Treatment modalities and selection of restorative materials for subgingivally placed restorations notes picture
subgingival restorations treatment modalities restorative material selection dentistry
https://www.biomimeticstudyclub.com/blog/treatment-approache…
deep margin elevation subgingival restoration gingivectomy crown lengthening orthodontic extrusion material selection
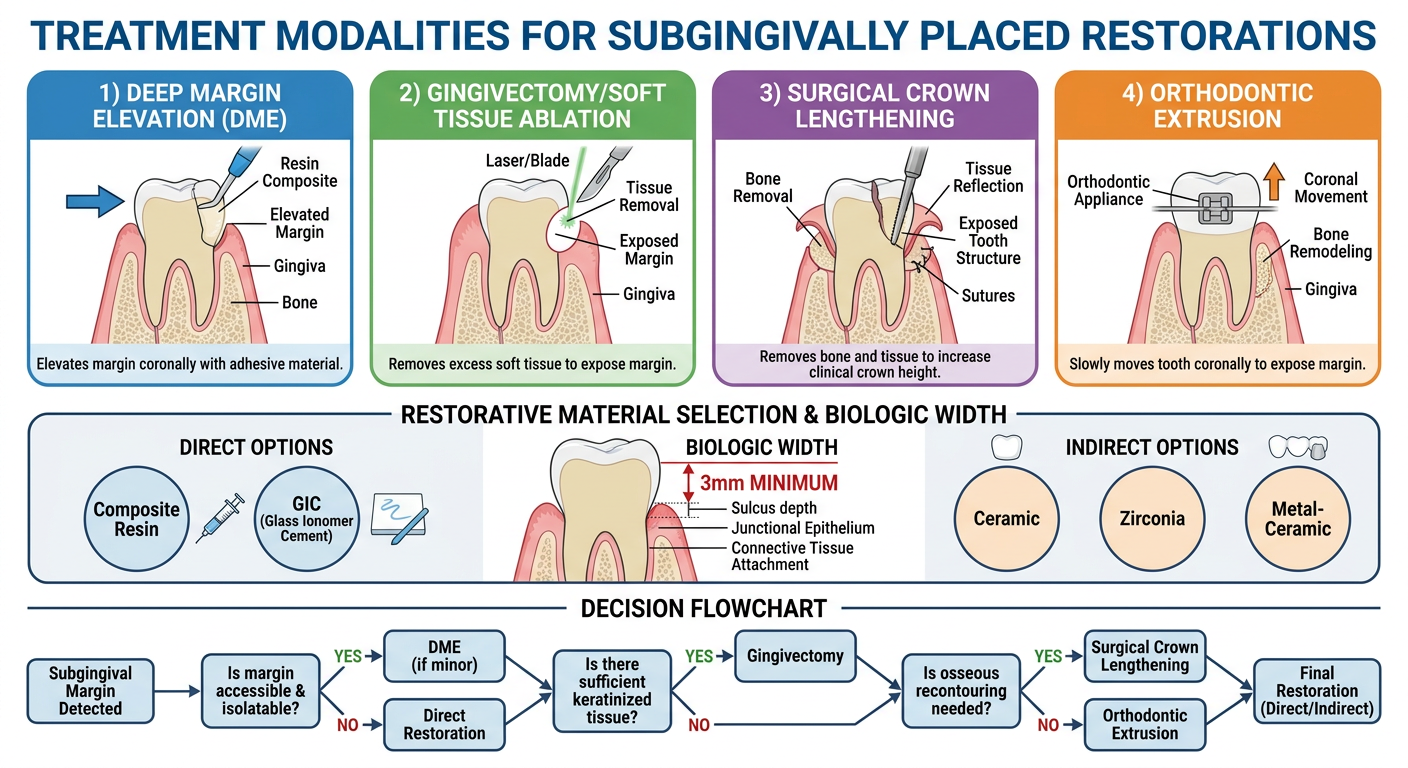
A comprehensive dental education diagram titled "Treatment Modalities for Subgingivally Placed Restorations" showing four main treatment approaches: 1) Deep Margin Elevation (DME) with resin composite elevating margin coronally, 2) Gingivectomy/Soft Tissue Ablation showing tissue removal with laser or blade, 3) Surgical Crown Lengthening showing bone and tissue removal to expose tooth structure, 4) Orthodontic Extrusion showing tooth being moved coronally. Include a section on restorative material selection showing direct (composite resin, GIC) and indirect (ceramic, zirconia, metal-ceramic) options with biologic width diagram showing 3mm minimum from bone to margin. Use clean medical illustration style with clear labels, arrows, and color coding. Include a decision flowchart at the bottom.
https://www.biomimeticstudyclub.com/blog/treatment-approache…
Treatment Modalities & Restorative Material Selection for Subgingivally Placed Restorations
Why Subgingival Margins Are Problematic
- Difficult isolation (moisture contamination compromises bonding)
- Inaccessibility for impression-taking and cementation
- Risk of violating the Supracrestal Tissue Attachment (STA) - formerly "biologic width" - leading to chronic inflammation, bone loss, and recession
- Bacterial biofilm accumulation causing periodontal breakdown
Key Rule: A minimum of 3 mm of sound tooth structure must exist between the alveolar crest and the final restoration margin to preserve the STA (junctional epithelium ~1 mm + connective tissue ~1 mm + sulcus ~1 mm).
Treatment Modalities
1. Deep Margin Elevation (DME) - Also Called Cervical Margin Relocation
- First described by Dietschi & Spreafico (1998); popularized by Magne & Spreafico (2012)
- Minimally invasive - no surgery, no bone removal
- Goal: relocate the adhesive interface to a dry, visible, accessible zone
- Subgingival caries or old restoration where isolation IS achievable
- Deep proximal boxes for onlays/inlays
- Reinforcing undermined cusps, sealing dentin, filling undercuts
- Rubber dam isolation with appropriate clamp
- Sectional matrix with wedge + Teflon tape for cervical seal (specialized matrices: Reel Matrix by Garrison)
- Soft tissue retraction using cord, wedges, light-cured rubber dam, Teflon tape
- Adhesive composite resin placed incrementally to elevate margin
- Final preparation now with supragingival/equigingival finish line
- Indirect restoration fabricated and cemented normally
2. Gingivectomy / Soft Tissue Ablation
- Scalpel/blade (traditional)
- Laser (diode, Nd:YAG, Er:YAG)
- Electrosurgery
- Soft tissue burs
- Cannot be used when bone removal is also needed
- Risk of STA violation if done too aggressively
- Contraindicated in thin biotype (recession risk)
- Wait 4-8 weeks post-surgery for tissue stabilization before final restoration
3. Surgical Crown Lengthening (SCL)
- When isolation for DME is not possible
- Contraindication to gingivectomy alone
- Subgingival crown fractures
- Increasing the ferrule effect (target: 1.5-2.0 mm of sound tooth structure above the finish line, 360 degrees)
- When DME would still violate STA
4. Orthodontic Extrusion (Forced Eruption)
- Subgingival fractures or deep caries where SCL would compromise crown-to-root ratio
- When preservation of bone is critical (esthetic zone)
- Where the extrusion margin migration avoids need for surgery
- Requires fibrotomy (fiberotomy) during extrusion to prevent soft tissue following the tooth
- May need retention period post-extrusion
- Time-consuming (weeks to months)
- Invasive in terms of treatment duration
Summary Comparison Table
| Modality | Invasiveness | Time | Bone Loss | Best For |
|---|---|---|---|---|
| Deep Margin Elevation (DME) | Minimal | Fast | None | Isolatable subgingival margins, indirect restorations |
| Gingivectomy | Mild | Fast | None | Pseudo-pockets, no STA violation |
| Surgical Crown Lengthening | High | Moderate | Yes | Deep margins, ferrule needs, failed isolation |
| Orthodontic Extrusion | Moderate | Slow (weeks-months) | None | Subgingival fractures, esthetic zone, poor ferrule |
Selection of Restorative Materials for Subgingival Restorations
A. Direct Restorations
1. Resin Composite (Material of Choice for DME)
- Preferred material for deep margin elevation
- Nanohybrid or bulk-fill composites (e.g., Filtek Z250, Tetric EvoCeram, Estelite Sigma Quick)
- Preheated composite improves flow and adaptation at deep margins
- Closed Sandwich Technique: thin RMGI liner/base over deep dentin (hydrophilic seal) + nanohybrid composite for margin elevation
- Requires strict adhesive protocol and rubber dam isolation
- Provides good marginal integrity, dentin sealing, cusp reinforcement
- High polish achievable - important as smooth margins reduce biofilm accumulation
2. Resin-Modified Glass Ionomer Cement (RMGI)
- Used as a liner/base in the closed sandwich technique
- Hydrophilic - tolerates slight moisture
- Chemical bond to dentin
- Good for deep, sclerotic dentin where adhesive bonding is less reliable
- Fluoride release - cariostatic benefit
3. Conventional Glass Ionomer Cement (GIC)
- Moisture-tolerant - can be used more easily in subgingival environments
- Suitable as a base or for temporary/interim restorations
- Used with indirect non-bonded restorations (conventional cementation approach)
- Less technique-sensitive than composites subgingivally
- Lower strength than composite; not ideal as a final esthetic restoration
B. Indirect Restorations (After Margin Management)
1. Ceramic Restorations (Lithium Disilicate, Zirconia)
- Preferred for posterior teeth requiring full/partial coverage
- Lithium disilicate (e.g., IPS e.max): good strength (400 MPa), excellent esthetics, can be adhesively cemented
- Zirconia: highest strength (>1000 MPa), ideal for high-load posterior areas, opaque
- Require dry, accessible margins for adhesive cementation - this is exactly why DME or SCL is done first
2. Metal-Ceramic (PFM) Restorations
- Suitable where esthetics is secondary and strength is needed
- Can be cemented with conventional cements (zinc phosphate, GIC) - more moisture-tolerant
- Less demanding of perfect subgingival isolation for cementation
3. Full-Metal Restorations (Cast Gold/Alloy)
- Most biologically inert and most tolerated by periodontal tissues
- Can be conventionally cemented
- Poor esthetics but excellent long-term durability
- Ideal for posterior teeth with subgingival margins where perfect isolation is difficult
Periodontal Response to Restorative Materials
| Material | Periodontal Response |
|---|---|
| Gold/metal alloys | Most biocompatible, minimal inflammation |
| Glazed ceramics | Very good, smooth surface reduces biofilm |
| Polished composite | Acceptable if well-adapted and smooth |
| Unpolished composite | Significant biofilm retention, inflammation |
| Amalgam | Moderate; corrosion products may irritate tissue |
| GIC/RMGI | Good; fluoride release may be beneficial |
Key principle: Surface smoothness and marginal fit are more important than material composition in determining the periodontal response to subgingival restorations.
Decision Algorithm
Deep subgingival margin identified
|
Can you isolate? (Rubber dam possible?)
/ \
YES NO
| |
DME Assess STA violation?
(preferred) / \
Violating STA Not violating STA
| |
Need bone? Gingivectomy
/ \
YES NO
| |
SCL Gingivectomy
If poor crown-root ratio after SCL → consider Orthodontic Extrusion instead
Clinical Pearls
- 0.5 mm subgingival margin is manageable; >1.5 mm creates major complications, especially for bonded cementation
- Biologic width/STA = 3 mm from alveolar crest; NEVER violate this zone
- For indirect bonded restorations (onlays, endocrowns), margin elevation is mandatory for predictable adhesion - you cannot bond with matrices and wedges in the way
- Smooth, gap-free composite margins are tolerated without significant periodontal inflammation (supported by histological evidence)
- After any surgical procedure (SCL or gingivectomy), wait 4-8 weeks for tissue stabilization before taking final impressions
- After orthodontic extrusion, a retention/fibrotomy period is required before restoration