Adult Brachial plexus injury classification signs symptoms clinical examination investigation evaluation treatment explain neuroraphy nerve transport neurotization these in detail with appropriate illustrative diagrams rehabilitation and post op protocol for all
Reading File
Finding Sources
Finding Sources
Searching Images
brachial plexus anatomy diagram injury classification
Reading File
Reading File
Searching Images
neurorrhaphy nerve graft neurotization transfer brachial plexus surgery
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Searching the Web
brachial plexus injury adult classification treatment neurorrhaphy nerve graft neurotization rehabilitation protocol 2024
Searching Images
brachial plexus Seddon Sunderland classification nerve injury grading diagram
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Adult Brachial Plexus Injury — Comprehensive Review
1. ANATOMY
The brachial plexus arises from the anterior rami of C5–T1 and is organized into five sequential segments: Roots → Trunks → Divisions → Cords → Branches (mnemonic: Robert Taylor Drinks Cold Beer).
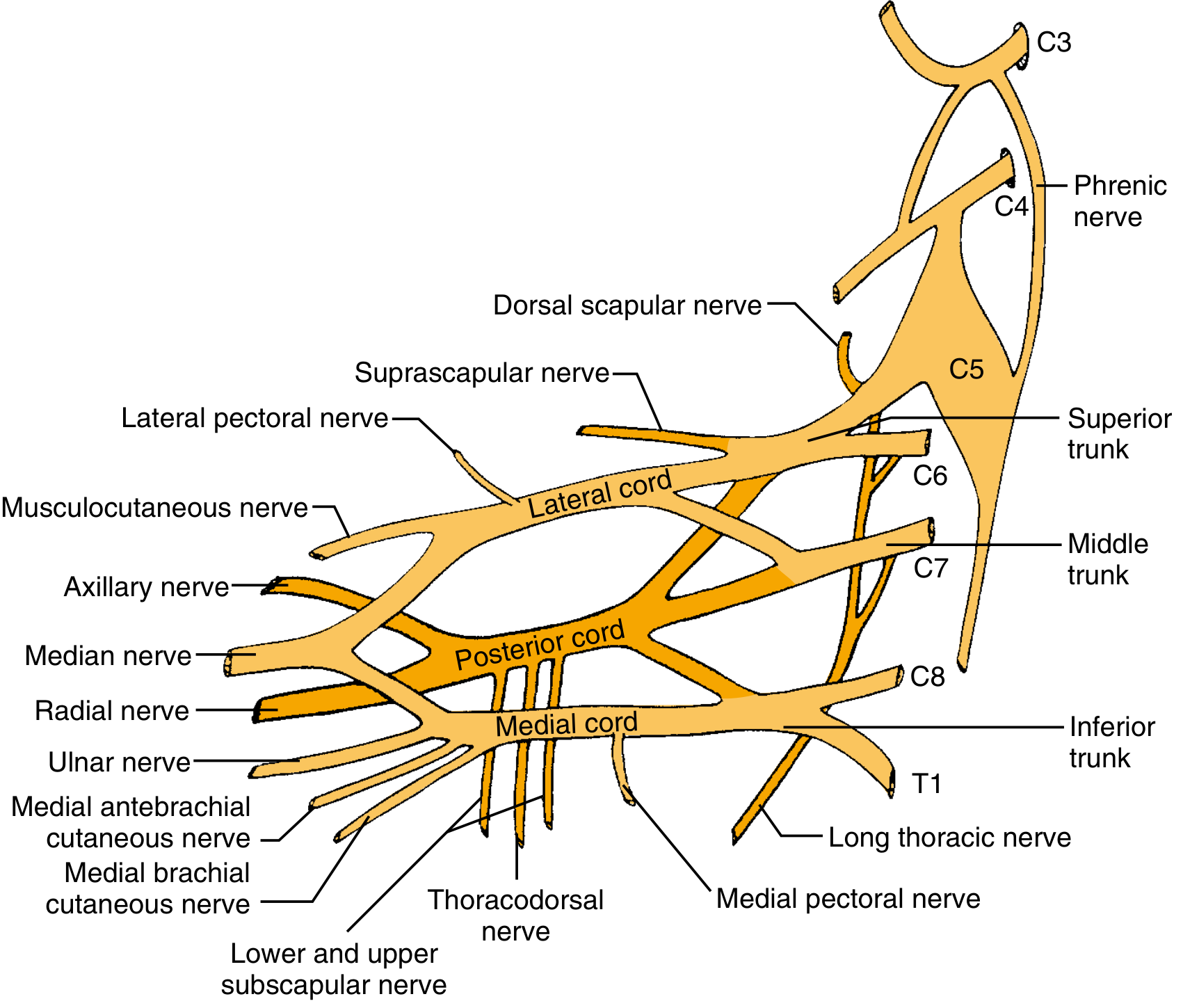
Topographic relationship to clavicle:
- Supraclavicular = roots + trunks (higher energy, worse prognosis)
- Infraclavicular = divisions + cords + branches
2. CLASSIFICATION OF NERVE INJURY
2A. Seddon Classification (3 classes)
| Seddon | Lesion | Wallerian Degeneration | Recovery |
|---|---|---|---|
| Neurapraxia | Focal demyelination, axon intact | None | Complete; days–6 weeks |
| Axonotmesis | Axon disrupted, connective tissue intact | Yes | Slow (1 mm/day); usually complete |
| Neurotmesis | Complete nerve transection | Yes | No spontaneous recovery; surgery required |
2B. Sunderland Classification (5 degrees) — More granular
| Sunderland | Structure Injured | Prognosis | Seddon Equivalent |
|---|---|---|---|
| 1st degree | Myelin only | Full recovery in days–weeks | Neurapraxia |
| 2nd degree | Axon (endoneurium intact) | Full recovery, weeks–months | Axonotmesis |
| 3rd degree | Axon + endoneurium | Incomplete recovery (misrouting) | Axonotmesis |
| 4th degree | Axon + endoneurium + perineurium | Neuroma-in-continuity; no spontaneous recovery | Axonotmesis |
| 5th degree | Complete trunk transection | No recovery without surgery | Neurotmesis |
| 6th degree (Mackinnon) | Mixed — combination pattern | Variable; represents most clinical injuries | — |
Key concept: Axon regenerates at ~1 mm/day (≈1 inch/month). Motor endplates degenerate irreversibly at 12–18 months → creates a surgical deadline for motor recovery.
2C. Topographic Classification
| Location | Level | Features |
|---|---|---|
| Preganglionic | Proximal to DRG (root avulsion) | Worst prognosis; no proximal stump available |
| Postganglionic | Distal to DRG | Surgical repair/grafting possible |
| Supraclavicular | Roots + trunks | High-energy; often preganglionic |
| Infraclavicular | Cords + branches | Better prognosis; isolated nerve injury |
3. MECHANISMS AND COMMON INJURY PATTERNS
Adult mechanisms (in order of frequency):
- Motorcycle/motor vehicle accidents (most common — violent traction)
- Penetrating trauma (stab, GSW, iatrogenic)
- Stretch injuries ("burners/stingers" in athletes)
- Scapulothoracic dissociation
Pattern frequencies:
- C5–C6 (upper trunk): 15%
- C5–C7: 20–35%
- C8–T1 (lower trunk): 10%
- Pan-plexus (complete): 50–75% in high-energy trauma
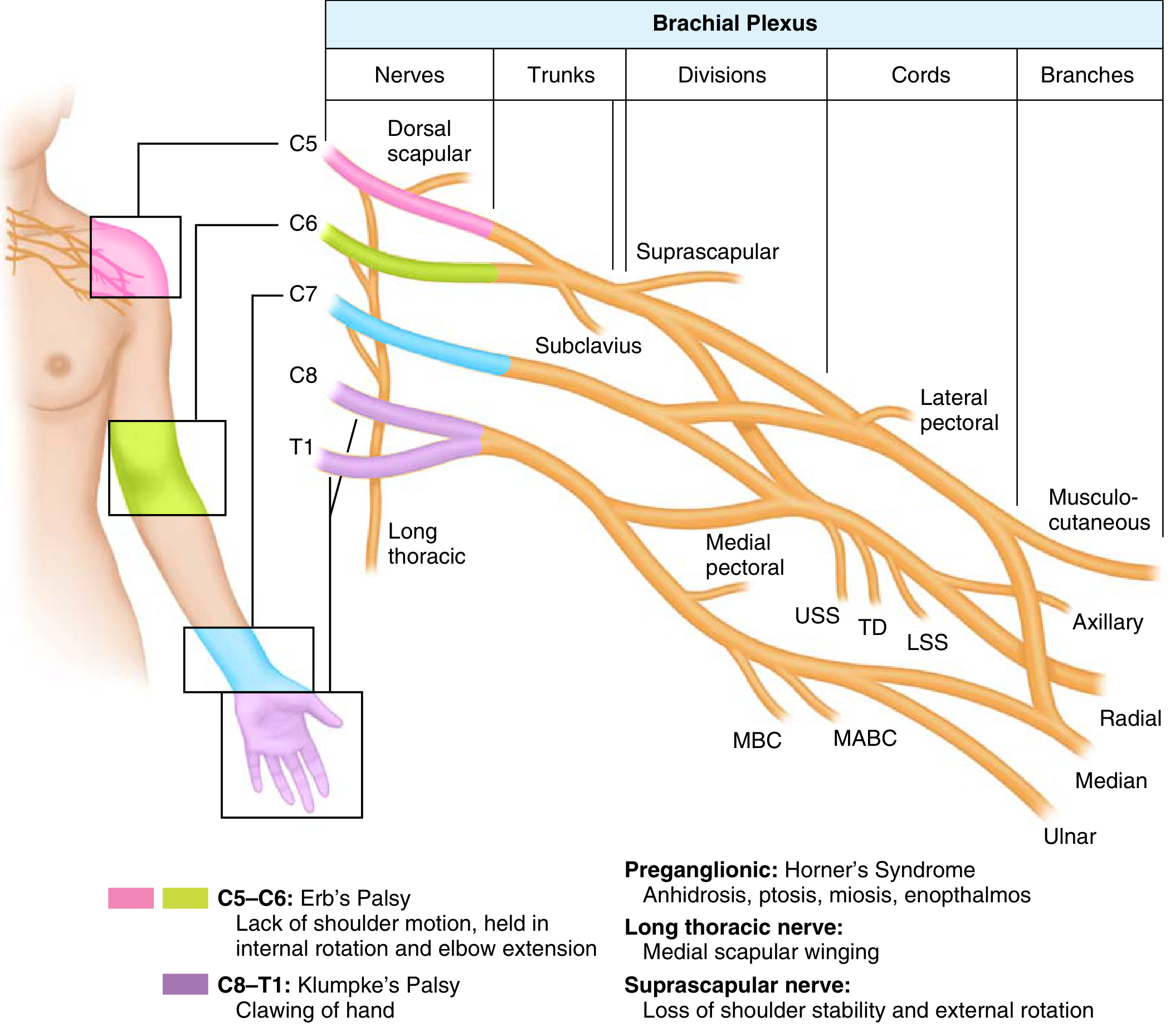
4. SIGNS & SYMPTOMS
4A. Upper Plexus Injury — Erb's Palsy (C5–C6)
- "Waiter's tip" posture: arm adducted, internally rotated, elbow extended, forearm pronated
- Loss of: shoulder abduction/external rotation, elbow flexion, forearm supination
- Sensory loss: lateral arm, forearm, thumb
- Deltoid, biceps, brachioradialis, supraspinatus, infraspinatus weakness
4B. Middle Trunk (C7)
- Weak wrist/finger extension
- Triceps weakness
- Sensory loss: middle finger
4C. Lower Plexus Injury — Klumpke's Palsy (C8–T1)
- Clawing of the hand (intrinsic minus)
- Loss of: hand grip, intrinsic hand muscles, wrist/finger flexors
- Sensory loss: medial forearm and hand (ulnar distribution)
- Horner syndrome if T1 preganglionic (ptosis, miosis, anhidrosis, enophthalmos)
4D. Pan-Plexus Injury (C5–T1)
- Flail, anesthetic upper limb
- Complete motor paralysis shoulder → hand
- Pain is common (especially with root avulsions — neuropathic/deafferentation pain)
5. SIGNS OF PREGANGLIONIC INJURY (Root Avulsion)
These indicate the injury is proximal to the DRG — no distal nerve stump for direct repair:
| Sign | Mechanism |
|---|---|
| Horner syndrome | Sympathetic chain (T1) involvement |
| Winged scapula | Long thoracic nerve (serratus anterior) |
| Rhomboid weakness | Dorsal scapular nerve (C5) |
| Elevated hemidiaphragm | Phrenic nerve (C3–C5) |
| Normal SNAPs with sensory loss | Cell bodies (DRG) intact, distal segment viable |
| Absent SSEPs | No continuity to spinal cord |
| Paraspinal EMG denervation | Posterior rami injured at root level |
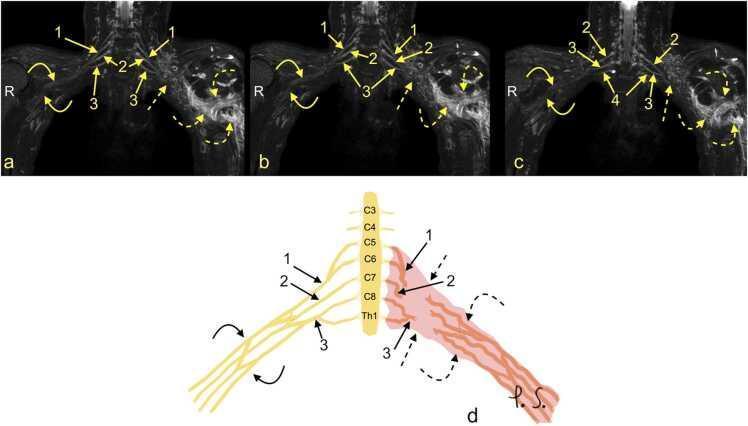
| Pseudomeningocele on MRI | CSF leak at avulsed root sleeve |
6. CLINICAL EXAMINATION
History
- Mechanism (high vs. low energy)
- Associated injuries (vascular — axillary/subclavian; fractures — clavicle, scapula, rib, cervical spine; pneumothorax)
- Time from injury
- Dominant hand, occupation, patient age
Physical Examination — Systematic Approach
Inspection:
- Posture of arm (Erb's tip vs. clawing)
- Muscle wasting (particularly deltoid, thenar, hypothenar)
- Scapular winging
Sensory Testing (dermatomal mapping):
| Root | Territory |
|---|---|
| C5 | Lateral arm (regimental badge area) |
| C6 | Lateral forearm, thumb, index |
| C7 | Middle finger |
| C8 | Ring, little finger |
| T1 | Medial forearm |
Motor Testing (MRC grading 0–5):
| Function | Root | Nerve |
|---|---|---|
| Shoulder abduction | C5 | Axillary → deltoid |
| Elbow flexion | C5–C6 | Musculocutaneous → biceps |
| Wrist extension | C6–C7 | Radial |
| Wrist flexion | C7–C8 | Median/ulnar |
| Finger extension | C7 | PIN (radial) |
| Finger abduction | T1 | Ulnar → interossei |
| Thumb opposition | T1 | Median → thenar |
Reflexes: Biceps (C5–C6), Brachioradialis (C6), Triceps (C7)
Tinel sign: Advancing Tinel over the nerve trunk is the most reliable clinical sign of nerve regeneration.
Vascular Assessment: Axillary/brachial pulses; bruit; expanding hematoma (subclavian/axillary artery injury accompanies ~30% of complete plexus injuries)
7. INVESTIGATIONS & EVALUATION
Imaging
Plain Radiographs (baseline series):
- Cervical spine: transverse process fractures → suggest root avulsion
- Chest PA + lateral: hemidiaphragm elevation → phrenic nerve injury
- Inspiratory/expiratory CXR: paradoxical diaphragm movement
- Shoulder + clavicle: fractures, scapulothoracic dissociation
CT Myelography (gold standard for root avulsion):
- Demonstrates pseudomeningocele at avulsed root sleeve
- Detects intradural root injury
- Still preferred over MRI in many centres for avulsion
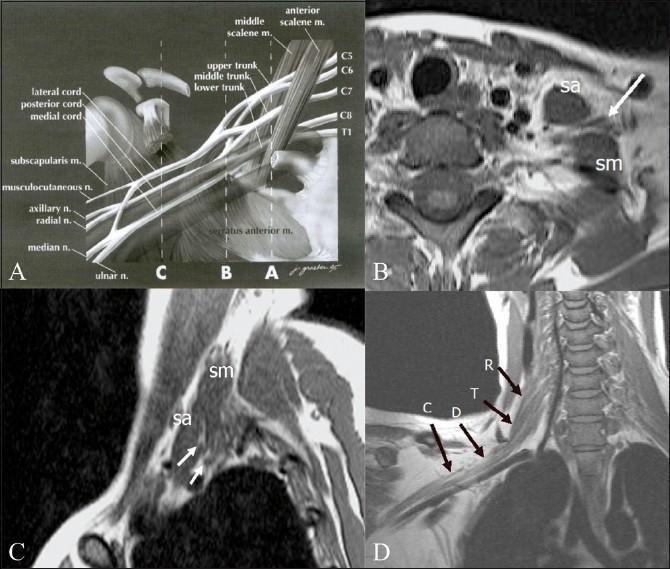
MRI/MR Neurography:
- Demonstrates: peripheral neuroma, pseudomeningocele, nerve edema (STIR hyperintensity), fascicular discontinuity
- Differentiates preganglionic vs. postganglionic injury
- Preferred for infraclavicular lesions and cord/branch-level injury
Electrodiagnostics
Timing: Must be performed ≥4–6 weeks after injury (Wallerian degeneration must be complete).
| Test | Findings | Interpretation |
|---|---|---|
| EMG — fibrillation potentials | Denervation in affected muscles | Confirms axonal loss |
| EMG — paraspinal muscles | Denervation | Preganglionic (root avulsion) |
| SNAPs (sensory nerve action potentials) | Normal SNAP + sensory loss on exam | Preganglionic injury (DRG intact) |
| Motor NCS | Absent/reduced CMAP | Axonal loss |
| Intraoperative NAP (nerve action potential) | Positive = viable axons crossing lesion | Neurolysis sufficient; negative = resection + graft |
| SSEPs (somatosensory evoked potentials) | Absent = no continuity to cord | Preganglionic avulsion |
8. TREATMENT
8A. Decision Framework
INJURY
├── Penetrating / sharp laceration → Immediate exploration (within 72 hours)
├── Vascular injury requiring repair → Simultaneous nerve exploration
├── Progressive neurologic deficit → Urgent surgery
├── Closed traction injury
│ ├── High-energy + complete → Surgery 3–12 weeks
│ ├── Low-energy + incomplete → Observe 3 months; surgery if plateau
│ └── Gunshot wound → Observe; most recover without surgery
└── Beyond 6 months → Less predictable nerve repair outcome
"3+1 Rule" of Surgical Timing:
- Early: <3 days — sharp transection, vascular compression
- Subacute: ~3 weeks — ragged lacerations (propeller, chainsaw)
- Delayed: 3–6 months — closed injuries with no recovery
- Late: >1 year — tendon/muscle transfer (nerve repair no longer viable)
Priorities of reconstruction:
- Elbow flexion (most functionally critical)
- Shoulder stability and abduction/external rotation
- Wrist/finger flexion (hand sensation)
- Finger extension
- Hand intrinsics (last priority, poorest outcome)
8B. NEURORRHAPHY (Primary Nerve Repair)
Definition: Direct surgical coaptation (suturing) of transected nerve ends without tension.
Technique:
- Preparation: Debride nerve ends sequentially until healthy, bleeding fascicles appear (no gap, no tension)
- Alignment: Align epineurial blood vessels as topographic landmarks
- Epineural repair: 8-0, 9-0, or 10-0 monofilament nylon interrupted sutures through epineurium — most common technique
- Grouped fascicular repair: Additional internal epineurial sutures between identifiable fascicular groups — reserved for large nerves with clear fascicular topography
- Tension-free: Critical; tension causes ischemia, scarring, failed regeneration
Indications:
- Sharp laceration with minimal zone of injury
- Short gap after neuroma-in-continuity resection
- Must be tension-free
Intraoperative NAP: If positive → neurolysis only (do not resect). If negative → resect and graft.
8C. NERVE GRAFTING (Cable/Interpositional Graft)
Indication: When direct repair is impossible without tension; gaps >1–2 cm in mixed nerves.
Principle: Reversed autologous nerve graft bridges the defect. "Reversed" direction ensures axons grow through graft without escaping through side branches.
Graft Sources:
| Donor Nerve | Length Available | Notes |
|---|---|---|
| Sural nerve (gold standard) | 30–40 cm | Sensory deficit lateral foot; most common |
| Medial antebrachial cutaneous | 15–20 cm | Same operative field as plexus |
| Lateral antebrachial cutaneous | 8–10 cm | — |
| Medial brachial cutaneous | 8–10 cm | — |
| Great auricular nerve | 5–8 cm | Neck dissection approach |
| Superficial radial nerve (sensory branch) | 15 cm | — |
Cable grafting technique: Multiple sural nerve segments placed in parallel ("cables") to match the diameter of the recipient nerve.
Vascularized nerve graft: Used for large gap reconstruction in scarred beds — ulnar nerve on its vascular pedicle is the classical example. Reduces central graft necrosis.
8D. NEUROTIZATION (Nerve Transfer)
Neurotization is the transfer of a functioning expendable nerve (or fascicle) to reinnervate a denervated target closer to the muscle, bypassing a proximal irreparable injury.
Advantages over proximal nerve grafting:
- Coaptation is closer to target muscle → shorter regeneration distance → faster recovery
- Distal nerve contains purer motor or sensory fascicles
- Essential when no proximal stump exists (avulsion)
Types:
- Intraplexal (intra-extraplexal) — donor from within the plexus
- Extraplexal — donor from entirely outside the plexus (cranial nerves, intercostals, phrenic, contralateral C7)
KEY NEUROTIZATION PROCEDURES
A. Oberlin Transfer (Modified Oberlin = "Double Fascicular Transfer")
- Donor: Ulnar nerve fascicle to FCU (± median nerve fascicle to FDS)
- Recipient: Musculocutaneous nerve → biceps motor branch (± brachialis branch)
- Purpose: Elbow flexion
- Approach: Medial arm incision
- Outcome: ~90% M3+ biceps recovery; gold standard for C5–C6 injury

B. Spinal Accessory (CN XI) → Suprascapular Nerve
- Purpose: Shoulder abduction + external rotation
- Donor: Descending branch of CN XI (spinal accessory)
- Recipient: Suprascapular nerve
- Outcome: ~70% regain useful shoulder abduction (MRC ≥3)
- Can be performed via dorsal (posterior) or anterior approach
C. Leechavengvong Procedure (Radial Nerve Triceps Branch → Axillary Nerve)
- Donor: Motor branch of radial nerve to long/medial head of triceps
- Recipient: Axillary nerve (anterior branch → deltoid)
- Purpose: Shoulder abduction and forward elevation
- Triceps function is maintained because redundant branches are used
D. Intercostal Nerve Transfer
- Donor: 3rd–5th intercostal nerves (motor branches)
- Recipient: Musculocutaneous nerve (elbow flexion) or nerve to chest free muscle flap
- Purpose: Elbow flexion; useful when ulnar/median nerve not available
- Requires patient to practice breathing movements to activate biceps initially
- Can provide 3–4 intercostal nerves; each contributes ~1,000–1,500 motor axons
E. Phrenic Nerve Transfer
- Donor: Phrenic nerve (C3–C5)
- Recipient: Suprascapular nerve or musculocutaneous nerve
- Purpose: Shoulder/elbow function in pan-avulsion
- Caution: Assess pulmonary function first; sacrifice causes hemidiaphragm paralysis
F. Contralateral C7 Transfer
- Donor: Contralateral C7 root (entire or posterior division)
- Recipient: Injured plexus (via sural nerve graft tunneled across midline)
- Purpose: Pan-plexus avulsion — restore wrist/finger flexion or extension
- Most axon-rich transfer (>18,000 axons in C7)
- Transient ipsilateral donor-side deficits; usually recover within months
- Used in total avulsion when no ipsilateral donors available
G. Free Functioning Muscle Transfer (FFMT)
- For late presentations (>12–18 months) when target muscles are fibrotic
- Gracilis muscle most commonly used
- Transferred with its vascular pedicle (anastomosed to thoracodorsal or serratus vessels)
- Neurotized directly by donor nerve (intercostal, spinal accessory, contralateral C7)
- Restores elbow flexion or finger flexion in selected cases
Summary Table — Common Nerve Transfers
| Procedure | Donor | Recipient | Function Restored |
|---|---|---|---|
| Oberlin | Ulnar fascicle (FCU) ± median fascicle (FDS) | Musculocutaneous → biceps ± brachialis | Elbow flexion |
| CN XI → suprascapular | Spinal accessory (descending br.) | Suprascapular nerve | Shoulder abduction + ER |
| Leechavengvong | Radial → triceps br. | Axillary nerve (ant. br.) | Shoulder abduction |
| Intercostal (3–4 nerves) | Intercostal motor branches | Musculocutaneous nerve | Elbow flexion |
| Phrenic | Phrenic nerve | Suprascapular / musculocutaneous | Shoulder / elbow |
| Contralateral C7 | Contralateral C7 root | Injured plexus (via graft) | Wrist/finger flexion |
8E. NEUROLYSIS
- External neurolysis: Release of nerve from surrounding scar tissue; preserves internal architecture
- Internal neurolysis: Separation of fascicles within nerve; controversial — may increase intraneural scarring
- Indication: Neuroma-in-continuity with positive intraoperative NAP (viable axons crossing) → neurolysis only; do not resect
8F. TENDON AND MUSCLE TRANSFERS
Indicated when nerve repair/reconstruction has failed or is no longer feasible (>12 months denervation without recovery):
- Elbow flexion: Latissimus dorsi/pectoralis minor transfer, Steindler flexorplasty, free gracilis FFMT
- Shoulder stabilization: Trapezius transfer, glenohumeral fusion (arthrodesis)
- Wrist extension: BR to ECRB; ECU to ECRB
- Isolated C8–T1 injury: early tendon transfers preferred (too distal for nerve repair to succeed in time)
9. INVESTIGATION–GUIDED DECISION PATHWAY
Supraclavicular injury
↓
EMG/NCS at 4–6 weeks (baseline)
↓
Horner's + paraspinal denervation + normal SNAPs
→ Preganglionic avulsion
→ CT myelography / MRI for pseudomeningocele
→ Nerve transfer (neurotization) — no direct repair possible
↓
No signs of avulsion + recovery plateau at 3 months
→ Explore; intraoperative NAP
├── NAP positive → Neurolysis
└── NAP negative → Resect + Cable graft / Nerve transfer
10. REHABILITATION & POST-OPERATIVE PROTOCOLS
10A. Pre-Operative Rehabilitation
- Goal: Prevent contractures, maintain passive ROM, protect denervated skin
- Gentle passive ROM exercises for all joints from day 1
- Resting splints in functional position (wrist neutral, MCP 70° flexion, IP extended)
- Patient and family education on skin protection (denervated skin insensate to heat/pressure)
- Pain management: gabapentin/pregabalin for neuropathic pain
10B. Acute Post-Operative Phase (0–6 weeks)
After Nerve Repair / Neurorrhaphy:
- Immobilization for 3 weeks in position of least tension (shoulder in slight adduction; elbow at ~90° flexion if upper plexus)
- Gradual mobilization from week 3 (avoid sudden passive stretching)
- Edema management: compression garments, elevation
- Wound care and scar management after 6 weeks
After Nerve Graft:
- Similar immobilization to direct repair
- No neuromuscular re-education needed in initial phase
- Focus on passive ROM maintenance
After Nerve Transfer (Neurotization):
- Immobilization typically minimal (coaptation under no tension)
- Crucial difference: The patient must learn to use a new cortical movement pattern to activate the donor nerve
- E.g., after Oberlin transfer, patient must squeeze hand (ulnar activation) to contract biceps initially
10C. Regeneration Phase (6 weeks – 6 months)
Timeline of expected recovery: Nerve regeneration ≈ 1 mm/day → recovery time = distance from repair to muscle ÷ 1 mm/day + 3-month maturation period.
- Serial clinical examinations every 6–8 weeks tracking advancing Tinel sign
- EMG monitoring at 3, 6, 9, 12 months
- Gravity-eliminated active-assisted ROM when first voluntary contraction detected
- Progressive gravity-resisted strengthening once MRC grade 2 achieved
- Neuromuscular re-education:
- Biofeedback EMG: Electrode on target muscle; audio/visual feedback for activation
- NMES (Neuromuscular electrical stimulation): Activate weakly recovering muscle; may enhance motor end plate maintenance
- Mental imagery and cortical remapping (especially after nerve transfer)
10D. Motor Re-Education for Nerve Transfers
This is the most critical and unique rehabilitation aspect:
| Transfer | Donor Movement | New Target | Re-education Cue |
|---|---|---|---|
| Oberlin (ulnar→biceps) | Wrist ulnar deviation / finger flexion | Elbow flexion | "Squeeze your fingers, think about bending your elbow" |
| CN XI → suprascapular | Shrug shoulders (trapezius) | Shoulder abduction | Mirror therapy: "Shrug while lifting arm" |
| Intercostal → musculocutaneous | Deep inhalation | Elbow flexion | "Take a deep breath while trying to flex your elbow" |
| Leechavengvong (triceps→axillary) | Elbow extension | Shoulder abduction | "Push down while raising your arm" |
Mirror therapy: Particularly useful for cortical remapping — patient observes normal limb performing desired movement while attempting with affected limb.
10E. Recovery Phase (6–18 months)
- Progressive resistance training
- Functional bimanual activities (occupational therapy)
- Work hardening / vocational rehabilitation
- Upper limb prosthetics assessment if reconstruction fails
- Splints tailored to residual deficits (cock-up wrist splint for wrist drop, dynamic MCP extension splint for intrinsic minus hand)
10F. Pain Management (Ongoing)
Root avulsions commonly cause severe neuropathic/deafferentation pain:
- First-line: Gabapentin, pregabalin, amitriptyline
- Opioids: short-term, titrated
- TENS (transcutaneous electrical nerve stimulation)
- DREZ (dorsal root entry zone) lesioning: surgical last resort for intractable avulsion pain
11. PROGNOSIS
| Factor | Good Prognosis | Poor Prognosis |
|---|---|---|
| Age | Young (<30 yrs) | Older adults |
| Injury type | Stretch, clean wound | Avulsion, crush, blast |
| Level | Infraclavicular | Supraclavicular (avulsion) |
| Time to surgery | <3 months | >6 months |
| Repair type | Direct (tension-free) | Delayed graft |
| Target muscle distance | Close (biceps) | Distal (intrinsics) |
Best outcomes are obtained in young patients treated with nerve transfer within 3 months of injury, particularly for elbow flexion restoration.
Quick Summary Chart
ADULT BRACHIAL PLEXUS INJURY
│
├── CLASSIFY
│ ├── Seddon: Neurapraxia / Axonotmesis / Neurotmesis
│ ├── Sunderland: Grades I–VI
│ └── Location: Pre/postganglionic; Supra/infraclavicular
│
├── DIAGNOSE
│ ├── Clinical: Motor/sensory mapping, Horner, Tinel, reflexes
│ ├── Imaging: CXR, CT myelography (avulsion), MR neurography
│ └── EDX: EMG + NCS + SSEPs at 4–6 weeks
│
├── TREAT (Timing-driven)
│ ├── <72 hrs: Sharp transection → Neurorrhaphy
│ ├── 3–12 weeks: High-energy closed → Exploration + NAP-guided resection + Graft
│ ├── 3–6 months: Plateau → Nerve transfer / neurotization
│ └── >12 months: Tendon/muscle transfer; FFMT
│
└── REHABILITATE
├── Pre-op: ROM, splinting, education
├── Post-op 0–6 wks: Immobilize, edema control, passive ROM
├── 6 wks–6 months: Biofeedback, NMES, cortical re-education
└── 6–18 months: Strengthening, functional training, vocational rehab
Sources: Miller's Review of Orthopaedics 9th Ed. | Current Surgical Therapy 14e | Bradley and Daroff's Neurology in Clinical Practice | Grainger & Allison's Diagnostic Radiology | UCSF Brachial Plexus Program (2024) | Goubier et al., J Hand Surg Eur 2024
This is a shared conversation. Sign in to Orris to start your own chat.