cd /tmp/workspace/attachments/3d7fae28-4455-4cce-b741-e3b327babd9f/ && python3 -c " import pdfplumber with pdfplumber.open('93fb34af-6ff1-4e5b-9cbe-30ddec6a76a7.pdf') as pdf: print(f'Pages: {len(pdf.pages)}') for i, page in enumerate(pdf.pages[:3]): print(f'--- Page {i+1} ---') text = page.extract_text() if text: print(text[:1500]) else: print('[No text extracted]') "
Chance of selection
python3 -c " import pdfplumber with pdfplumber.open('/tmp/workspace/attachments/3d7fae28-4455-4cce-b741-e3b327babd9f/93fb34af-6ff1-4e5b-9cbe-30ddec6a76a7.pdf') as pdf: print(f'Total Pages: {len(pdf.pages)}') for i, page in enumerate(pdf.pages): print(f'=== Page {i+1} ===') text = page.extract_text() if text: print(text) else: print('[No text]') "
find /tmp/workspace/attachments/ -name "*.pdf" 2>/dev/null && ls /tmp/workspace/attachments/
/tmp/workspace
Chance of Selection - Honest Assessment
Overall Verdict: Moderate (50-65%) - Competitive but needs strengthening
Strengths (What works in its favour)
Weaknesses (What may hurt selection)
How to Improve Selection Chances
| Fix | Impact |
|---|---|
| Add full sample size formula with r-value | High |
| Add statistical tests (Pearson r, regression, ROC) | High |
| Expand literature review to 12-15 references with recent papers | Medium |
| Justify Harvard Step Test choice | Medium |
| Add a timeline / Gantt chart | Low-Medium |
| Mention ethics approval status | Low |
Context Matters
- ICMR STS (Short Term Studentship) - Moderate-High chance if above gaps are fixed; the topic fits their priorities well
- College-level project selection - High chance; most internal committees favour feasibility over perfection
- State/National conference abstract - Moderate; needs stronger methods section
- Journal submission (post-data collection) - Will need full data before this matters
Out of 10 chance of selection is?
6/10
| Factor | Score |
|---|---|
| Topic relevance & novelty | 8/10 |
| Study design & feasibility | 7/10 |
| Objectives & hypothesis clarity | 7/10 |
| Methodology detail | 5/10 |
| Literature review depth | 5/10 |
| Sample size justification | 4/10 |
| Statistical analysis plan | 4/10 |
If it is not selected what can I do
If Not Selected - Your Options
1. Resubmit to Another Scheme (Most Common Path)
| Scheme | Eligibility | Stipend | Deadline |
|---|---|---|---|
| ICMR STS | MBBS 1st-3rd year | ₹10,000/month | Usually Jan-Feb |
| DBT Star College | UG students | Project grant | Varies |
| Indian Physiological Society | Medical students | Recognition + certificate | Annual |
| State Medical Council projects | MBBS students | Varies by state | Check locally |
2. Do the Study Anyway (Best Long-Term Move)
- A stadiometer and measuring tape (already in your physiology department)
- 100 willing classmates
- Harvard Step Test equipment (standard in physiology labs)
- Zero extra cost
- Submit as a conference abstract (PHYSICON, ASICON, college fests)
- Publish in a student/indexed journal (JCDR, IJPP, NJIRM)
- Use it as a thesis if your university allows
3. Strengthen and Resubmit Next Cycle
"Using r = 0.35 from [reference], with α = 0.05 and power = 80%, minimum n = 61; rounded to 100 for attrition."
"Pearson/Spearman correlation, multiple linear regression, ROC curve analysis with AUC for cutoff values."
4. Find a Co-Guide or Senior Collaborator
Bottom Line
It boost my cv
Yes - Massively. Here's Why.
CV Value - Ranked by Impact
| Achievement | CV Weight |
|---|---|
| Published paper (indexed journal) | ⭐⭐⭐⭐⭐ Highest |
| Oral/poster at national conference | ⭐⭐⭐⭐ |
| ICMR STS completion certificate | ⭐⭐⭐⭐ |
| Oral/poster at state/college level | ⭐⭐⭐ |
| Project submitted (even if ongoing) | ⭐⭐ |
Where It Helps You Specifically
- Doesn't affect marks, but helps in interviews for MD seats in Physiology, Community Medicine, Internal Medicine
- Interviewers ask "tell me about your research experience" - having a real answer is a differentiator
- Research publications are heavily weighted for residency applications abroad, especially in the US (ERAS application)
- ICMR, Wellcome Trust, Fogarty - all ask for prior research experience
The Smart Play
Do the study now (free, using college resources)
↓
Present at a college/state conference (get certificate)
↓
Submit to a journal like JCDR or IJPP
↓
Published paper by final year MBBS
↓
Strong CV before internship even starts
Thank you
- Strengthening the proposal before resubmission
- Statistical analysis once you collect data
- Writing up the paper for publication
Gfr
Glomerular Filtration Rate (GFR)
Definition
Normal Values
| Group | Normal GFR |
|---|---|
| Men | ~120 ± 25 mL/min |
| Women | ~95 ± 20 mL/min |
| Expressed per body surface area | ~125 mL/min per 1.73 m² |
The Driving Force (Starling Forces at Glomerulus)
SNGFR = Kf × [(Pgc - Pbs) - (πgc - πbs)]
| Variable | Value | Meaning |
|---|---|---|
| Kf | Ultrafiltration coefficient | Surface area × hydraulic conductivity |
| Pgc | ~45 mmHg | Glomerular capillary hydrostatic pressure |
| Pbs | ~10 mmHg | Bowman's space hydrostatic pressure |
| πgc | ~25 mmHg | Glomerular capillary oncotic pressure |
| πbs | ~0 mmHg | Bowman's space oncotic pressure |
Measurement of GFR
- Inulin is freely filtered, NOT reabsorbed or secreted
- Must be given IV (not produced in the body)
- GFR = (Uinulin × V) / Pinulin
- Example: Urine [inulin] = 125 mg/mL, Urine flow = 1 mL/min, Plasma [inulin] = 1 mg/mL → GFR = 125 mL/min
- Guyton & Hall Medical Physiology
- Creatinine = byproduct of muscle phosphocreatine breakdown
- Freely filtered + small amount tubularly secreted → slightly overestimates GFR
- Formula: CCr = ([Cr]U × urine flow) / [Cr]P
- The tubular secretion error and assay measurement error tend to cancel out, making it a practical estimate
- Guyton & Hall Medical Physiology
Clearance Formula (General)
Cx = (Ux × V) / Px
CKD Staging by GFR (KDIGO)
| Stage | eGFR (mL/min/1.73 m²) | Description |
|---|---|---|
| G1 | ≥ 90 | Normal / high |
| G2 | 60-89 | Mildly decreased |
| G3a | 45-59 | Mild-moderately decreased |
| G3b | 30-44 | Moderate-severely decreased |
| G4 | 15-29 | Severely decreased |
| G5 | < 15 | Kidney failure |
- GFR < 60 mL/min/1.73 m² is where anemia, acidosis, hyperphosphatemia, hypoalbuminemia, and hyperparathyroidism begin to appear
- Lower eGFR + higher albuminuria = independently associated with cardiovascular mortality and all-cause mortality - Comprehensive Clinical Nephrology, 7th Ed.
Factors That Affect GFR
| Factor | Effect on GFR |
|---|---|
| Afferent arteriole dilation | Increases |
| Afferent arteriole constriction | Decreases |
| Efferent arteriole constriction | Increases (initially) |
| Increased Kf (surface area) | Increases |
| Raised plasma oncotic pressure | Decreases |
| Increased Bowman's capsule pressure (e.g. obstruction) | Decreases |
| Low birth weight / preterm birth | Risk factor for reduced GFR long-term |
Key Exam Points
- Inulin = gold standard (IV, not practical clinically)
- Creatinine clearance = overestimates GFR (tubular secretion)
- Cystatin C = emerging reliable marker, not affected by muscle mass
- PAH clearance = measures Effective Renal Plasma Flow (ERPF), not GFR
- Filtration fraction = GFR/RPF = ~20%
How does GFR change with age or disease?
How GFR Changes with Age and Disease
PART 1 - GFR and Aging
The Normal Decline Pattern
| Landmark Study | Finding |
|---|---|
| Davies & Shock (pioneering, n=70, ages 24-89) | Inulin clearance showed linear GFR decline after age 30; oldest group had 46% less GFR than youngest |
| Lindeman et al. (longitudinal, 254 subjects, 14 years) | Mean annual decline = 7.5 mL/min per decade via creatinine clearance |
| Aging Kidney Anatomy Study (n=4500 kidney donors) | eGFR decline = 7.4 mL/min/decade; measured GFR = 6.1 mL/min/decade |
- Brenner and Rector's The Kidney, 2-Volume Set
Reference GFR Values by Age (Kidney Donors - Healthy Individuals)
| Age Group | Median eGFR |
|---|---|
| 18-19 years | ~114 mL/min/1.73 m² |
| Declines progressively | ~6-7.5 mL/min per decade |
| By 70-80 years | Often 50-70 mL/min/1.73 m² |
Important: One-third of subjects in Lindeman's study had NO decline, and a small subset actually increased - likely due to hyperfiltration from comorbidities (obesity, diabetes). Not everyone declines equally.
Why Does GFR Fall With Age? (Mechanisms)
- Glomerulosclerosis - prevalence rises from 2.7% (ages 18-29) to 73% (ages 70-77) in kidney biopsies of healthy donors
- Tubular atrophy and interstitial fibrosis accompany sclerosis
- Arteriosclerosis reduces renal blood flow
- Reduced Kf (ultrafiltration coefficient) - in older subjects: 4.9 vs 7.0 nL/min-mmHg in younger subjects
- Compensatory hypertrophy of remaining nephrons - initially preserves GFR, but causes glomerular capillary hypertension and further damage over time
- Blunted vasodilatory reserve - aged kidneys already in compensatory vasodilation and cannot dilate further; vasoconstrictive response to Ang II remains intact
CKD Prevalence Rises with Age
- CKD prevalence = up to 56% in those aged 75+
- Older age paradox: relative risk of ESKD per unit GFR decline doesn't increase in older patients (competing risk of death), BUT absolute risk of death is higher in older patients with lower GFR
- In patients aged 65+, risk of ESKD exceeds risk of death only when GFR ≤ 15 mL/min/1.73 m² - Brenner and Rector's The Kidney
PART 2 - GFR Changes in Disease
1. Diabetes Mellitus (Diabetic Nephropathy)
Glomerular hyperfiltration + renal hypertrophy
↓ (5-10 years)
Microalbuminuria (30-300 mg/24h)
↓ (5-10 more years)
Proteinuria + declining GFR
↓
ESKD
- Hyperglycemia activates RAAS, increases glomerular capillary pressure
- SGLT1/SGLT2 upregulation in proximal tubule → decreased Na delivery to macula densa → hyperfiltration
- Advanced glycosylation end products, TGF-β, connective tissue growth factor → glomerular matrix accumulation
- GFR decline rate = 1.8 to 14 mL/min/year (variable, depends on treatment)
- Up to 24% of T1DM and 50% of T2DM CKD patients are normoalbuminuric today (contemporary treatment effect)
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025)
2. Hypertension
- Hypertension accelerates GFR decline (systolic BP rise with age directly correlates with creatinine clearance decline)
- Increased incidence of GFR decline over 5 years in hypertensive patients
- Mechanism: systemic hypertension transmitted to glomerular capillaries → glomerular capillary hypertension → sclerosis
- Brenner and Rector's The Kidney
3. Acute Kidney Injury (AKI)
- Sudden, rapid fall in GFR over hours to days
- Causes: prerenal (reduced perfusion), intrinsic (glomerulonephritis, tubular necrosis), postrenal (obstruction)
- GFR can recover fully if the cause is reversed early
4. Chronic Kidney Disease (CKD) - General
- Lower eGFR = graded increased risk of anemia, acidosis, hyperphosphatemia, hypoalbuminemia, hyperparathyroidism (all worsening at GFR < 60)
- Lower eGFR + albuminuria = independently associated with cardiovascular mortality and all-cause mortality
- Rate of decline varies by disease type and treatment
Summary Table
| Condition | GFR Change | Rate |
|---|---|---|
| Normal aging (after 40) | Gradual decline | ~6-7.5 mL/min/decade |
| Diabetic nephropathy | Hyperfiltration first, then decline | 1.8-14 mL/min/year |
| Hypertension | Accelerated decline | Variable |
| AKI | Sudden sharp fall | Hours-days |
| CKD progression | Steady decline | Variable by cause |
| Unilateral nephrectomy | Compensatory rise in remaining kidney | Partial compensation |
| Pregnancy | GFR increases ~50% | (physiological hyperfiltration) |
Starling force
Starling Forces
The 4 Starling Forces
| Force | Direction | Normal Value | Effect |
|---|---|---|---|
| Capillary hydrostatic pressure (Pc) | Outward (filtration) | ~35 mmHg (arterial end) / ~15 mmHg (venous end) | Pushes fluid OUT into interstitium |
| Interstitial hydrostatic pressure (Pi) | Inward (opposes filtration) | ~-3 mmHg (slightly negative) | Pulls fluid INTO capillary (slightly) |
| Plasma oncotic pressure (πc) | Inward (absorption) | ~25-28 mmHg | Pulls fluid INTO capillary |
| Interstitial oncotic pressure (πi) | Outward (opposes absorption) | ~5-8 mmHg | Pushes fluid OUT |
The Starling Equation
Jv = Kf × [(Pc - Pi) - σ(πc - πi)]
| Symbol | Meaning |
|---|---|
| Jv | Net fluid flow across capillary |
| Kf | Filtration coefficient (hydraulic conductance × surface area) |
| Pc - Pi | Net hydrostatic pressure gradient |
| πc - πi | Net oncotic pressure gradient |
| σ | Reflection coefficient (0 = freely permeable; 1 = completely impermeable to protein) |
- If Jv is positive → net filtration (fluid moves OUT into interstitium)
- If Jv is negative → net absorption (fluid moves INTO capillary)
What Happens Along the Capillary
ARTERIAL END VENOUS END
Pc = ~35 mmHg (high) Pc = ~15 mmHg (low)
πc = ~25 mmHg πc = ~28 mmHg (rises as water leaves)
Net filtration pressure = +10 mmHg Net absorption pressure = +10 mmHg
→ Fluid moves OUT → Fluid moves IN
-
At the arterial end: hydrostatic pressure exceeds oncotic pressure → fluid filters OUT
-
At the venous end: as water leaves, plasma proteins concentrate → oncotic pressure rises, hydrostatic falls → fluid is drawn back IN
-
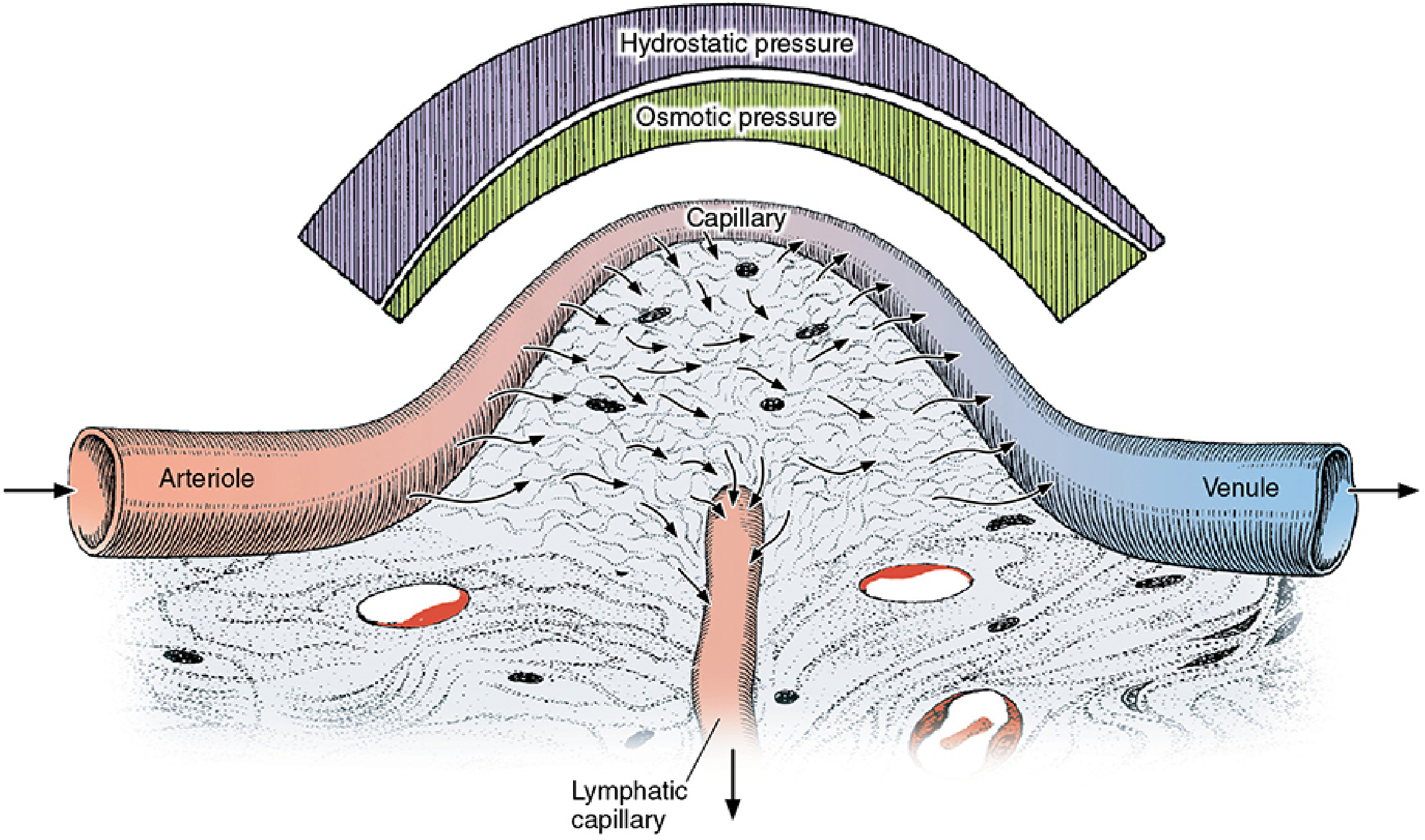
Not all filtered fluid is reabsorbed - the excess (~2-4 L/day) is returned via lymphatics
-
Junqueira's Basic Histology, 17th Ed.; Comprehensive Clinical Nephrology, 7th Ed.
Why Plasma Proteins (Albumin) Matter
- Capillary walls are freely permeable to small solutes (Na+, glucose) but poorly permeable to proteins
- So only proteins generate an effective osmotic gradient (oncotic pressure) across the capillary wall
- Small solute concentrations equilibrate on both sides → cancel out
- Albumin is the main contributor to oncotic pressure (~80% of total)
- Comprehensive Clinical Nephrology, 7th Ed.
Causes of Edema (Starling Force Imbalance)
| Mechanism | Example | Starling Force Altered |
|---|---|---|
| ↑ Capillary hydrostatic pressure | Heart failure, venous obstruction, excess IV fluids | ↑ Pc |
| ↓ Plasma oncotic pressure | Hypoalbuminemia (liver failure, nephrotic syndrome, malnutrition) | ↓ πc |
| ↑ Capillary permeability | Inflammation, sepsis, burns, anaphylaxis | ↑ Kf, ↑ σ leakage of protein into interstitium |
| Lymphatic obstruction | Filariasis, post-mastectomy lymphedema, tumor obstruction | Excess filtrate not drained |
| ↑ Interstitial oncotic pressure | Protein leakage into interstitium | ↑ πi |
Starling Forces at the Glomerulus (Renal Application)
| Force | Value |
|---|---|
| Glomerular capillary hydrostatic pressure (Pgc) | ~45 mmHg |
| Bowman's space hydrostatic pressure (Pbs) | ~10 mmHg |
| Glomerular capillary oncotic pressure (πgc) | ~25 mmHg |
| Bowman's space oncotic pressure (πbs) | ~0 mmHg |
| Net ultrafiltration pressure | ~10 mmHg |
Key Exam Points
- Oncotic pressure = colloid osmotic pressure (same thing, different names)
- Normal net fluid movement = slightly outward overall (filtration exceeds absorption)
- Lymphatics handle the excess (~2-4 L/day)
- Albumin = main determinant of oncotic pressure; hypoalbuminemia → edema
- Increased capillary permeability causes inflammatory edema (protein-rich exudate)
- Cardiac failure edema = ↑ venous back-pressure → ↑ Pc
Give as in gkpaul
STARLING FORCES (Starling Hypothesis of Capillary Exchange)
Definition
The Starling Equation
Jv = Kf [(Pc - Pi) - (πc - πi)]
| Symbol | Meaning |
|---|---|
| Jv | Net fluid movement (mL/min) |
| Kf | Hydraulic conductance (filtration coefficient) |
| Pc | Capillary hydrostatic pressure |
| Pi | Interstitial hydrostatic pressure |
| πc | Capillary oncotic pressure |
| πi | Interstitial oncotic pressure |
- Jv positive (+) → Net filtration (fluid moves OUT into interstitium)
- Jv negative (-) → Net absorption (fluid moves INTO capillary)
The 4 Starling Forces
Forces Favouring FILTRATION (fluid OUT of capillary) ➕
- Generated by cardiac contraction
- Higher at arterial end (~35 mmHg), lower at venous end (~15 mmHg)
- More affected by venous pressure than arterial pressure
- ↑ in: heart failure, venous obstruction
- Due to small amount of protein in interstitial fluid
- Normally very low (proteins don't easily cross capillary wall)
- ↑ in: capillary injury (proteins leak out)
Forces Favouring ABSORPTION (fluid INTO capillary) ➖
- Due to plasma proteins, mainly albumin (80%)
- Main force holding fluid inside the capillary
- ↓ in: hypoalbuminemia (liver failure, nephrotic syndrome, malnutrition) → oedema
- Slightly negative normally (tissue gel resists compression)
- Opposes filtration
Net Filtration Pressure - Worked Example
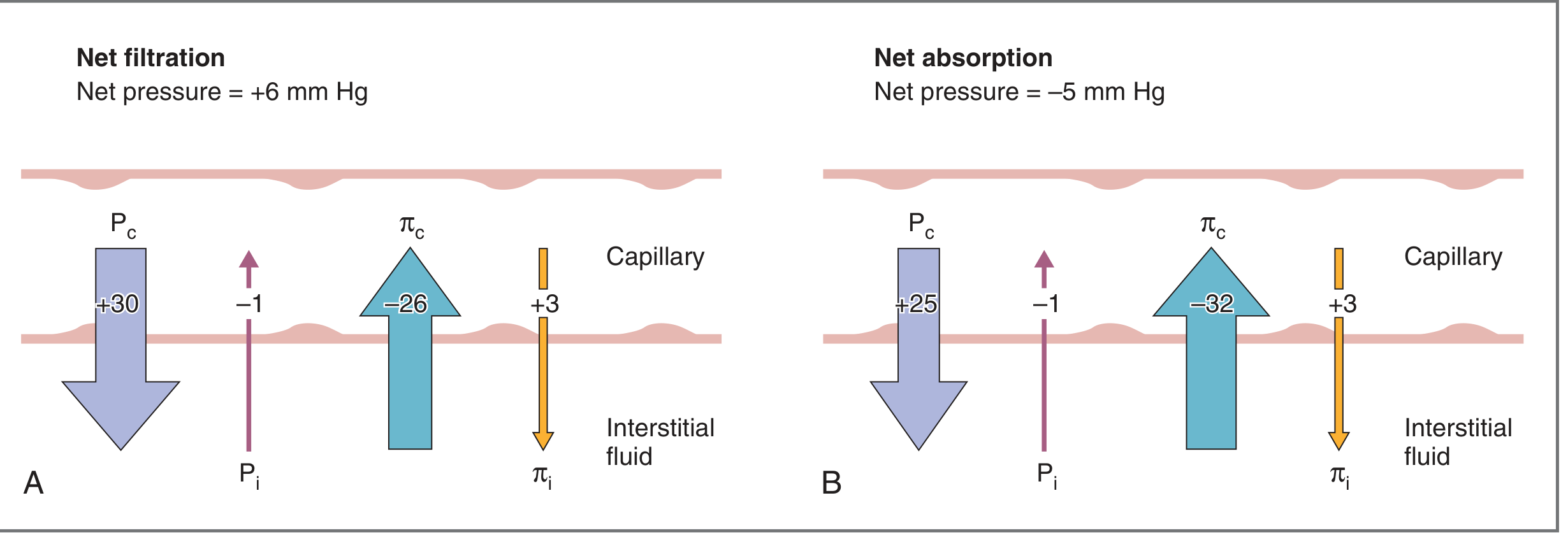
Net pressure = +Pc - Pi - πc + πi = +30 - 1 - 26 + 3 = +6 mmHg → Filtration
= +25 - 1 - 32 + 3 = -5 mmHg → Absorption
= 0.5 mL/min per mmHg × 6 mmHg = 3 mL/min
Along the Length of a Capillary
ARTERIAL END VENOUS END
Pc = 35 mmHg (high) Pc = 15 mmHg (falls)
πc = 25 mmHg πc = 28 mmHg (rises as water leaves)
Net = Filtration ➕ Net = Absorption ➖
- At arterial end → Net filtration (Pc > πc)
- At venous end → Net absorption (πc > Pc)
- Not all filtered fluid is reabsorbed → excess drained by lymphatics (~2-4 L/day)
Kf (Hydraulic Conductance / Filtration Coefficient)
- = water permeability × surface area of capillary
- Highest: Glomerular capillaries (explains high GFR = 125 mL/min)
- Lowest: Cerebral capillaries (blood-brain barrier)
- Increased by: Capillary injury, burns, toxins, inflammation
- NOT affected by: arteriolar resistance, hypoxia, metabolites
Causes of Oedema
Oedema = excess interstitial fluid when filtration > lymphatic return
| Cause | Mechanism | Example |
|---|---|---|
| ↑ Pc | Venous/arterial pressure rises | CCF, DVT, pregnancy |
| ↓ πc | Low plasma proteins | Nephrotic syndrome, cirrhosis, malnutrition, burns |
| ↑ Kf | Capillary wall damage | Inflammation, sepsis, anaphylaxis |
| Lymphatic obstruction | Drainage impaired | Filariasis, post-mastectomy |
| ↑ πi | Protein leaks into interstitium | Capillary injury |
Important Points for Exam ✅
- Pc is the main force for filtration; πc is the main force for absorption
- Albumin accounts for ~80% of plasma oncotic pressure
- Small molecules (Na+, glucose) do NOT generate effective osmotic pressure across capillaries - they equilibrate on both sides
- Venous pressure affects Pc more than arterial pressure does
- Lymphatics return ~2-4 L/day of excess filtered fluid
- Inflammation → ↑ Kf + protein leaks out → both ↑ filtration and ↑ πi → pitting oedema
- Glomerular filtration uses the same Starling principle, with Pgc = 45 mmHg (much higher than systemic capillaries)