Backache
Reading File
Asking for Preferences
Dd and management
Finding Sources
Searching PubMed
"low back pain"[MeSH Terms] AND "diagnosis" AND "management"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a full clinical overview of Backache (Low Back Pain) - Differential Diagnosis and Management, synthesized from Harrison's 22e, Bradley & Daroff's Neurology, and Firestein's Rheumatology.
Backache - Differential Diagnosis & Management
Epidemiology
60-80% of people experience back pain at some point in life. It is the most common reason for neurological consultation after headache. In up to 90% of cases, no definite anatomic or pathophysiologic diagnosis can be made (nonspecific LBP). Only <5% have an underlying serious systemic cause. - Bradley & Daroff's Neurology in Clinical Practice
Classification
| Type | Key Feature |
|---|---|
| Mechanical | Worsens with activity/upright posture; relieved by rest |
| Inflammatory | Morning stiffness >30 min; improves with exercise, not rest; worse at night (2nd half) |
| Referred | Non-spinal origin (visceral, vascular) |
| Neurogenic / Radicular | Pain radiates in dermatomal distribution with neurological signs |
Differential Diagnosis
1. Mechanical (>95% of LBP)
- Lumbosacral strain/sprain - most common cause overall; acute injury, paraspinal tenderness, muscle spasm; no neurological deficit
- Lumbar disc herniation - shooting/stabbing pain radiating down leg; L4-5 herniation: pain to dorsomedial foot; L5-S1 herniation: pain to lateral foot/small toe; positive straight leg raise (SLR); weakness of tibialis anterior (L5) or peroneus longus/brevis (S1)
- Lumbar facet joint syndrome - found in up to 35% of LBP cases; unilateral/bilateral low back pain radiating to thigh (not below knee); pain worsened by extension and lateral rotation; negative SLR; normal neurology
- Lumbar spinal stenosis - neurogenic claudication; bilateral leg pain/weakness with walking that is relieved by sitting/forward flexion (shopping cart sign); older patients
- Spondylolisthesis - anterior displacement of vertebral body (typically L5 on S1); may cause local or radicular pain
- Osteoporotic vertebral compression fracture - acute severe pain in post-menopausal woman; no preceding trauma
2. Inflammatory
- Spondyloarthritis (ankylosing spondylitis, PsA, reactive arthritis, IBD-associated) - age <40, insidious onset, morning stiffness >30 min, improves with exercise, alternating buttock pain, nocturnal pain in 2nd half of night; raised ESR/CRP, HLA-B27 positive
- Rheumatoid arthritis (less commonly causes LBP)
3. Infectious
- Vertebral osteomyelitis / discitis - fever, elevated inflammatory markers, palpation tenderness; night pain; often Staphylococcus aureus; requires antibiotics; MRI is investigation of choice
- Epidural abscess - spinal emergency; fever + back pain + neurological deficit
- Pott's disease (TB spine) - in endemic areas/immunocompromised
4. Neoplastic
- Metastatic disease (breast, lung, prostate, kidney, thyroid) - most common malignant cause; nocturnal pain not relieved by rest; history of malignancy; weight loss
- Primary spinal tumours (rare: meningioma, schwannoma, ependymoma)
- Multiple myeloma
5. Sacroiliac (SI) Joint Syndrome
- Unilateral low back/buttock pain radiating to hip or thigh; worsened climbing stairs; positive Patrick/FABER test; positive single-leg standing test - Bradley & Daroff's Neurology
6. Referred / Non-Spinal Causes
- Renal: pyelonephritis, nephrolithiasis (colicky, costovertebral angle tenderness)
- GI: peptic ulcer (penetrating), pancreatitis, retroperitoneal pathology
- Vascular: aortic aneurysm (pulsatile, expansile mass; vascular emergency)
- Gynaecological: endometriosis, uterine fibroids, ovarian pathology
- Prostate disease
7. Psychological / Biopsychosocial
- Chronic LBP has high co-prevalence with depression (33-67%), anxiety (10-30%), substance misuse (13-40%), and personality disorders (>50%). Psychosocial yellow flags (job dissatisfaction, disability claims, fear-avoidance) prolong chronicity. - Harrison's 22e
Red Flags (requiring urgent imaging - preferably MRI)
| Red Flag | Possible Cause |
|---|---|
| Fever + back pain + tenderness | Infection (osteomyelitis, epidural abscess) |
| Known malignancy / unexplained weight loss | Metastatic disease |
| Pain worsened in recumbent position / night pain | Neoplasm, infection |
| Bowel or bladder dysfunction | Cauda equina syndrome (surgical emergency) |
| Objective neurological deficit (weakness, sensory loss, reflex loss) | Cord or nerve root compression |
| Pain aggravated by Valsalva | Disc herniation, tumour |
| Back pain after significant trauma | Fracture |
| Age >50 / osteoporosis with acute severe pain | Vertebral compression fracture |
| Progressive worsening pain | Tumour, infection |
Note: Individual red flags have low sensitivity and specificity. The presence of multiple red flags significantly increases predictive value and should guide imaging decisions. - Firestein's Rheumatology
Investigations
| Investigation | Indication |
|---|---|
| Plain X-ray | Fracture, spondylolisthesis, spondylosis (initial screening) |
| MRI spine | Preferred for disc herniation, cord/nerve compression, infection, neoplasm |
| CT | If MRI contraindicated; bony detail |
| CBC, ESR, CRP | Infection, inflammatory arthritis, malignancy |
| HLA-B27 | Suspected spondyloarthritis |
| Bone scan / SPECT | Facet arthropathy, metastases, stress fractures |
| EMG/NCV | Radiculopathy (note: may be negative in acute disc herniation) |
| PSA, SPEP, urine BJP | Prostate ca, myeloma if indicated |
MRI is not routinely needed in acute mechanical LBP without red flags, as most cases resolve within 6 weeks.
Management
Step 1 - Acute Mechanical LBP (< 6 weeks)
Most cases resolve spontaneously. Over-investigation and over-treatment should be avoided.
Non-pharmacological (first-line):
- Reassurance and patient education - avoid bed rest; early return to normal activity within 2 weeks is widely recommended
- Targeted physiotherapy and core-strengthening exercises
- Heat application
- Manual therapy / spinal manipulation (modest benefit; non-inferior to other physical therapies)
- Massage (short-lived benefit for spasmodic/tension-based pain)
Pharmacological:
- NSAIDs - first-line analgesic (e.g., ibuprofen, naproxen, diclofenac); reduce inflammation and pain
- Non-benzodiazepine muscle relaxants (e.g., methocarbamol, cyclobenzaprine) - useful for spasm
- Paracetamol - no longer recommended as first-line; insufficient evidence for back pain specifically
- Opioids - short-term only for debilitating acute pain; lowest effective dose; avoid long-term; never combine with benzodiazepines (risk of respiratory depression)
- Gabapentinoids (gabapentin, pregabalin) - insufficient evidence for either axial or radicular back pain
Step 2 - Specific Cause Management
Disc herniation with radiculopathy:
- NSAIDs + muscle relaxants + physiotherapy as initial treatment
- If not improving: lumbar epidural steroid injection (LESI) for fast relief (if no severe neural compression)
- Surgery (microdiscectomy) for: moderate-severe focal neurological deficit, bowel/bladder dysfunction, or severe pain >3 months not responding to conservative management
Facet joint syndrome:
- NSAIDs first line
- If refractory: diagnostic medial branch block; intra-articular corticosteroid injection; radiofrequency ablation (medial branch neurotomy)
SI joint syndrome:
- NSAIDs first line
- SI joint corticosteroid injection for temporary relief
- Radiofrequency ablation if injections give short-lived benefit
Spinal stenosis:
- Physiotherapy, NSAIDs, analgesics
- Epidural steroid injections
- Surgical decompression (laminectomy) for severe/progressive neurological deficits
Inflammatory spondyloarthritis:
- NSAIDs (high doses); exercise is important
- TNF inhibitors / IL-17 inhibitors for NSAID-refractory disease
Vertebral osteomyelitis:
- IV antibiotics (target organism); surgical drainage if abscess, instability, or neurological compromise
Vertebral compression fracture:
- Analgesia, mobilisation, osteoporosis treatment (bisphosphonates, calcium/vitamin D)
- Kyphoplasty/vertebroplasty in selected cases
Malignancy:
- Radiotherapy, steroids (for cord compression), surgical stabilisation, systemic oncology treatment as appropriate
Step 3 - Chronic LBP (> 3 months)
Multimodal / Interdisciplinary approach:
- Biopsychosocial model - address psychological comorbidities (depression, anxiety, catastrophisation, fear-avoidance)
- Cognitive-behavioural therapy (CBT) - reduces pain intensity; strong evidence
- Mindfulness-based stress reduction (MBSR)
- Yoga, Tai Chi - evidence for benefit
- Acupuncture - modest, short-lived benefit; true acupuncture slightly superior to sham
Pharmacological for chronic LBP:
- Duloxetine (SNRI) - evidence for pain reduction in chronic LBP; also addresses comorbid depression
- Tricyclic antidepressants - analgesic benefit independent of antidepressant effect
- NSAIDs (with gastroprotection)
- Opioids are not recommended for long-term use; no demonstrated long-term benefit for pain or function
Interventional procedures:
- Fluoroscopic epidural steroid injections (for radicular component)
- Facet joint injections / medial branch blocks
- Radiofrequency ablation
- Spinal cord stimulation (for refractory cases)
Surgery (last resort):
- Indicated for progressive neurological deficit, cauda equina syndrome, or failure of ≥3 months of comprehensive conservative treatment with confirmed structural lesion on imaging
MRI Images of Common Structural Causes
Disc herniation with cord compression (cervical, same mechanism applies to lumbar):
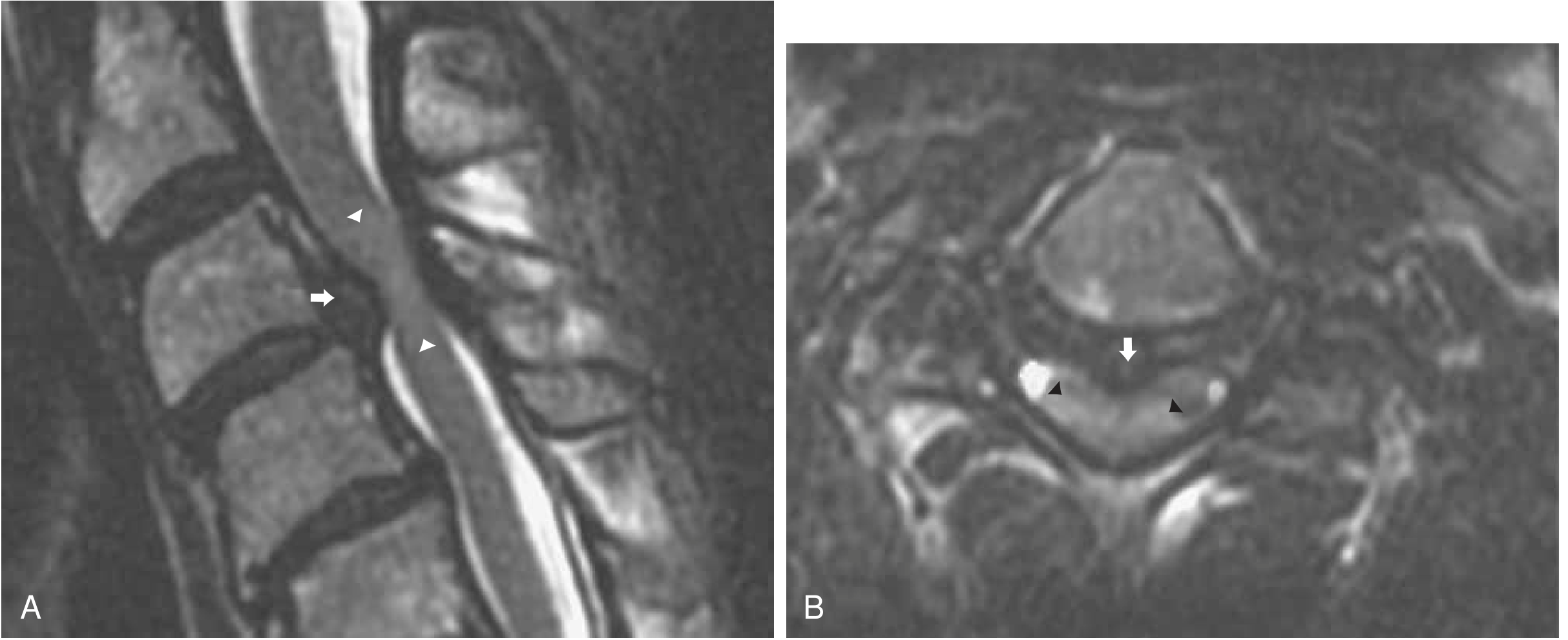
Sagittal T2 MRI (A): disc herniation compressing the cord with hyperintense signal in the cord parenchyma (arrowheads). Axial T2 (B): central disc herniation (arrow) with cord signal change (arrowheads). - Bradley & Daroff's Neurology
Summary Table
| Cause | Key Feature | SLR | Neurology | First-line Rx |
|---|---|---|---|---|
| Muscle strain | Acute injury, spasm | - | Normal | NSAIDs, muscle relaxants, PT |
| Disc herniation (L4/5, L5/S1) | Dermatomal radiation, Valsalva worsens | + | May be abnormal | NSAIDs, PT; LESI if refractory |
| Facet joint syndrome | Extension worsens, no below-knee radiation | - | Normal | NSAIDs; joint injection |
| SI joint syndrome | Buttock/thigh pain, Patrick test + | - | Normal | NSAIDs; SI injection |
| Spinal stenosis | Neurogenic claudication, relieved by flexion | - | Variable | PT; epidural; surgery |
| Spondyloarthritis | <40 yr, morning stiffness, improves with exercise | - | Normal | NSAIDs; TNFi |
| Vertebral osteomyelitis | Fever, night pain, tenderness | - | Variable | IV antibiotics |
| Metastatic disease | Nocturnal pain, weight loss, history of cancer | - | Variable | RT, steroids, surgery |
| Cauda equina syndrome | Bowel/bladder dysfunction, saddle anaesthesia | - | Bilateral | SURGICAL EMERGENCY |
Sources: Harrison's Principles of Internal Medicine 22e (2025) - p.170; Bradley & Daroff's Neurology in Clinical Practice - p.796, 1100; Firestein & Kelley's Textbook of Rheumatology - p.569; KNGF Guideline on LBP Management 2024 (PMID 38407016)
This is a shared conversation. Sign in to Orris to start your own chat.