explain me 10 common heart disease with ECG changes and ecg images of those disease, in simplified manner for neetpg and fmge preparation
ECG changes myocardial infarction STEMI
atrial fibrillation ECG electrocardiogram
complete heart block third degree AV block ECG
Wolff-Parkinson-White WPW syndrome ECG delta wave
left ventricular hypertrophy ECG voltage criteria
pulmonary embolism ECG S1Q3T3 right heart strain
ventricular tachycardia ECG wide complex tachycardia
hyperkalemia ECG peaked T waves sine wave
pericarditis ECG saddle shaped ST elevation diffuse
right bundle branch block RBBB ECG RSR pattern V1
🫀 10 Common Heart Diseases — ECG Changes (NEET PG / FMGE Guide)
1. 🔴 STEMI — ST Elevation Myocardial Infarction
What happens?
Key ECG Changes (in order of evolution):
| Stage | ECG Finding |
|---|---|
| Hyperacute (mins) | Tall, peaked hyperacute T waves |
| Acute (hours) | ST elevation (convex / tombstone) |
| Evolving (hours–days) | Q waves appear + T wave inversion |
| Old MI | Persistent Q waves, T inversion |
Localisation (must know for MCQs):
| Leads with ST elevation | Territory | Artery |
|---|---|---|
| V1–V4 | Anterior | LAD |
| II, III, aVF | Inferior | RCA |
| I, aVL, V5–V6 | Lateral | LCx |
| V1–V2 (posterior: tall R, ST depression) | Posterior | RCA/LCx |
MCQ Tip: Reciprocal ST depression in opposite leads confirms STEMI (e.g., inferior STEMI → ST depression in I, aVL).
ECG — Anterior STEMI (tombstone pattern, V2–V5):
ECG — Inferior STEMI (ST elevation II, III, aVF with reciprocal changes in I, aVL):
2. 💜 Atrial Fibrillation (AF)
What happens?
Key ECG Changes:
- ❌ No P waves (replaced by fine fibrillatory f-waves, best seen in V1)
- ✅ Irregularly irregular R-R intervals
- QRS is narrow (unless aberrant conduction)
- Ventricular rate variable (can be fast, normal, or slow)
MCQ Tip: "Irregularly irregular" = AF. Most common sustained arrhythmia. Causes: valvular disease (especially mitral stenosis), hypertension, thyrotoxicosis, alcohol.
ECG — Atrial Fibrillation:

3. 💙 Complete Heart Block (3rd Degree AV Block)
What happens?
Key ECG Changes:
- P waves present at their own rate (faster, ~60–100/min)
- QRS complexes at escape rate (slower, 20–40/min)
- No relationship between P waves and QRS (AV dissociation)
- QRS wide if ventricular escape, narrow if junctional escape
MCQ Tip: "P waves march through QRS complexes" = 3rd degree block. Requires pacemaker implantation. Commonest cause: ischemic heart disease (inferior MI involving AV node).
ECG — Complete Heart Block:
4. ⚡ Wolff-Parkinson-White (WPW) Syndrome
What happens?
Key ECG Changes (Classic Triad):
- Short PR interval (< 120 ms) — fast conduction via accessory pathway
- Delta wave — slurred upstroke at start of QRS (slow conduction through ventricular muscle)
- Wide QRS (> 120 ms) — due to delta wave
MCQ Tips:
- Type A WPW: Positive delta wave in V1 → left-sided pathway
- Type B WPW: Negative delta wave in V1 → right-sided pathway
- Can cause SVT (AVRT) — most common arrhythmia
- Never give digoxin/verapamil/adenosine in WPW with AF → may accelerate conduction → VF
- Treatment: Radiofrequency ablation
ECG — WPW Syndrome:

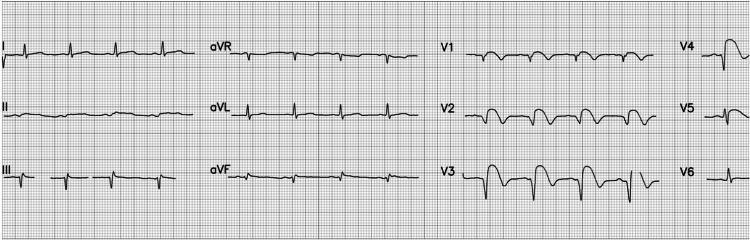
5. 🫁 Pulmonary Embolism (PE)
What happens?
Key ECG Changes:
- S1Q3T3 pattern (most classic MCQ finding):
- S wave in Lead I
- Q wave in Lead III
- T inversion in Lead III
- Sinus tachycardia (most common finding overall)
- Right axis deviation
- RBBB (complete or incomplete)
- T inversion V1–V4 (right ventricular strain)
- P pulmonale (peaked P in II)
MCQ Tip: S1Q3T3 is classic but only present in ~20% of cases. Sinus tachycardia is the most common ECG finding in PE. Must exclude STEMI (PE can mimic inferior MI).
ECG — Pulmonary Embolism (S1Q3T3):

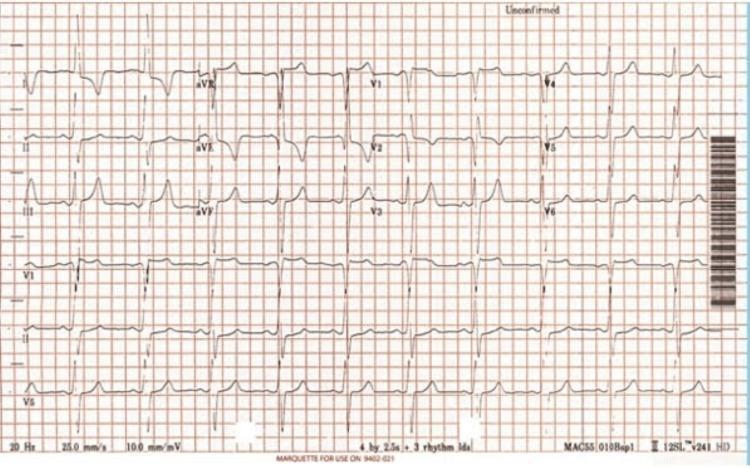
6. 🟣 Left Ventricular Hypertrophy (LVH)
What happens?
Key ECG Changes:
- Voltage criteria:
- Sokolow-Lyon: S in V1 + R in V5/V6 > 35 mm
- Cornell: R in aVL + S in V3 > 28 mm (men) / > 20 mm (women)
- R in aVL > 11 mm alone
- LV strain pattern: ST depression + T inversion in V5, V6, I, aVL (like a "strain" pattern)
- Left axis deviation
- Prolonged QRS
MCQ Tip: Most common cause = systemic hypertension. Sokolow-Lyon criteria most commonly tested. LV strain = asymmetric T inversion in lateral leads.
ECG — LVH with strain pattern:
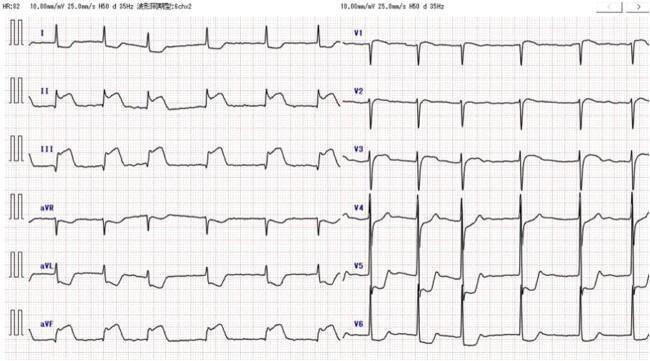
7. 🟠 Acute Pericarditis
What happens?
Key ECG Changes (4 Stages):
| Stage | Finding |
|---|---|
| 1 (early) | Diffuse concave (saddle-shaped) ST elevation (all leads except aVR, V1) + PR depression |
| 2 | ST returns to baseline |
| 3 | T wave inversion (diffuse) |
| 4 | ECG normalizes |
| Feature | Pericarditis | STEMI |
|---|---|---|
| ST shape | Concave (saddle) | Convex (tombstone) |
| Distribution | Diffuse (all leads) | Territorial |
| PR segment | Depressed | Normal |
| Q waves | Absent | Present (evolving) |
| Reciprocal ST depression | Only in aVR/V1 | Yes (opposite leads) |
MCQ Tip: PR depression = pathognomonic of pericarditis. Cause: young adults — viral (Coxsackie B), post-MI (Dressler's syndrome), uraemia, SLE.
ECG — Acute Pericarditis:

8. ⚠️ Ventricular Tachycardia (VT)
What happens?
Key ECG Changes:
- Rate: 100–250/min
- Wide QRS (> 120 ms) — bizarre morphology
- Regular rhythm (monomorphic VT)
- No P waves visible (or AV dissociation)
- Capture beats and fusion beats (pathognomonic of VT)
- Concordance in precordial leads
- No RS complex in any precordial lead
- RS duration > 100 ms
- AV dissociation
- Morphological criteria (notching of downstroke)
MCQ Tips:
- All wide-complex tachycardias = VT until proven otherwise
- Torsades de Pointes = polymorphic VT with twisting QRS around baseline → seen in long QT syndrome
- Treatment: Amiodarone, DC cardioversion if hemodynamically unstable
ECG — Ventricular Tachycardia:

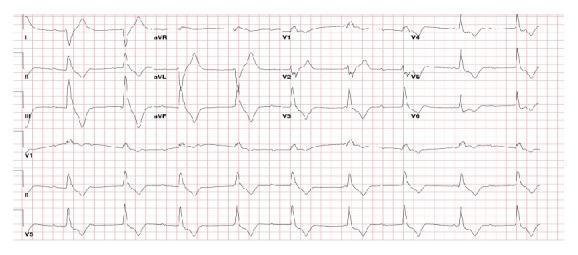
9. 🔵 Hyperkalemia
What happens?
Key ECG Changes (progressive with rising K⁺):
| K⁺ Level | ECG Finding |
|---|---|
| 5.5–6.5 mEq/L | Tall, peaked (tented) T waves — narrow base, symmetric |
| 6.5–7.5 mEq/L | PR prolongation, P wave flattening/disappearance |
| 7.5–8.0 mEq/L | QRS widening (intraventricular conduction delay) |
| > 8.0 mEq/L | Sine wave pattern → VF → cardiac arrest |
MCQ Tips:
- First ECG change = peaked T waves (not tall, but narrow-based and symmetric)
- Cause: CKD/renal failure, Addison's disease, K-sparing diuretics, ACE inhibitors
- Treatment: IV Calcium gluconate (membrane stabiliser, immediate) → Insulin + Dextrose → Sodium bicarbonate → Dialysis
ECG — Hyperkalemia (peaked T waves + QRS widening):
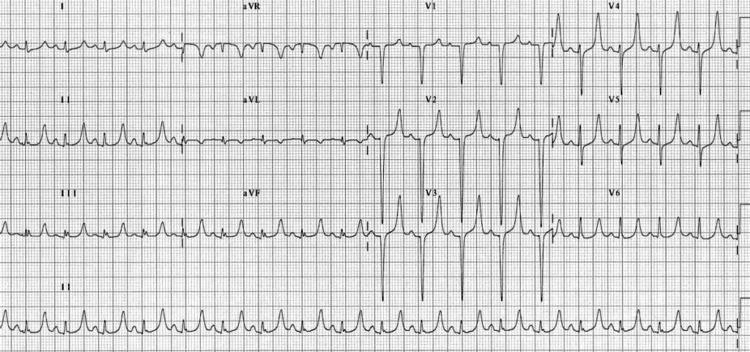
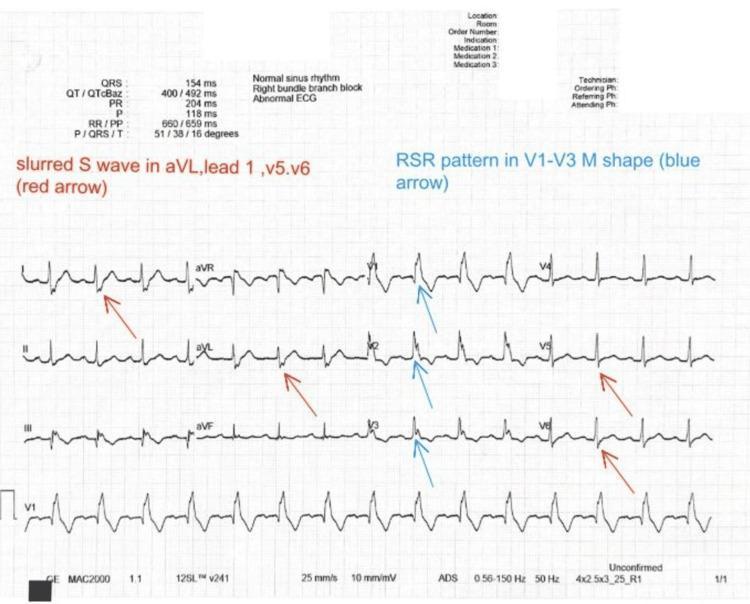
10. 🩵 Right Bundle Branch Block (RBBB)
What happens?
Key ECG Changes:
- Wide QRS > 120 ms (complete RBBB); 100–120 ms = incomplete
- rSR' pattern in V1 ("M-shaped" / "rabbit ears") — signature finding
- Wide, slurred S waves in I, V5, V6 (lateral leads)
- T inversion in V1–V3 (secondary repolarisation change)
MCQ Tips:
- "WiLLiaM MoRRoW" mnemonic: LBBB = W in V1, M in V6 (William); RBBB = M in V1, W in V6 (Morrow)
- New RBBB in chest pain = right heart strain → think PE or RV infarct
- RBBB alone in young = often benign
- Causes: PE, cor pulmonale, ASD, cardiomyopathy, congenital
ECG — Right Bundle Branch Block:
🧠 Quick MCQ Recall Table
| Condition | Key ECG Finding | Top MCQ Buzzword |
|---|---|---|
| STEMI | ST elevation (convex) + Q waves | Tombstone ST, reciprocal changes |
| Atrial Fibrillation | No P waves, irregularly irregular | "Irregularly irregular" |
| Complete Heart Block | P–QRS dissociation | "P waves march through QRS" |
| WPW | Short PR + delta wave + wide QRS | Delta wave, Bundle of Kent |
| Pulmonary Embolism | S1Q3T3, sinus tachycardia | S1Q3T3, right heart strain |
| LVH | Voltage criteria, lateral strain | Sokolow-Lyon >35mm |
| Pericarditis | Diffuse saddle ST + PR depression | PR depression, Dressler's |
| Ventricular Tachycardia | Wide QRS, fast, AV dissociation | Wide complex tachycardia |
| Hyperkalemia | Peaked T waves → sine wave | Peaked T, tent T |
| RBBB | rSR' in V1, slurred S in V6 | Rabbit ears, Morrow pattern |
💡 Study Tips for NEET PG/FMGE:
- Learn lead groupings by territory (inferior = II, III, aVF; anterior = V1–V4; lateral = I, aVL, V5–V6)
- Practice "Which artery is blocked?" questions using lead localisation
- PR depression = pericarditis (almost always comes as a 1-liner MCQ)
- WPW drugs to AVOID: Digoxin, Verapamil, Adenosine (in AF with WPW)
- Complete heart block → Pacemaker; VT → Amiodarone/DC cardioversion
teach me borhavve syndrome for neetpg fmge , simplified with image
Boerhaave syndrome esophageal perforation chest X-ray CT scan
Boerhaave syndrome NEET PG FMGE esophageal perforation key points MCQ
Mackler triad Boerhaave syndrome mediastinitis pneumomediastinum
🫁 Boerhaave Syndrome — Complete NEET PG / FMGE Guide
🔑 What Is It?
Named after Dutch physician Herman Boerhaave who described it in 1724. Historically uniformly fatal until 1947 when the first successful surgical repair was performed. Current mortality: ~20–40% (highest of all GI perforations).
🧠 Pathophysiology — How Does It Happen?
Forceful vomiting / retching
↓
Sudden ↑ intraesophageal pressure
↓
Closed glottis (no pressure escape)
↓
Intrinsic weakness of LEFT POSTERIOR WALL of DISTAL esophagus
↓
FULL THICKNESS TEAR (transmural)
↓
Gastric contents → Mediastinum → Pleura
↓
Chemical Mediastinitis → Sepsis → Death
Why left side? The distal esophagus is anatomically weakest at its left posterolateral wall, just above the gastroesophageal (GE) junction — hence left pleural effusion is more common.
Why no serosa? The esophagus is the only GI organ without a serosal layer, so once the wall ruptures, there is no barrier — contents leak directly into the mediastinum.
📍 Site of Rupture (MCQ Favourite)
| Location | Details |
|---|---|
| Most common site | Left posterolateral wall of distal 1/3 of esophagus (3–5 cm above GE junction) |
| Left chest involvement | Most common side (due to anatomy) |
| Cervical perforation | Rare in Boerhaave; more common in iatrogenic |
⚡ Classic Cause & Triggers
- Weightlifting
- Childbirth / labour straining
- Defecation (Valsalva)
- Seizures
- Coughing / asthma attacks
- Blunt abdominal trauma
🩺 Clinical Features
⭐ Mackler's Triad (Classic MCQ Triad)
"Vomiting → Chest Pain → Subcutaneous Emphysema"
| Feature | Detail |
|---|---|
| 1. Vomiting/Retching | Precedes the pain — the triggering event |
| 2. Severe chest/epigastric pain | Sudden onset, excruciating, pleuritic; radiates to back |
| 3. Subcutaneous emphysema | Air tracked up to neck, palpable "crackling" in neck/chest |
Other Clinical Signs:
- Hamman's sign — Crunching/crackling sound heard on auscultation synchronous with heartbeat (due to pneumomediastinum) — pathognomonic
- Dyspnoea, cyanosis
- Fever, tachycardia (signs of mediastinitis)
- Dysphagia, odynophagia
- Signs of septic shock if delayed
🔴 Boerhaave vs Mallory-Weiss — High-Yield Comparison
| Feature | Boerhaave Syndrome | Mallory-Weiss Syndrome |
|---|---|---|
| Type of tear | Full thickness (transmural) | Partial thickness (mucosal only) |
| Location | Distal esophagus (left posterior) | GE junction / gastric cardia |
| Presentation | Chest pain + subcutaneous emphysema | Haematemesis (painless / minimal pain) |
| Trigger | Forceful vomiting against closed glottis | Retching/vomiting (any) |
| Mortality | HIGH (20–40%) | LOW (heals spontaneously in 90%) |
| Diagnosis | Contrast esophagogram | Endoscopy |
| Treatment | Surgical repair (emergency) | Conservative / endoscopic haemostasis |
MCQ Tip: Mallory-Weiss = blood in vomit. Boerhaave = chest pain + surgical emergency.
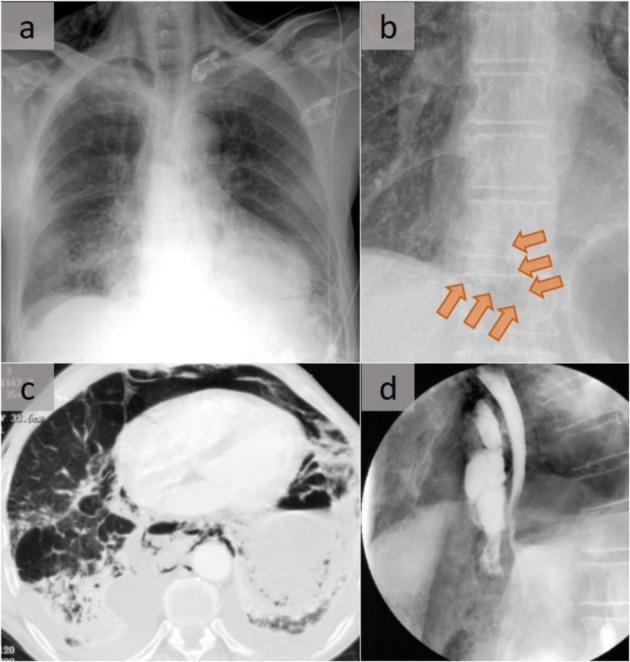
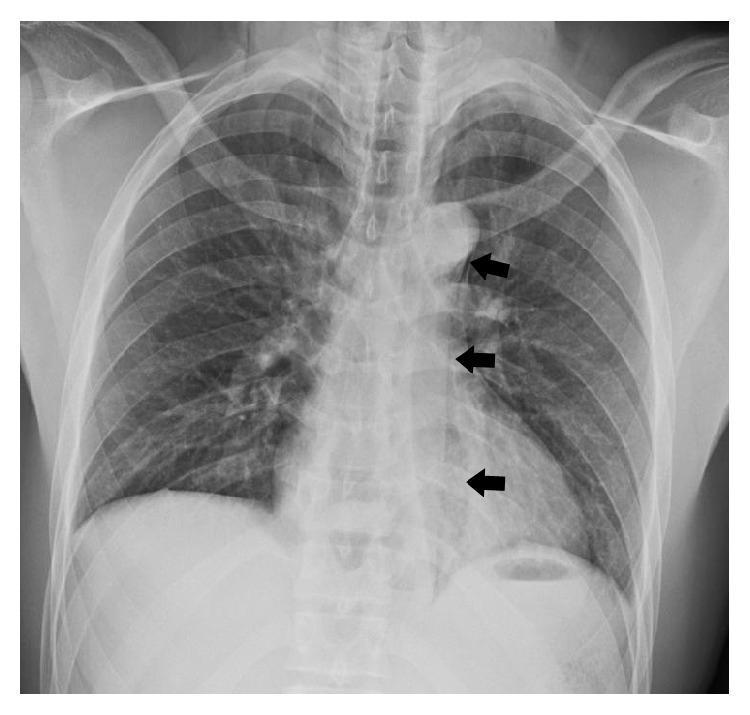
🩻 Investigations
1. Chest X-Ray (First line / screening)
- Pneumomediastinum — air around mediastinal structures (earliest sign)
- Left pleural effusion (or hydropneumothorax)
- Subcutaneous emphysema in neck
- Widened mediastinum
- Naclerio V-sign — V-shaped gas collection at left lower mediastinal border between parietal pleura and diaphragm (pathognomonic on CXR)
2. ⭐ Gold Standard — Contrast Esophagogram (Gastrografin swallow)
- Use water-soluble contrast (Gastrografin) first — shows extravasation of contrast outside esophagus
- If negative but high suspicion → use barium (more sensitive but causes chemical mediastinitis if it leaks)
- Confirms diagnosis + localises the site
3. CT Chest (best for complications)
- Pneumomediastinum
- Pleural effusion / empyema
- Esophageal wall defect + contrast extravasation
- Mediastinitis (fat stranding)
🖼️ Imaging — Boerhaave Syndrome

💉 Treatment
Emergency Surgery (Mainstay — within 24 hours)
| Time from Injury | Treatment |
|---|---|
| < 24 hours (early) | Primary surgical repair (direct suture of tear) + mediastinal drainage |
| > 24 hours (delayed) | Diversion + drainage (T-tube, oesophagectomy if severe) |
Conservative (selected cases only)
- Small, contained perforation with no mediastinitis
- Nothing by mouth (NPO) + IV fluids
- Broad-spectrum antibiotics (cover oral flora — gram positives, anaerobes)
- IV PPI (decreases chemical mediastinitis from acid reflux)
- Close monitoring
Endoscopic Treatment
- Endoscopic stent placement (for contained tears)
- Endoscopic clipping
MCQ Tip: Primary surgical repair within 24 hours = best outcome. After 24 hours, mortality rises dramatically. Always give IV antibiotics + IV PPI as adjuncts.
⚰️ Complications
- Mediastinitis — most dangerous, life-threatening
- Empyema (pus in pleural space)
- Sepsis / Septic shock
- ARDS
- Esophageal fistula
- Tracheo-esophageal fistula
🧠 High-Yield MCQ Summary
| Point | Answer |
|---|---|
| Classic triad | Mackler's triad — Vomiting + Chest pain + Subcutaneous emphysema |
| Pathognomonic sign on CXR | Naclerio V-sign |
| Pathognomonic auscultation sign | Hamman's sign (crunching with heartbeat) |
| Most common site of rupture | Left posterolateral distal esophagus |
| Gold standard investigation | Contrast esophagogram (Gastrografin) |
| Best first-line investigation | Chest X-ray |
| Most sensitive investigation | CT chest |
| Treatment of choice | Primary surgical repair < 24 hours |
| Key difference from Mallory-Weiss | Full thickness vs partial; no haematemesis vs haematemesis |
| Most common cause of esophageal perforation overall | Iatrogenic (endoscopy) — Boerhaave is spontaneous |
| Drug always given | IV Antibiotics + IV PPI |
| Mortality | ~20–40% |
🗂️ One-Liner for Quick Recall
"Middle-aged man, heavy meal + alcohol, forceful vomiting → sudden tearing chest pain radiating to back + neck crepitus → Naclerio V on CXR + Gastrografin leak = Boerhaave → Immediate surgery"