Colorectal polyps in details from scratch to pro level from standard books
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Searching PubMed
colorectal polyp surveillance guidelines management
I now have thorough, high-quality data from multiple standard textbooks (Schwartz, Sleisenger & Fordtran, Yamada, Bailey & Love, Robbins & Kumar, Current Surgical Therapy) plus recent guidelines. Let me compile the comprehensive answer.
Colorectal Polyps: From Scratch to Pro Level
Sources: Schwartz's Principles of Surgery (11e), Sleisenger & Fordtran's GI and Liver Disease, Yamada's Textbook of Gastroenterology (7e), Bailey & Love's Short Practice of Surgery (28e), Robbins & Kumar Basic Pathology, Robbins Cotran & Kumar Pathologic Basis of Disease, Current Surgical Therapy (14e)
1. Definition and Basic Concept
A polyp is a nonspecific clinical term describing any projection from the surface of the intestinal mucosa, regardless of histologic nature. The term is purely morphological - it says nothing about pathology. Most colorectal polyps are asymptomatic and are discovered incidentally during colonoscopy or imaging. Their clinical importance is entirely determined by histopathology, which governs cancer risk, treatment, and surveillance intervals.
- Approximately 90% of polyps detected at colonoscopy are mucosal in origin
- Of mucosal polyps, ~75% are adenomas
- 20-53% of average-risk persons over age 50 harbor at least one adenoma
2. Classification
The most practical classification divides polyps into mucosal and submucosal types, with mucosal polyps being overwhelmingly more common and clinically significant:
TABLE: Classification of Colorectal Polyps (from Yamada's Textbook of Gastroenterology)
| Mucosal Polyps | Submucosal Polyps |
|---|---|
| Adenomatous (tubular, villous, tubulovillous) | Lipoma |
| Serrated: Hyperplastic (microvesicular, goblet cell, mucin-depleted), SSA/P, TSA | Carcinoid tumor (NET) |
| Hamartomatous: Juvenile, Peutz-Jeghers | GIST |
| Inflammatory/pseudopolyps | Colitis cystica profunda, pneumatosis, hemangioma, neurofibroma |
| Malignant polyp | Metastatic melanoma |
By malignant potential (Bailey & Love):
| Category | Type | Malignant Potential |
|---|---|---|
| Inflammatory | Pseudopolyps (IBD) | None |
| Hamartomatous | Peutz-Jeghers, Juvenile | Low to moderate |
| Serrated lesions | Hyperplastic, SSL, TSA | Variable |
| Adenoma | Tubular, tubulovillous, villous | Yes - increases with villous component |
| Malignant | Adenocarcinoma | Already malignant |
3. Morphology: Pedunculated vs. Sessile
Polyps are morphologically described by their attachment to the colonic wall:
- Pedunculated: attached by a vascular stalk; most amenable to snare polypectomy
- Sessile: flat or broad-based; no stalk; greater technical challenge for resection
- Flat/depressed lesions: especially dangerous - sessile and depressed lesions have MORE malignant potential than pedunculated lesions of equivalent size
The Paris classification is used endoscopically: type Ip (pedunculated), Is (sessile), IIa (slightly elevated), IIb (flat), IIc (slightly depressed), and III (excavated).
4. Adenomatous Polyps (Conventional Adenomas)
4.1 Epidemiology
- Most common polyp with malignant potential, representing 50-65% of all colonic polyps
- Found in up to 25% of persons over 50 in the US (Schwartz)
- Autopsy studies: nearly 50% of subjects had at least one adenoma
- Men have ~1.5x higher risk than age-matched women
- Prevalence rises steeply with age: ~1-5% in 30-39 years, 16% in 50-59 years, 25% by age 70-79
4.2 Histologic Types
Tubular Adenoma (TA):
- Most common: 65-85% of all adenomas (Current Surgical Therapy); 80-86% in Sleisenger
- Complex network of tubular, branching glands
- Glands do not extend beyond the muscularis mucosae
- Small, usually <1 cm; mild dysplasia predominates
- Risk of malignancy: ~5%
Villous Adenoma:
- 3-16% of all adenomas
- Long, finger-like projections (villi) extending from the stroma to the surface
- Large, often sessile; secretory - can cause watery diarrhea with electrolyte imbalance (McKittrick-Wheelock syndrome in extreme cases)
- Risk of malignancy: up to 40%
- ~60% of polyps >2 cm are villous
Tubulovillous Adenoma (TVA):
- 8-16% of adenomas; mixture of both patterns
- Risk of malignancy: ~22% (Schwartz)
- A polyp is classified as tubular if ≥80% tubular glands, villous if ≥80% villiform
Key sizing rule: A polyp is classified by its predominant architecture. Pure villous is rare in practice.
| Size | Predominant Type | % with HGD/Cancer |
|---|---|---|
| 1-5 mm | 99.1% TA | Very low (<0.1%) |
| 6-9 mm | 97% TA | Low |
| 10-19 mm | 86.8% TA, 11.3% TVA | Moderate |
| 20-50 mm | 62.5% TA, 29.4% TVA | High |
(Sleisenger, Table 126.1)
4.3 Dysplasia
By definition, all adenomas are dysplastic. Dysplasia is graded as:
- Low-grade dysplasia (LGD): Nuclei basally located, hyperchromatic, slightly enlarged but uniform. Glands show branching and budding. Goblet cell mucin loss begins.
- High-grade dysplasia (HGD): (= former "severe dysplasia" / "carcinoma in situ") - Nuclear stratification, pleomorphism, prominent nucleoli, extreme glandular crowding, complete loss of goblet mucin. No metastatic potential as long as muscularis mucosae is intact.
4.4 Histology Images
Below: Histological appearance of adenomas (Yamada's Textbook of Gastroenterology):
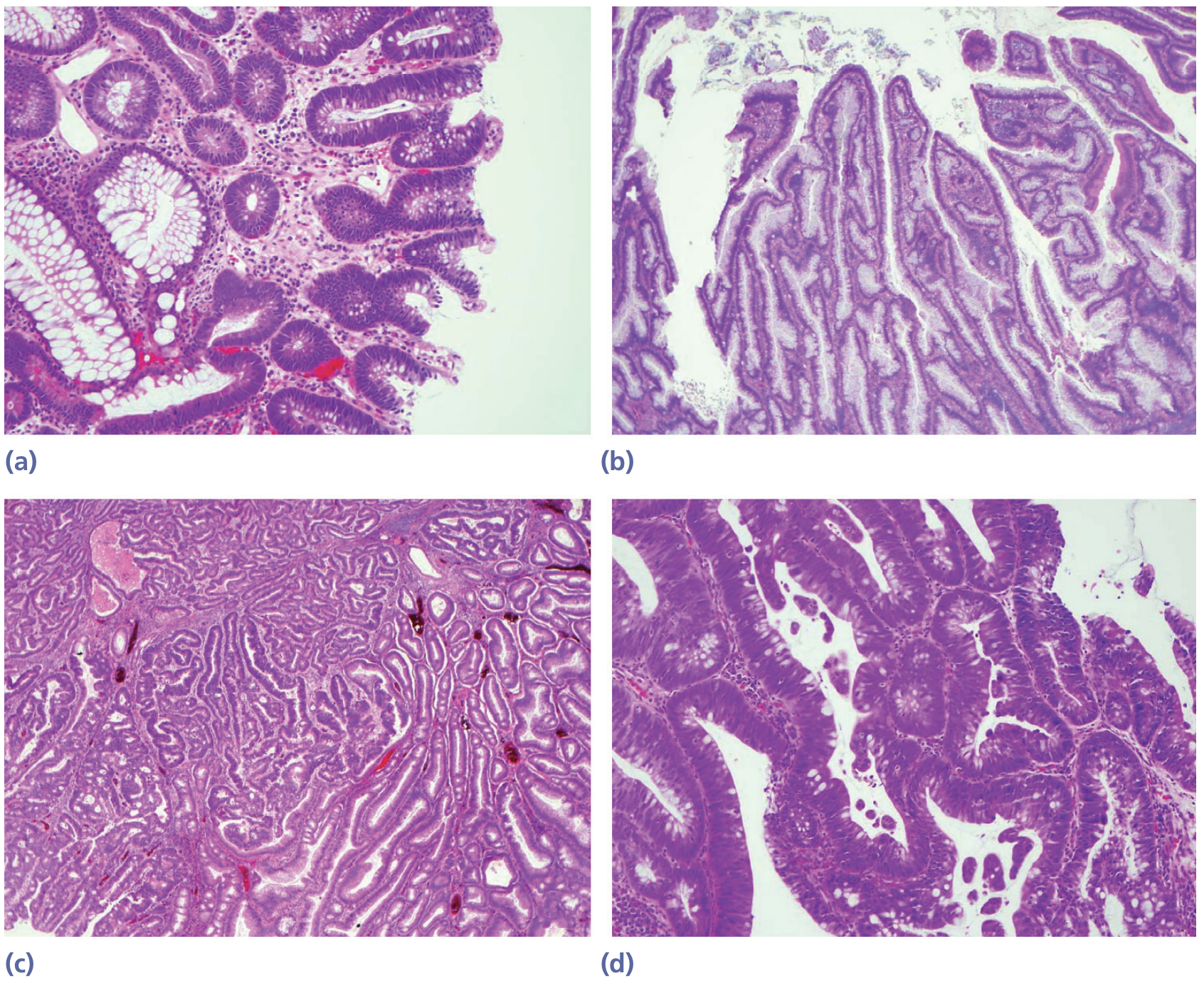
Fig. Histology of adenomatous polyps: (a) tubular adenoma, (b) villous adenoma, (c) tubulovillous, (d) high-grade dysplasia
Below: Gross and microscopic appearance (Robbins Pathology):
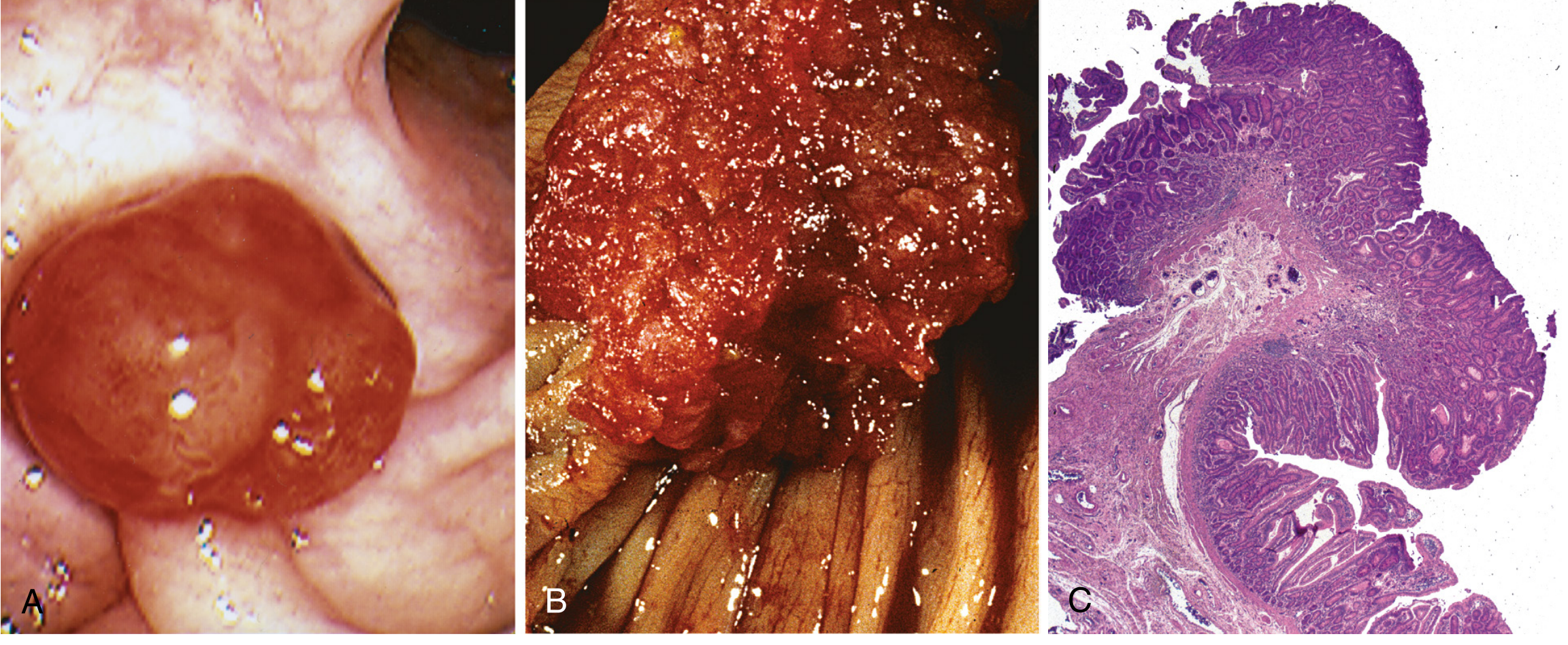
Fig. Colonic adenomas: (A) endoscopic view of pedunculated adenoma, (B) villous adenoma gross specimen, (C) histology of tubular adenoma
5. The Adenoma-Carcinoma Sequence
The central concept of colorectal oncology: the majority of colorectal carcinomas evolve from adenomatous polyps.
5.1 Molecular Pathways
1. Chromosomal Instability (CIN) Pathway - the "Loss of Heterozygosity" pathway (~70-80% of CRC):
- Normal mucosa → hyperproliferative epithelium → early adenoma → intermediate adenoma → late adenoma → carcinoma
- Key mutations: APC loss (early) → KRAS mutation → SMAD4 loss → TP53 loss (late)
- Predominates in left-sided, non-mucinous CRC
2. Microsatellite Instability (MSI) / Mismatch Repair (MMR) Pathway (~15% sporadic CRC):
- Defects in MMR genes (MLH1, MSH2, MSH6, PMS2)
- Accumulation of mutations in microsatellite regions at rates up to 1000x normal
- Right-sided predominance; mucinous histology; better prognosis
- Underlies Lynch syndrome (HNPCC) and ~10-15% sporadic CRC (via MLH1 methylation)
3. Serrated Pathway (~20-35% of CRC):
- BRAF mutation → KRAS mutation → CpG island methylator phenotype (CIMP) → MLH1 silencing by promoter methylation → carcinoma
- Sessile serrated lesions (SSLs) are the key precursor
- Right-sided; microsatellite unstable; mucinous
(Robbins Cotran & Kumar, Table 17.10)
5.2 Timeline
- Mean age difference between adenoma and cancer: ~4-5 years for sporadic lesions
- Average dwell time from mild dysplasia to cancer: ~8 years; severe dysplasia to cancer: ~3.6 years
- Over a 10-year period, the risk that an adenoma-bearing person develops CRC is only ~2.5% (Sleisenger) - but this risk is dramatically higher for large or villous lesions
6. Serrated Polyps
This group has become increasingly important as a distinct carcinogenesis pathway.
6.1 Hyperplastic Polyps (HP)
- Most common serrated polyp (~75% of serrated lesions)
- Usually small (<5 mm), located in the rectosigmoid
- Serrated architecture limited to the upper crypt only; glands taper near base
- Prominent neuroendocrine cells; thickened collagen table
- Three subtypes: Microvesicular (most common), goblet cell-rich, mucin-poor (no clinical significance to subtype in daily practice)
- Traditionally benign with no malignant potential
- Exception: large HPs (>1 cm), right-sided location, >20 HPs, or family history of CRC - these carry elevated risk
6.2 Sessile Serrated Lesion (SSL) / Sessile Serrated Adenoma (SSA)
- Also called SSA/P (sessile serrated adenoma/polyp); 2019 WHO recommends "SSL"
- ~9% of all colonic polyps; 15-25% of serrated polyps (Yamada)
- Predominantly right colon - broad-based, may reach several cm, subtle endoscopic appearance (color similar to adjacent mucosa, may look like a thickened fold)
- Histology: serrated architecture extending to the deep crypts, papillary invaginations, dilated and horizontally oriented crypt bases (L-shaped or boot-shaped crypts), few neuroendocrine cells, thin collagen table
- Key molecular events: BRAF mutation → CIMP → MLH1 methylation → CRC
- Loss of MLH1 occurs at the point of cytologic dysplasia; aberrant nuclear β-catenin labeling in SSLs with acquired conventional dysplasia
- SSLs are precursors to microsatellite unstable (MSI-H) right-sided CRC
6.3 Traditional Serrated Adenoma (TSA)
- Rare (~1% of serrated lesions)
- Predominantly distal colon
- Histology: complex villiform architecture, ectopic crypts with narrow slits, prominent eosinophilic cytoplasm, pencillate (pencil-shaped) nuclei - the defining feature
- Crypts lose their orientation to the muscularis mucosae
- Associated with KRAS or BRAF mutation
6.4 Serrated Polyposis Syndrome (SPS) / Serrated Polyposis
WHO 2019 criteria (updated - at least one of):
- ≥20 serrated polyps (any size) spread throughout the colon, OR
- ≥5 serrated polyps proximal to the sigmoid, with ≥2 measuring >10 mm, OR
- Any number of serrated polyps with a first-degree relative with SPS
CRC risk: 30-50% (Current Surgical Therapy)
7. Hamartomatous Polyps
7.1 Juvenile Polyps
- Most common polyp type in children (but can occur at any age)
- Gross: round, smooth, stalk-bearing, often ulcerated and mucus-filled ("retention cyst")
- Histology: dilated mucous glands in an edematous, inflammatory stroma - the hallmark
- Individual juvenile polyps are not premalignant
- Presentation: rectal bleeding, prolapse, intussusception
Juvenile Polyposis Syndrome (JPS):
- Autosomal dominant; mutations in SMAD4 (50%) or BMPR1A
- Diagnostic criteria: >5 juvenile polyps in colorectum, OR juvenile polyps throughout GI tract, OR any juvenile polyps + family history
- CRC risk: 40% - these lesions CAN degenerate into adenomas and carcinoma
- Screening: start age 10-12 years; annual colonoscopy
- Surgery: total abdominal colectomy + IRA, or proctocolectomy + IPAA if rectum heavily involved
7.2 Peutz-Jeghers Syndrome (PJS)
- Autosomal dominant; LKB1 (STK11) gene mutation
- Hallmarks: GI polyposis (predominantly small intestine > colon) + mucocutaneous melanin pigmentation (lips, buccal mucosa, perioral, hands, feet)
- Histology: arborizing smooth muscle core (branching "arborizing" fronds) covered by normal epithelium - the muscle is the hamartoma
- Complications: intussusception (bowel obstruction), bleeding
- CRC risk: 30-40%
- Extraintestinal malignancies: breast, pancreas, ovary (sex cord tumors with annular tubules), cervix (adenoma malignum), testicle (Sertoli cell tumor)
- Surveillance: baseline colonoscopy + upper endoscopy at age 20 years, then annual flexible sigmoidoscopy
7.3 Cowden Syndrome (PTEN Hamartoma Syndrome)
- Autosomal dominant; PTEN mutation
- Hamartomas of all three embryonal cell layers
- Features: facial trichilemmomas, breast cancer risk, thyroid disease (Lhermitte-Duclos disease of cerebellum), GI polyps
- Bannayan-Riley-Ruvalcaba syndrome is allelic (PTEN)
7.4 Cronkhite-Canada Syndrome
- Non-inherited (sporadic)
- Diffuse GI polyposis (entire tract) + alopecia + nail atrophy/onycholysis + cutaneous hyperpigmentation
- Protein-losing enteropathy, malabsorption, diarrhea, hypogeusia
- High mortality; surgery only for complications
8. Inflammatory Polyps (Pseudopolyps)
- Occur most commonly in inflammatory bowel disease (ulcerative colitis, Crohn's disease)
- Represent islands of residual normal/regenerating mucosa surrounded by denuded areas
- Also seen after amoebic colitis, schistosomiasis
- No malignant potential of the polyp itself
- The underlying chronic inflammation (not the polyp) confers CRC risk in IBD
9. Malignant Polyp
9.1 Definition
A malignant polyp = an adenoma in which a focus of carcinoma has invaded beyond the muscularis mucosae into the submucosa (pT1). This is NOT the same as HGD or intramucosal carcinoma (both carry zero metastatic potential).
Up to 5% of adenomatous polyps harbor a focus of carcinoma; higher in larger, villous, and dysplastic lesions.
9.2 Haggitt Classification (Pedunculated Polyps)
| Level | Definition | LN Metastasis Risk |
|---|---|---|
| 0 | Carcinoma in situ / intramucosal carcinoma | 0% |
| 1 | Submucosa, confined to the head | ~3% |
| 2 | Invasion into the neck of the polyp | ~3% |
| 3 | Invasion into the stalk | ~3% |
| 4 | Invasion of submucosa of the bowel wall below the stalk | Up to 25% |
Haggitt levels 1-3 correspond to Sm1; Haggitt 4 corresponds to Sm1, Sm2, or Sm3.
9.3 Kikuchi Classification (Sessile Polyps)
| Level | Definition | LN Metastasis Risk |
|---|---|---|
| Sm1 | Upper third of submucosa | 3% |
| Sm2 | Middle third | 8% |
| Sm3 | Lower third | 23% |
9.4 Favorable vs. Unfavorable Features (Sleisenger, Table 126.5)
| Feature | Favorable | Unfavorable |
|---|---|---|
| Differentiation | High or moderate | Poor |
| Vascular/lymphatic invasion | Absent | Present |
| Polypectomy margin | Clear (>2 mm) | Involved |
| Invasion of bowel wall submucosa | Absent | Present |
- All favorable features present: Endoscopic polypectomy is curative. No further surgery needed.
- One or more unfavorable features: Adverse outcome risk 10-25% (up to 45-50% with multiple unfavorable features); surgical resection is generally indicated.
10. Polyposis Syndromes
10.1 Familial Adenomatous Polyposis (FAP)
Genetics: Autosomal dominant. Germline mutation of APC gene (chromosome 5q21), a key negative regulator of the Wnt signaling pathway. ~75% inherited; ~25% de novo. Most mutations between codons 168-1640, with hotspots at codons 1061 and 1309.
Clinical Features:
- Classic FAP: >100 synchronous colorectal adenomas (can be thousands); polyps in rectum and left colon
- Polyps develop in adolescence; 15% of patients by age 10, 75% by age 20
- Without treatment: 100% CRC risk by age 35-40 (Robbins) / nearly always by age 50
- FAP is at least histologically indistinguishable from sporadic adenomas, though flat/depressed adenomas and microscopic adenomas (1-2 dysplastic crypts) are also prevalent
Extracolonic Manifestations (Bailey & Love Summary Box 77.2):
Endodermal:
- Duodenal/periampullary adenomas (>95% of patients) - second leading cause of death in FAP
- Gastric fundic gland polyps (30-90%, low malignant potential)
- Gastric adenomas (10-30%, particularly in Asians)
- Hepatoblastoma
Ectodermal:
- Epidermoid/sebaceous cysts (~50%)
- Congenital hypertrophy of the retinal pigment epithelium (CHRPE; 75%) - detectable at birth, marker for early screening
- Pilomatrixoma
- Brain tumors (Turcot syndrome variant - medulloblastoma)
Mesodermal:
- Desmoid tumors (30%) - fibromatosis, may be intraabdominal; can be life-threatening
- Osteomas (80%) - especially mandible
- Dental abnormalities
FAP Variants:
- Gardner Syndrome: FAP + osteomas + desmoid tumors + soft tissue tumors (specific APC mutation)
- Turcot Syndrome: FAP + CNS malignancy (medulloblastoma); also seen with Lynch syndrome (glioblastoma)
- Attenuated FAP (AFAP): <100 adenomas; right colon predominance; APC mutation outside codons 168-1640; later onset; CRC risk still ~100% but delayed
Surveillance: Annual colonoscopy from age 10-12 years. EGD from age 20 years (using Spiegelman scoring for duodenal polyposis staging and surveillance intervals).
Treatment:
Surgery is aimed at preventing CRC. Options:
- Restorative proctocolectomy + IPAA (ileal pouch-anal anastomosis): Removes all colorectal mucosa; preferred for dense rectal polyposis; preserves continence; ~10% pouch failure rate; still requires surveillance of "rectal cuff" if stapled anastomosis
- Total colectomy + IRA (ileorectal anastomosis): Preserves rectum; suitable if <20 rectal polyps; rectum requires annual endoscopic surveillance; 10% develop rectal cancer
- Total proctocolectomy + end ileostomy: For patients who cannot undergo IPAA or where continence is not possible
Chemoprevention: Celecoxib (COX-2 inhibitor, FDA-approved for FAP) reduces polyp burden; sulindac decreases polyp number in retained rectum. NOT a substitute for surgery.
10.2 MUTYH-Associated Polyposis (MAP)
- Autosomal recessive - key distinction from FAP
- Biallelic mutation of base-excision repair gene MUTYH (MYH)
- <100 polyps; later onset than FAP
- Sessile serrated polyps, hyperplastic polyps, often with KRAS mutations
- CRC risk: ~80%
10.3 Lynch Syndrome (HNPCC)
- Autosomal dominant; mutations in MMR genes: MLH1, MSH2 (most common), MSH6, PMS2
- Not a true polyposis (few polyps), but markedly accelerated adenoma-to-carcinoma sequence
- Right-sided predominance; mucinous/signet ring histology; MSI-H tumors; better prognosis
- Amsterdam II criteria and revised Bethesda guidelines used for identification
- CRC risk: ~50-80%; also endometrial, ovarian, gastric, urinary tract, biliary cancers
- Surveillance: colonoscopy every 1-2 years from age 20-25 years
(Full table of polyposis syndromes - from Current Surgical Therapy 14e, Table 1 above)
11. Risk Factors for Colorectal Polyps
Non-modifiable:
- Age - most important determinant; risk increases steeply after age 50
- Male sex - RR ~1.5 vs women; men aged 45-49 have similar advanced adenoma prevalence as women aged 55-59
- Family history - first-degree relative with CRC/adenoma doubles risk
- Race - African Americans and Hispanics have greater proportion of proximal adenomas
Modifiable/Environmental:
- Low dietary fiber, high red/processed meat intake, high fat
- Obesity, physical inactivity - independently increase risk
- Smoking - strongly associated with serrated polyps and HP polyposis
- Alcohol - dose-dependent risk
- Diabetes/metabolic syndrome - increased risk via insulin resistance
Protective factors:
- NSAIDs/Aspirin (most well-established): >110 animal studies + >35 epidemiologic studies confirm 25-35% reduction in adenoma risk via COX-2 inhibition → reduced cellular proliferation, enhanced apoptosis, reduced angiogenesis
- 81 mg/day aspirin reduces RR of adenoma and advanced adenoma by 19% and 41% respectively (Sleisenger)
- Calcium supplements (modest effect)
- Hormone replacement therapy (HRT) in postmenopausal women
- Selenium
- Physical activity, weight loss
12. Clinical Presentation
Most polyps are asymptomatic - discovered on screening or incidental imaging. When symptomatic:
- Rectal bleeding - most common symptom (usually occult, detected on FOBT/FIT)
- Change in bowel habit - especially with large polyps
- Mucous secretion - especially villous adenomas; massive secretion (>3 L/day) causing dehydrating diarrhea = McKittrick-Wheelock syndrome
- Iron-deficiency anemia - from chronic occult blood loss
- Rarely: obstruction, intussusception (hamartomatous polyps in children), prolapse
13. Diagnosis
13.1 Colonoscopy
- Gold standard - detects and allows simultaneous removal
- Sensitivity: ~94% for polyps >10 mm; lower for flat/sessile lesions
- Reports polyp number, size, location, morphology (Paris classification)
13.2 Chromoendoscopy & Advanced Imaging
- NBI (narrow band imaging): Enhances vascular patterns; NICE classification (type 1 = hyperplastic, type 2 = adenoma)
- Kudo pit pattern: Type I/II = non-neoplastic; III-V = neoplastic; requires chromoendoscopy and high-magnification (100x)
- FICE, i-SCAN, linked color imaging (LCI): Enhanced imaging for improved adenoma detection rate (ADR)
13.3 CT Colonography (Virtual Colonoscopy)
- Sensitivity: 92% for polyps ≥10 mm; 78-86% for polyps 5-9 mm; poor for <5 mm
- Cannot biopsy/resect; detects incidental extracolic findings (up to 70% of cases; 11% clinically significant)
- Management of 6-9 mm polyps found on CTC remains debated
13.4 Stool Tests
- FIT: Sensitivity ~60-79% for adenomas; widely used for population screening
- Cologuard (multi-target stool DNA): Sensitivity 92% for CRC, but only ~42% for advanced adenomatous polyps
- Stool tests do not detect/remove polyps; positive result requires colonoscopy
14. Management
14.1 Polypectomy Techniques
- Cold snare polypectomy: Preferred for polyps <10 mm (no electrical current; lower delayed bleeding rate)
- Hot snare polypectomy: Larger polyps (10-19 mm); uses electrocautery
- EMR (Endoscopic Mucosal Resection): For sessile polyps ≥20 mm; submucosal saline injection to "lift" lesion before snare resection; piecemeal removal acceptable but reduces histologic staging ability
- ESD (Endoscopic Submucosal Dissection): En-bloc removal of large lesions; superior for staging malignant polyps; technically demanding
- Tattoo marking of sessile polypectomy sites - essential for subsequent endoscopic surveillance and surgical localization
- Argon plasma coagulation (APC): Adjunctive ablation of residual adenomatous tissue at polypectomy margins; not suitable as primary treatment (no specimen obtained)
14.2 Complications of Polypectomy
- Bleeding (most common): Usually immediate but can be delayed up to 2 weeks; self-limiting in most; managed with endoscopic clips, epinephrine injection, resnaring, APC; rarely requires angiography or surgery
- Perforation: Microperforation in a prepared patient - bowel rest + broad-spectrum antibiotics + observation; signs of sepsis/peritonitis = laparotomy
- Post-polypectomy syndrome: Transmural burn without free perforation; localized pain + fever after polypectomy; managed conservatively
14.3 Malignant Polyp Management
- Complete en-bloc endoscopic excision + histopathologic assessment
- If all favorable features: no further surgery
- If unfavorable features (poor differentiation, vascular invasion, involved margin, deep SM invasion): surgical resection
- Sessile malignant rectal polyps: consider full-thickness surgical excision (TAE, TEM, TAMIS) ± adjuvant chemoradiation for high-risk cases
- Re-colonoscopy at 3-6 months after large polyp removal to confirm completeness
15. Surveillance After Polypectomy
Polyp follow-up recommendations (adapted from BSG/ACPGBI guidelines - Bailey & Love:
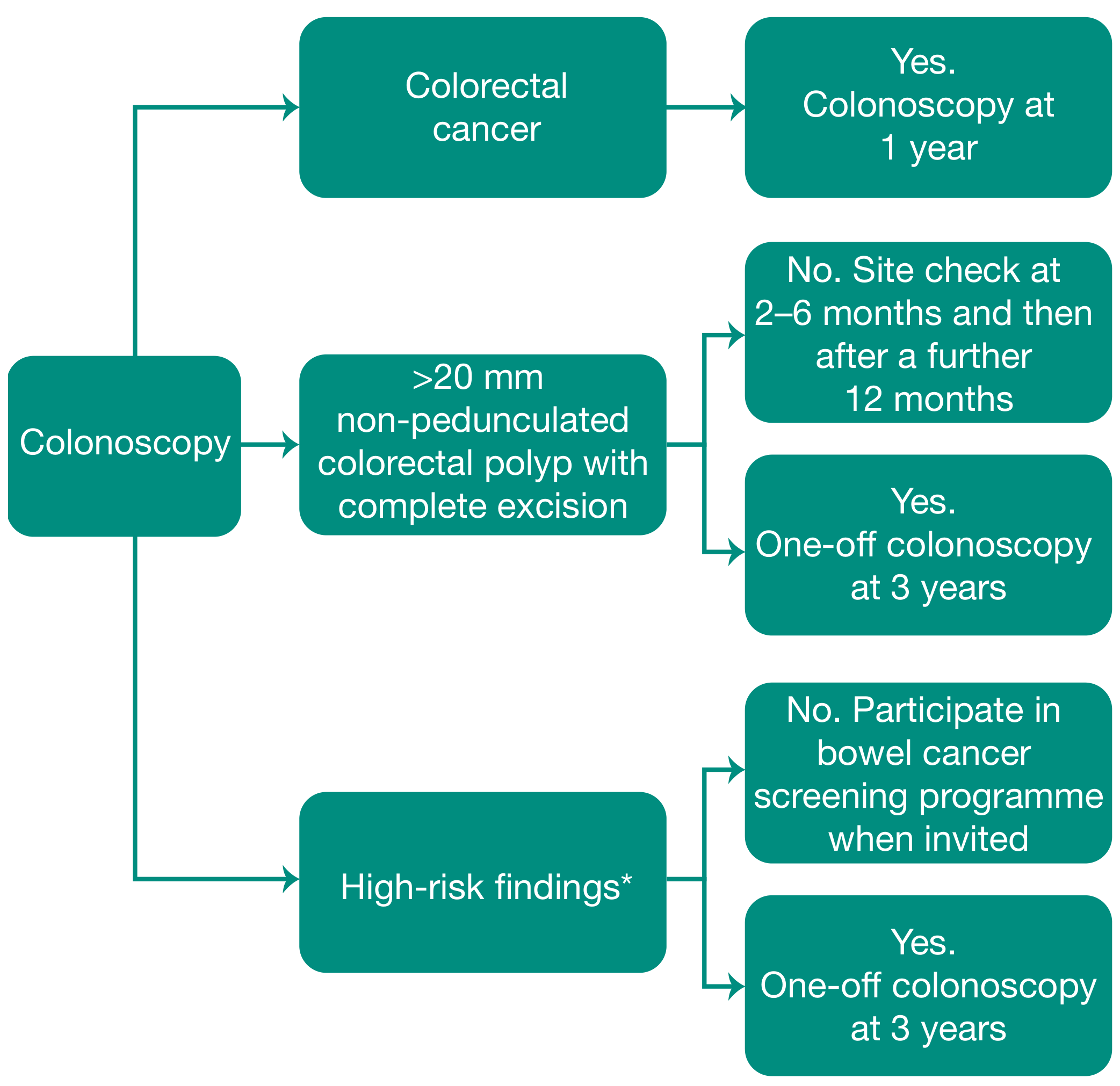
Fig. BSG/ACPGBI post-polypectomy surveillance recommendations
Standard surveillance intervals (from Sleisenger & Fordtran):
| Finding at Index Colonoscopy | Surveillance Interval | Risk Category |
|---|---|---|
| No adenomas | 10 years (average risk) | Low |
| 1-2 tubular adenomas <10 mm, LGD | 5-10 years | Low |
| 3-4 tubular adenomas <10 mm | 3 years | Moderate |
| 5-10 adenomas, OR any adenoma ≥10 mm, OR any with villous histology, OR any with HGD | 3 years | High |
| >10 adenomas | 1 year; investigate for polyposis syndrome | High |
| Piecemeal removal of large (≥20 mm) sessile polyp | 3-6 months (site check) then 1 year | High |
| Sessile serrated lesion ≥10 mm or with dysplasia | 3 years | High |
AGA 2023 Expert Review (PMID 37737817): updated risk stratification framework now incorporates serrated lesion features into post-polypectomy surveillance
16. Chemoprevention
| Agent | Evidence | Mechanism |
|---|---|---|
| Aspirin (81-325 mg/day) | Strong RCT evidence; 19-35% reduction | COX-1/COX-2 inhibition → ↓ proliferation, ↑ apoptosis, ↓ angiogenesis |
| Celecoxib (COX-2 inhibitor) | FDA-approved for FAP; APPROVe/APC/PreSap trials show benefit | Selective COX-2 inhibition; cardiovascular AE limits use |
| Calcium | Modest protection; ~15-20% reduction | Binds bile acids and fatty acids in colon lumen |
| Vitamin D | Emerging data | Anti-proliferative; promotes differentiation |
| Sulindac (NSAID) | Reduces polyp burden in FAP rectum | COX-1/COX-2; additional COX-independent mechanisms |
17. Pro-Level Molecular Summary Table
(from Robbins Cotran & Kumar, Table 17.10)
| Etiology | Molecular Defect | Target Genes | Inheritance | Site | Histology |
|---|---|---|---|---|---|
| FAP | APC/Wnt pathway | APC | AD | No predominance | Tubular/villous adenoma → typical adenocarcinoma |
| MAP (MUTYH) | Base excision repair | MUTYH | AR | No predominance | Sessile serrated → mucinous adenocarcinoma |
| Lynch syndrome (HNPCC) | MMR deficiency | MSH2, MLH1 | AD | Right side | Sessile serrated → mucinous adenocarcinoma |
| Sporadic CRC (70-80%) | APC/Wnt pathway | APC | None | Left side | Tubular/villous → typical adenocarcinoma |
| Sporadic CRC (10-15%) | MMR deficiency | MSH2, MLH1 | None | Right side | SSP → mucinous adenocarcinoma |
| Sporadic CRC (5-10%) | Hypermethylation/CIMP | MLH1, BRAF | None | Right side | SSP → mucinous adenocarcinoma |
18. Key Numbers to Memorize (Exam & Clinical Practice)
| Fact | Value |
|---|---|
| Risk of malignancy in tubular adenoma | 5% |
| Risk of malignancy in tubulovillous adenoma | 22% |
| Risk of malignancy in villous adenoma | Up to 40% |
| Risk of carcinoma in polyp >2 cm | 35-50% |
| % of CRC arising from adenomas (sporadic) | ~80% |
| Adenoma prevalence after age 50 (colonoscopy) | 20-53% |
| FAP - % with CRC if untreated | ~100% by age 35-40 |
| Lynch syndrome - CRC risk | 50-80% |
| Serrated polyposis - CRC risk | 30-50% |
| Peutz-Jeghers - CRC risk | 30-40% |
| Juvenile polyposis - CRC risk | 40% |
| SSA - % of all colonic polyps | ~9% |
| Adenoma recurrence rate within 3-5 years after polypectomy | 20-50% |
| LN metastasis risk at Haggitt level 4 / Sm3 | Up to 25-23% |
| Unfavorable features → adverse outcome risk | 10-25% (up to 45-50%) |
Recent Guidelines Update
- AGA 2023 Post-Polypectomy Surveillance Update [PMID 37737817]: Updated risk stratification for post-polypectomy surveillance now incorporates serrated lesion features; patients with SSLs ≥10 mm or with dysplasia are now explicitly placed in the high-risk (3-year interval) category.
- EHTG-ESCP 2024 FAP/MAP Guidelines [PMID 38722804]: Updated European guidelines for management of adenomatous polyposis syndromes including FAP, MAP, and GAPPS; emphasizes individualized surgical approach and endoscopic surveillance protocols.
- AGA Living CPG on Computer-Aided Detection (CADe) Colonoscopy [PMID 40121061]: AI-assisted colonoscopy modestly but significantly increases adenoma detection rate (ADR); now endorsed as an adjunct in routine colonoscopy.
Sources:
- Schwartz's Principles of Surgery, 11e (Chapter on Colorectal Polyps)
- Sleisenger & Fordtran's GI and Liver Disease, Chapter 126 (Colonic Polyps and Polyposis Syndromes)
- Yamada's Textbook of Gastroenterology, 7e, Chapter 70
- Bailey & Love's Short Practice of Surgery, 28e, Chapter 77
- Robbins & Kumar Basic Pathology / Robbins Cotran & Kumar Pathologic Basis of Disease, Chapter 17
- Current Surgical Therapy, 14e (Colorectal Polyps chapter)
This is a shared conversation. Sign in to Orris to start your own chat.