Chronic pancreatitis
Reading File
Finding Sources
Searching PubMed
"chronic pancreatitis"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the complete answer.
Chronic Pancreatitis
Definition & Overview
Chronic pancreatitis (CP) is an irreversible inflammatory disease of the pancreas resulting in progressive fibrosis, permanent destruction of the exocrine parenchyma, and eventually loss of the islets of Langerhans. Unlike acute pancreatitis, the damage does not resolve. Recurrent bouts of acute pancreatitis of any etiology can evolve over time into CP. Prevalence ranges from 9-62 per 100,000 globally, with incidence between 5-14 per 100,000 persons.
- Robbins & Kumar Basic Pathology, p. 3045
- Grainger & Allison's Diagnostic Radiology, p. 687
Etiology & Classification (TIGAR-O)
| Category | Examples |
|---|---|
| Toxic-metabolic | Alcohol (most common - esp. middle-aged men), tobacco, hypercalcemia, hyperlipidemia, renal failure, drugs |
| Idiopathic | Early-onset, late-onset (up to 40% of cases) |
| Genetic | PRSS1 (cationic trypsinogen), SPINK1 (trypsin inhibitor), CFTR mutations |
| Autoimmune | IgG4-related (Type 1), non-IgG4 (Type 2) |
| Recurrent acute pancreatitis | Necrosis-fibrosis sequence |
| Obstructive | Pancreatic ductal adenocarcinoma, IPMN, strictures, pancreas divisum |
Alcohol mechanism: may alter activation of digestive enzymes, increase oxygen-derived free radicals, or exert direct toxic effects on acinar cells.
- Robbins & Kumar Basic Pathology, p. 3047-3048
Pathology
Gross: Hard gland, extremely dilated ducts, visible calcific concretions.
Microscopy (key features):
- Parenchymal fibrosis
- Reduced number and size of acini (acinar loss is constant)
- Variable dilation of pancreatic ducts
- Relative early sparing of islets of Langerhans (eventually destroyed)
- Chronic inflammatory infiltrate around lobules and ducts
- Ductal epithelium: atrophy, hyperplasia, or squamous metaplasia
- Ductal concretions
Autoimmune pancreatitis specifically: "Swirling" fibrosis + venulitis (lymphocytic sclerosing pancreatitis), dense infiltration by IgG4-positive lymphocytes and plasma cells.
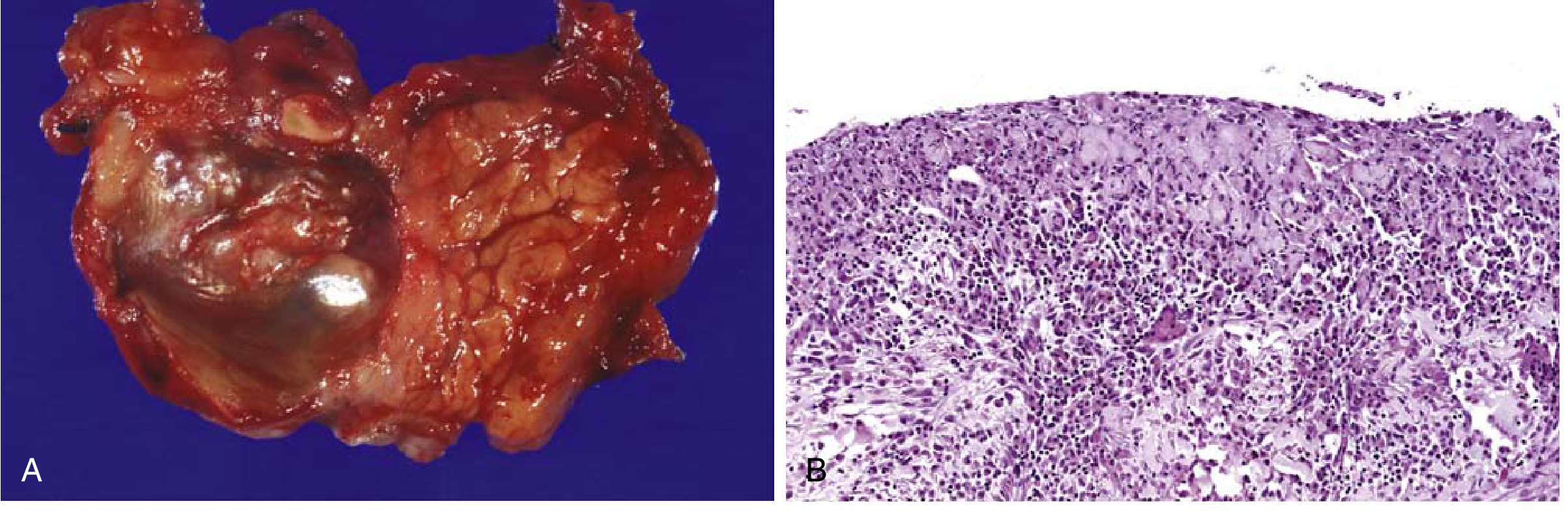
Fig. 15.5 - Robbins & Kumar: (A) Gross specimen - hard fibrotic pancreas with calcific concretions. (B) Histology - parenchymal fibrosis, reduced acini, chronic inflammatory infiltrate.
- Robbins & Kumar Basic Pathology, p. 3056-3060
Clinical Features
| Feature | Details |
|---|---|
| Pain | Most common symptom; persistent/recurrent epigastric and back pain, may radiate to back |
| Exocrine insufficiency | Steatorrhoea, malabsorption, weight loss (affects 36% of CP patients) |
| Endocrine insufficiency | Diabetes mellitus (affects 41% of CP patients) |
| Jaundice | Repeated bouts, from common bile duct narrowing |
| Silent presentation | Some patients present only with exocrine/endocrine insufficiency without prior pain |
- Robbins & Kumar Basic Pathology, p. 3062
- Grainger & Allison's Diagnostic Radiology, p. 687
Complications
| Complication | Note |
|---|---|
| Chronic abdominal pain | Often dominant, complex central sensitization component |
| Exocrine pancreatic insufficiency | Fat-soluble vitamin deficiency, steatorrhoea |
| Diabetes mellitus (Type 3c) | Due to islet destruction |
| Pseudocyst formation | Common |
| Bile duct stricture / biliary cirrhosis | |
| Pancreatic duct stricture | |
| Splanchnic venous thrombosis | Splenic, mesenteric, portal vein |
| Metabolic bone disease | Osteoporosis from malabsorption |
| Pancreatic cancer | Up to 16-fold increased risk in long-standing CP |
| Malnutrition / micronutrient deficiencies |
- Harrison's Principles of Internal Medicine 22E, Table 339-7
- Grainger & Allison's Diagnostic Radiology, p. 687
Diagnosis
Imaging
Plain X-ray: Pancreatic calcification (highly suggestive of alcohol-related CP).
Ultrasound: Heterogeneous echotexture, MPD dilation (normal <2.5 mm), side branch dilation.
CT: Best initial cross-sectional modality. Combination of ≥3 of four features gives high specificity:
- Parenchymal calcifications
- Intraductal calcification
- Parenchymal atrophy
- Cystic lesions
Early CP is difficult to diagnose on CT. Focal CP may mimic ductal adenocarcinoma.
MRI/MRCP: Preferred for ductal imaging, avoids ERCP complications. DWI helps exclude tumour. Findings: multifocal stenoses of MPD and side branches, intraductal filling defects (protein plugs), areas of calcification.
ERCP: Gold standard for ductal anatomy but carries procedural risk. The "duct penetrating sign" helps differentiate focal inflammatory mass from cancer (duct traverses inflammatory mass without complete obstruction; cancer completely obstructs the duct).
EUS: High sensitivity, especially for early/minimal change CP. Can detect changes before CT/MRI. Should be performed after acute episode has resolved.
EUS Criteria
Traditional criteria (sum of features):
| Parenchymal | Ductal |
|---|---|
| Hyperechoic strands | Stones |
| Hyperechoic foci | Main duct irregularity |
| Lobularity | Hyperechoic main duct wall |
| Cysts | Visible side branches; MPD dilation |
Rosemont criteria (2009): More specific, uses Major A / Major B / Minor criteria weighting - e.g., hyperechoic foci with shadowing = Major A; lobularity with honeycombing = Major A.
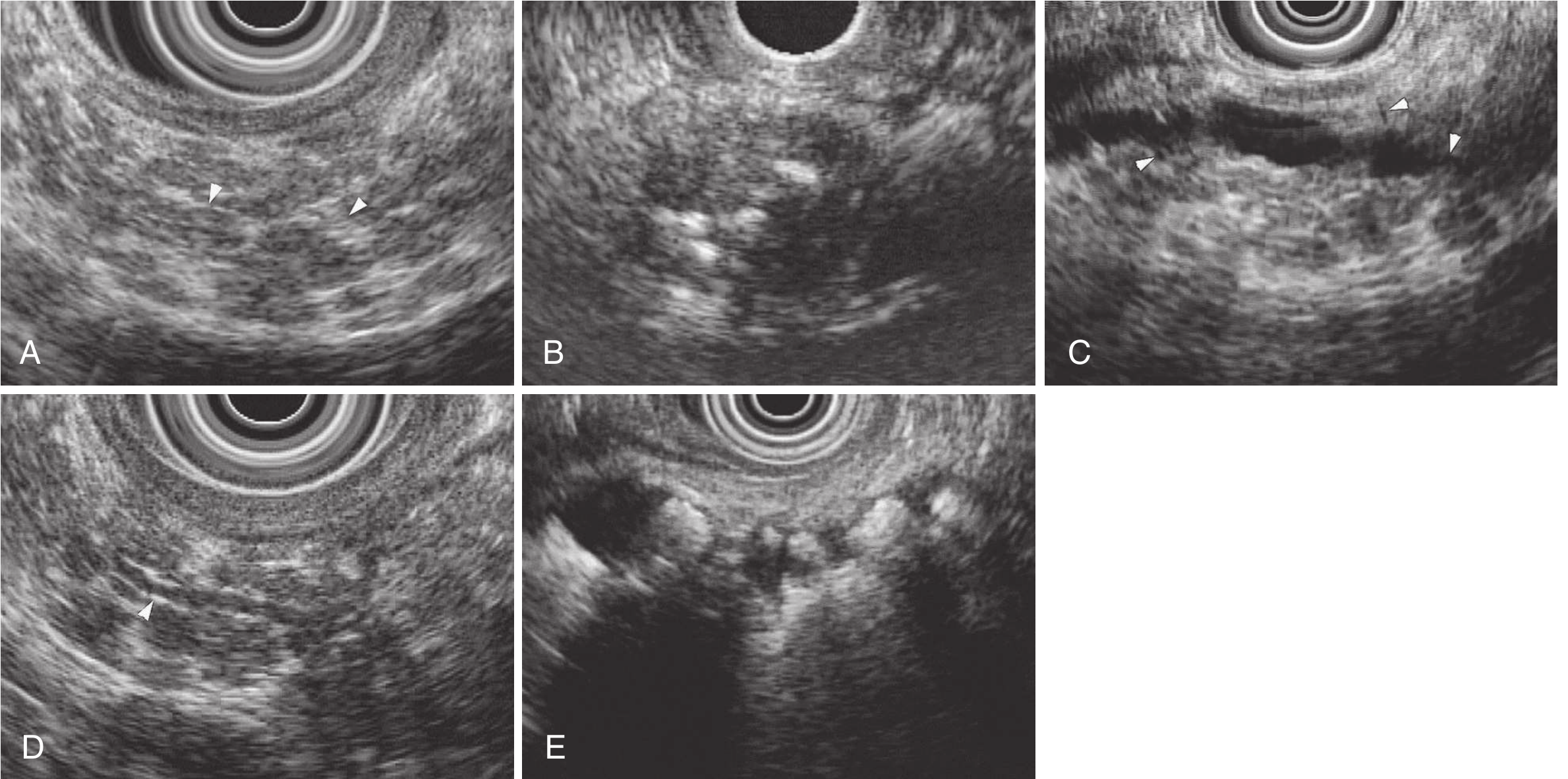
Fig 51.8 - Clinical GI Endoscopy: EUS features of chronic pancreatitis.
- Clinical Gastrointestinal Endoscopy 3e, p. 765-766
- Grainger & Allison's Diagnostic Radiology, p. 687
Functional Tests
- Fecal elastase (low = exocrine insufficiency)
- Serum trypsin (low in advanced disease)
- Tube-based secretin test / endoscopic secretin test (if imaging equivocal)
- HbA1c or GTT for endocrine insufficiency
Management
The management algorithm below (from Schwartz's Surgery/Forsmark 2013) summarizes the overall approach:
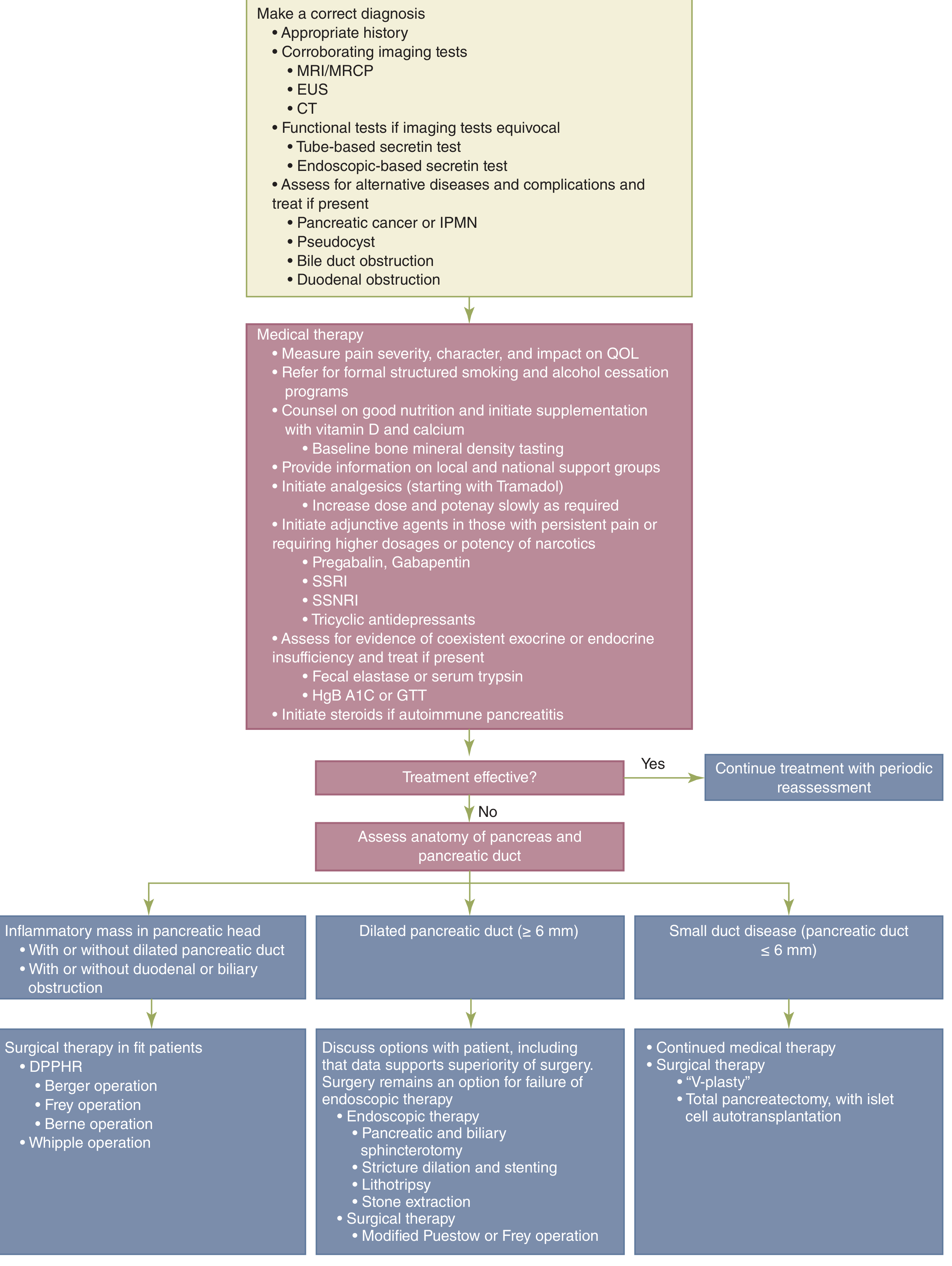
Step 1: Correct Diagnosis + Treat Complications
- Rule out pancreatic cancer/IPMN, pseudocyst, bile duct obstruction, duodenal obstruction
Step 2: Medical Therapy
Pain management:
- Smoking and alcohol cessation (formal structured programs)
- Analgesics: start with tramadol, escalate dose slowly; use opioids if necessary
- Adjunctive agents (for persistent pain or reducing narcotic dose):
- Pregabalin / gabapentin (one RCT showed reduction in pain scores)
- SSRIs, SNRIs, tricyclic antidepressants
- Antioxidants: mixed results in studies
- Pancreatic enzyme supplementation: meta-analyses show no consistent benefit for pain; benefit may be through improving dyspepsia/maldigestion
- Octreotide (somatostatin analogue): 200 μg SC TID showed 65% pain relief vs 35% placebo (best in obstructive pancreatopathy with chronic pain)
- Celiac plexus block (EUS-guided): 55% initial relief, but durable >6 months in only 10%; conditional recommendation, low-quality evidence
Nutritional/other:
- Vitamin D and calcium supplementation; baseline bone mineral density testing
- Manage exocrine insufficiency: pancreatic enzyme replacement therapy (PERT)
- Manage diabetes (Type 3c)
- Autoimmune pancreatitis: responds to corticosteroids (and anti-B cell therapy)
Step 3: Assess Pancreatic Ductal Anatomy (if medical therapy fails)
Three anatomical scenarios guide further therapy:
A. Dilated Pancreatic Duct (≥6 mm)
Endoscopic options (first line):
- Pancreatic and biliary sphincterotomy
- Stricture dilation and stenting
- ESWL (extracorporeal shock wave lithotripsy) + stone extraction
Surgical therapy (data supports superiority over endoscopy - 2 RCTs):
- Modified Puestow procedure (longitudinal pancreaticojejunostomy) - lateral drainage
- Frey operation (local resection of pancreatic head + lateral PJ)
- 80% immediate pain relief; ~50% pain recurrence by 3 years
A landmark study (Nealon & Thompson 1993) showed early surgical ductal decompression delays or prevents progression of CP - the only therapy shown to do so (Table 33-20 data: operated group, 87% remained mild-moderate at 24 months vs only 22% in the non-operated group).
B. Inflammatory Mass in Pancreatic Head
Surgical options:
- DPPHR (duodenum-preserving pancreatic head resection):
- Berger operation
- Frey operation
- Berne operation
- Whipple operation (pancreaticoduodenectomy) if cancer cannot be excluded
C. Small Duct Disease (duct ≤6 mm)
-
Continue medical therapy
-
Surgical options: "V-plasty" or total pancreatectomy with islet cell autotransplantation (TP-IAT) for intractable pain, hereditary pancreatitis, or failed previous surgery
- Patients with shorter symptom duration and lower pre-op opioid requirements do best
- Some patients have persistent pain post-operatively (central sensitization)
-
Schwartz's Principles of Surgery 11e, p. 1393-1418
-
Harrison's Principles of Internal Medicine 22E, p. 2796-2797
-
Clinical Gastrointestinal Endoscopy 3e, p. 765
Special Entity: Autoimmune Pancreatitis (AIP)
-
Type 1 (IgG4-related): Most common form; IgG4+ plasma cells, storiform fibrosis, obstructive phlebitis; may involve biliary tree, salivary glands, kidneys; responds to steroids
-
Type 2: Granulocytic epithelial lesion (GEL); associated with IBD; responds to steroids
-
Key: recognize because it is steroid-responsive - avoids unnecessary surgery
-
Serum IgG4 elevated (>2x upper limit - highly suggestive)
-
Robbins & Kumar Basic Pathology, p. 3051, 3060
Summary
| Aspect | Key Points |
|---|---|
| Most common cause | Chronic alcohol use (middle-aged men) |
| Cardinal symptom | Chronic abdominal/back pain |
| Pathology hallmark | Parenchymal fibrosis + acinar loss + ductal concretions |
| Best imaging (duct) | MRCP / ERCP |
| Best early detection | EUS |
| Exocrine insufficiency | PERT |
| Endocrine insufficiency | Insulin/diabetes management |
| Pain - first line | Alcohol/smoking cessation + tramadol ± pregabalin |
| Pain - ductal dilation | Surgery superior to endoscopy (2 RCTs) |
| Special form | Autoimmune pancreatitis - steroid-responsive |
| Long-term risk | 16-fold increased pancreatic cancer risk |
This is a shared conversation. Sign in to Orris to start your own chat.