarty catheter 2F: Tibial vessels; 4F: SFA; 5F: Iliac
- Fasciotomy indication: Compartment pressure >30 mmHg or within 20-30 of diastolic
- Category III ALI: Primary amputation (do NOT revascularize)
- Buerger's disease treatment: Complete and permanent smoking cessation
- CEAP C6: Active venous ulcer
- Most important finding on duplex for DVT: Non-compressibility of vein
- Positive Perthes' test: Do NOT strip the saphenous vein (it is the collateral)
- Angiosome concept: Direct revascularization to vessel supplying the ischemic territory
- Wells score ≥2: DVT likely - proceed to duplex
- D-dimer: Highly sensitive, not specific; useful to RULE OUT in low probability
- Leriche syndrome: Aortoiliac occlusion = buttock claudication + impotence + absent femoral pulses
- Stemmer's sign positive: Cannot pinch skin at base of 2nd toe = lymphoedema
- CLTI criteria (ABI): Resting ankle pressure <50 mmHg or ABI <0.4
Top 10 Examiner Traps
| Trap | Correct Answer |
|---|
| 1. "Where is the femoral pulse?" | Midpoint of inguinal ligament, NOT mid-inguinal point |
| 2. "Is dorsalis pedis absent = arterial disease?" | Absent in 10% normal population; always check PT pulse too |
| 3. "First-line for claudication = surgery/angioplasty?" | NO - Exercise programme is first-line (Class IA) |
| 4. "Homan's sign is reliable for DVT?" | NO - sensitivity 50%, specificity 40%; unreliable; use Wells + duplex |
| 5. "Revascularize ALI Category III?" | NO - Primary amputation; revascularization causes lethal reperfusion |
| 6. "PTFE graft is as good as vein below knee?" | NO - GSV vein is significantly superior for below-knee bypass |
| 7. "Buerger's disease is treated by bypass?" | NO - Only treatment is complete smoking cessation; bypass often impossible |
| 8. "ABI >1.3 = normal?" | NO - Non-compressible vessels (calcified); use TBI instead |
| 9. "Strip saphenous vein in positive Perthes' test?" | NEVER - it is the main drainage channel when deep veins are obstructed |
| 10. "DVT = warfarin for life?" | NO - 3 months for provoked DVT; 6 months-indefinite for unprovoked/cancer DVT; DOACs preferred |
Top 10 Vascular Examination Pearls
- Always examine standing AND lying - varicosities only visible standing
- Always examine BOTH limbs - contralateral PAD is common
- Temperature assessment with dorsum of hand - more sensitive than palm
- Grade ALL pulses 0-3 - do not just say "present/absent"
- Auscultate over femoral and popliteal arteries for bruits (indicate stenosis)
- Always auscultate aorta for aortic bruit (aortoiliac disease)
- Prominent popliteal pulse = aneurysm until proven otherwise
- Buerger's test every time in arterial case - gives Buerger's angle
- Neurological exam in all diabetic patients - neuropathy modifies presentation
- Capillary refill time >5 sec in toes = severe ischemia
Top 10 Operative Pearls
- GSV is the first choice for all below-knee bypass grafting
- Always send biopsy from amputated limb if unusual (malignancy?)
- Heparin before clamping - prevents distal propagation of thrombus
- Always do completion angiogram or Doppler after embolectomy
- Prophylactic fasciotomy if ischemia >4-6 hours before reperfusion
- Cover prosthetic graft with retroperitoneum - prevents aortoenteric fistula
- Patch closure of arteriotomy - prevents stenosis
- Saphenous nerve runs with GSV - gentle retraction avoids injury
- Vertical skin incision at groin (parallel to femoral vessels); not transverse
- BKA stump length 12-15 cm below tibial tuberosity for best prosthetic fit
Sources: Bailey & Love's Short Practice of Surgery 28th Edition (Norman Williams, Christopher Bulstrode, Ronan O'Connell), Sabiston Textbook of Surgery (Townsend et al.), Sabiston Chapter 103/104 on PAD and Amputation, Goldman-Cecil Medicine, Harrison's Principles 22e, Gray's Anatomy for Students, SVS/ESVS Global Vascular Guidelines 2019, AHA/ACC PAD Guidelines 2016/2024 update, NICE CG168 (Varicose Veins), NICE NG158 (Peripheral Arterial Disease).
A note from your examiner: The mark of a great vascular long-case presentation is not just knowing the facts, but demonstrating clinical reasoning - WHY this patient has this condition, WHAT the examination findings tell you about the level and severity of disease, and HOW you would make a rational management decision. Always start with the bedside, work your way to imaging, and present a patient-centred management plan. Good luck.