HIV
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Searching PubMed
"HIV" AND "pathogenesis"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a thorough overview. Here is the complete answer.
HIV: Virology, Pathogenesis, and Epidemiology
1. Classification and Discovery
HIV (Human Immunodeficiency Virus) is the causative agent of AIDS (Acquired Immunodeficiency Syndrome). It was first isolated in 1983 from a patient with lymphadenopathy, and by 1984 was definitively linked to AIDS, which had first been recognized in the United States in 1981. HIV belongs to the Lentivirus genus of the family Retroviridae.
Two main types exist:
- HIV-1 - responsible for the global pandemic; more virulent
- HIV-2 - less transmissible; predominantly found in West Africa; progresses more slowly
2. Virology
Structure
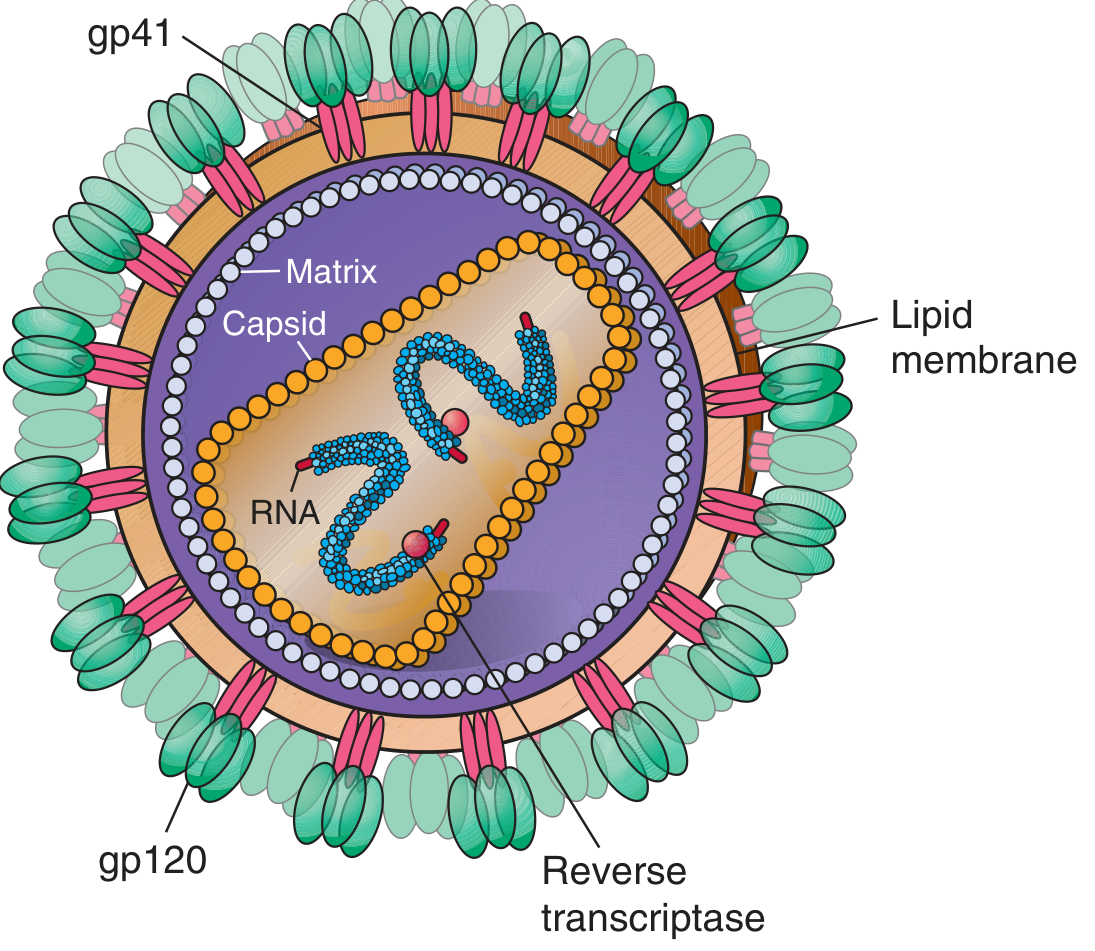
HIV-1 is an enveloped, positive-sense, single-stranded RNA virus with a cone-shaped capsid. Key structural components:
| Component | Protein | Function |
|---|---|---|
| Envelope spike (outer) | gp120 | Binds CD4 receptor on host cells |
| Transmembrane anchor | gp41 | Mediates membrane fusion for cell entry |
| Matrix | p17 | Lines inner lipid membrane |
| Capsid (core) | p24 | Surrounds the RNA genome |
| Enzymes (inside core) | Reverse transcriptase, Integrase, Protease | Replication machinery |
Genome
The HIV genome (~9.8 kb) encodes three major structural genes:
- gag - codes for core proteins (p24, p17)
- pol - codes for enzymes (reverse transcriptase, integrase, protease)
- env - codes for envelope glycoproteins (gp120, gp41)
HIV-1 is more complex than simple retroviruses: it also carries six regulatory genes - tat, rev, nef, vif, vpr, and vpu - which modify the host cell and regulate viral gene expression. HIV-2 lacks vpu but uniquely has vpx. The genome is flanked by long terminal repeats (LTRs) that regulate gene expression. - Harrison's Principles of Internal Medicine, 22E, p. 1601
Replication Cycle
- Attachment: gp120 binds the CD4 receptor on T helper cells, macrophages, and dendritic cells
- Co-receptor binding: gp120 then engages a co-receptor - mainly CCR5 (early infection, macrophage-tropic strains) or CXCR4 (late infection, T-cell tropic strains)
- Fusion: gp41 undergoes conformational change, fusing viral and cell membranes
- Reverse transcription: Viral RNA is converted to double-stranded DNA by reverse transcriptase (an error-prone enzyme with no proofreading - generating enormous viral diversity)
- Integration: Viral DNA is inserted into the host genome by integrase, forming the provirus (may remain latent for years)
- Transcription & Translation: Host RNA polymerase transcribes proviral DNA
- Assembly & Budding: New virions bud from the cell surface; protease cleaves polyproteins to produce mature, infectious particles
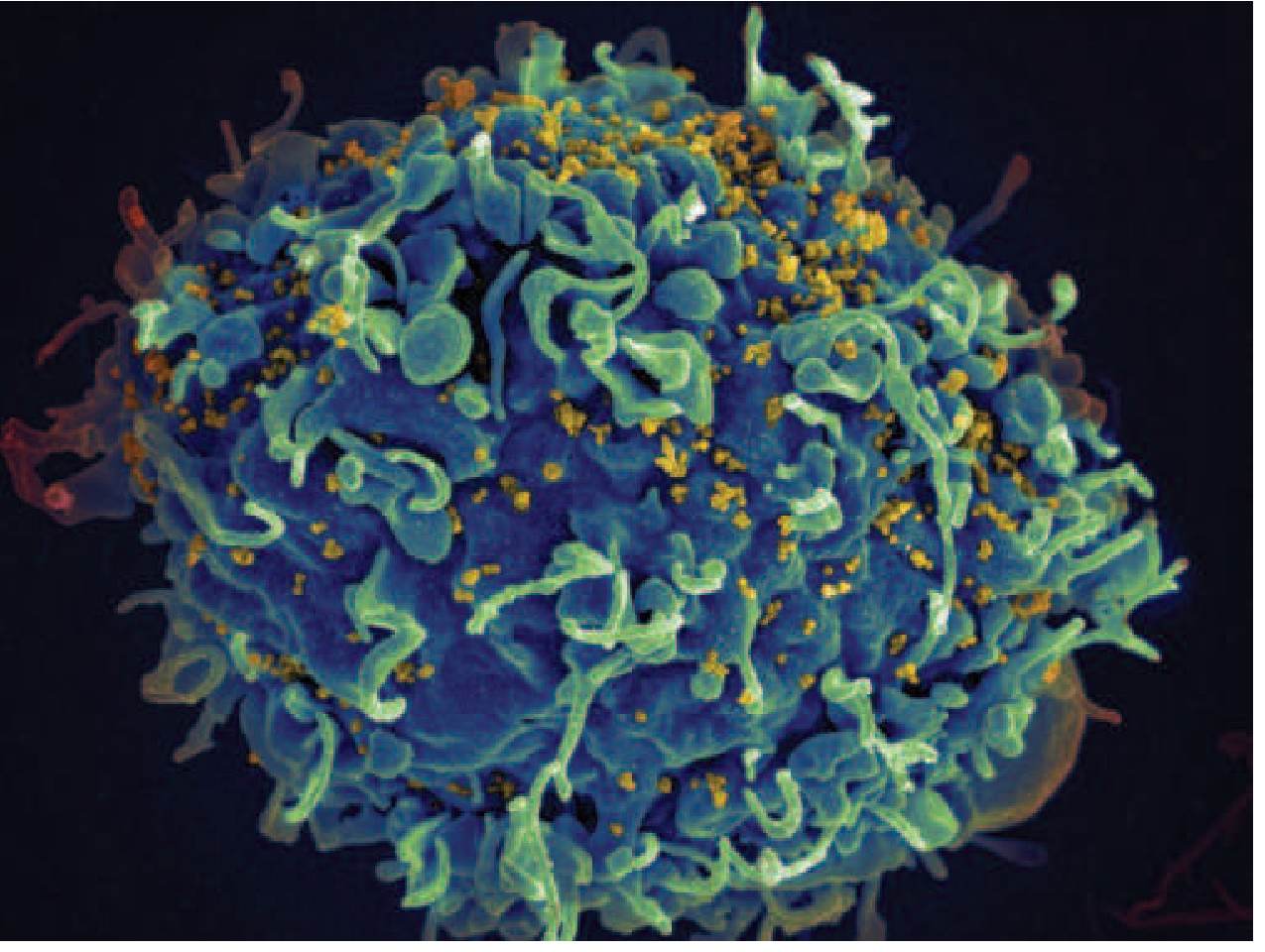
Scanning electron micrograph: HIV-1 (yellow) budding from an infected H9 T cell (blue)
3. Molecular Heterogeneity
HIV-1 is classified into four groups:
- Group M (Major) - responsible for >90% of global infections; further divided into subtypes (clades) A through K
- Group O (Outlier)
- Group N (Non-M/Non-O)
- Group P
The error-prone nature of reverse transcriptase (no proofreading capability) drives continuous mutation, producing quasi-species within a single host and major diversity between geographic regions. This heterogeneity complicates vaccine development and contributes to drug resistance. - Harrison's 22E, p. 1602
4. Pathogenesis
Primary Target: CD4+ T Lymphocytes
HIV's core pathogenic mechanism is the progressive depletion of CD4+ T lymphocytes (helper T cells), which are the orchestrators of both cellular and humoral immunity. Depletion results from:
- Direct cytopathic killing by viral replication
- Immune-mediated destruction of infected cells by CD8+ cytotoxic T lymphocytes
- Bystander cell death (apoptosis of uninfected cells)
- Impaired CD4+ T cell production
Normal CD4+ count: 500-1500 cells/μL. AIDS is defined (for persons >6 years) when CD4+ drops below 200 cells/μL OR when an AIDS-defining opportunistic illness appears.
Disease Progression Stages
| Stage | CD4 Count | Features |
|---|---|---|
| Acute HIV infection | Transiently drops, then partial recovery | Flu-like syndrome (2-4 weeks post-exposure), high viral load, highly infectious |
| Clinical latency | Gradual decline (may span 8-10 years) | Often asymptomatic; virus still replicating |
| AIDS | <200 cells/μL | Opportunistic infections, AIDS-defining malignancies |
Viral Reservoirs and Latency
A key challenge in eradicating HIV is the establishment of latent reservoirs - long-lived memory CD4+ T cells, macrophages, and dendritic cells harboring integrated proviral DNA that is transcriptionally silent and invisible to the immune system. This latent reservoir persists even with fully suppressive antiretroviral therapy (ART).
Immunologic Dysregulation
Beyond CD4+ T cell loss, HIV causes:
- Chronic immune activation - persistent inflammation even in treated patients
- CD8+ T cell exhaustion - loss of functional cytotoxic responses
- B cell dysfunction - hypergammaglobulinemia but impaired specific antibody responses
- NK cell impairment - reduced innate antiviral surveillance
- Monocyte/macrophage infection - reservoir and source of CNS disease (HIV-associated neurocognitive disorders)
Cellular and Molecular Immunology, Chapter 21
5. Transmission
HIV is transmitted through:
| Route | Efficiency | Notes |
|---|---|---|
| Male-to-male sexual contact | High | Accounts for ~68% of new US infections (2022) |
| Heterosexual contact | Moderate | ~23% of new US infections |
| Injection drug use | High (~0.67% per needle sharing) | Sharing needles/syringes |
| Blood transfusion / blood products | Very high (>90%) | Essentially eliminated in developed countries via screening |
| Perinatal (mother-to-child) | 25-40% untreated | Reduced to <2% with ART |
| Occupational (needlestick) | ~0.23% | Post-exposure prophylaxis (PEP) within 24 hours is protective |
| Breast milk | Low-moderate | Risk reduced with maternal ART |
HIV is NOT transmitted by casual contact, saliva, tears, insects, food, or water. Body fluids that can transmit HIV: blood, semen, vaginal secretions, breast milk, rectal fluids. - Harrison's 22E, pp. 1605-1610
6. Epidemiology
Globally (2024 estimates):
- ~39-40 million people living with HIV worldwide
- Sub-Saharan Africa bears the greatest burden (~67% of all infections)
- ~1.3 million new infections per year globally
United States:
- Annual new infections fell from ~130,000/year (peak, late 1980s) to ~31,800 in 2022 (a 12% decline from 2018-2022)
- Racial/ethnic disparities are stark: Black/African Americans (12% of the US population) account for 37% of new infections; Hispanic/Latinos (18% of population) account for 33%
- HIV is concentrated in urban areas, but the US South has higher rural/semi-urban burden
- Perinatal transmission has fallen dramatically: from ~1750 pediatric cases in 1991 to 62 in 2022
- HIV-related deaths in the US: peaked around 1994, fallen to 1.3 deaths/100,000 in 2022
The primary driver of declining mortality is antiretroviral therapy (ART), which can reduce viral load to undetectable levels, preserve immune function, prevent opportunistic infections, and prevent onward transmission ("Undetectable = Untransmittable," or U=U). - Harrison's 22E, pp. 1610-1612
Key Summary
| Feature | Detail |
|---|---|
| Virus type | Lentivirus (Retroviridae), ssRNA, enveloped |
| Primary receptor | CD4 (with CCR5 or CXCR4 co-receptor) |
| Primary target cell | CD4+ T lymphocyte |
| Hallmark of disease | Progressive CD4+ T cell depletion |
| AIDS-defining CD4 threshold | <200 cells/μL |
| Key enzyme for drug targeting | Reverse transcriptase, Integrase, Protease |
| Global burden | ~40 million living with HIV |
| Curative treatment | None currently; ART is suppressive but not curative |
Let me know if you'd like to go deeper into any specific aspect - clinical staging, ART regimens, opportunistic infections, or vaccine development.
This is a shared conversation. Sign in to Orris to start your own chat.