Lesions above decussation of corticospinal tract in medulla producw
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is the complete, textbook-confirmed answer:
Lesions Above the Decussation of the Corticospinal Tract
Produce: Contralateral (opposite-side) weakness/paralysis
The Key Principle
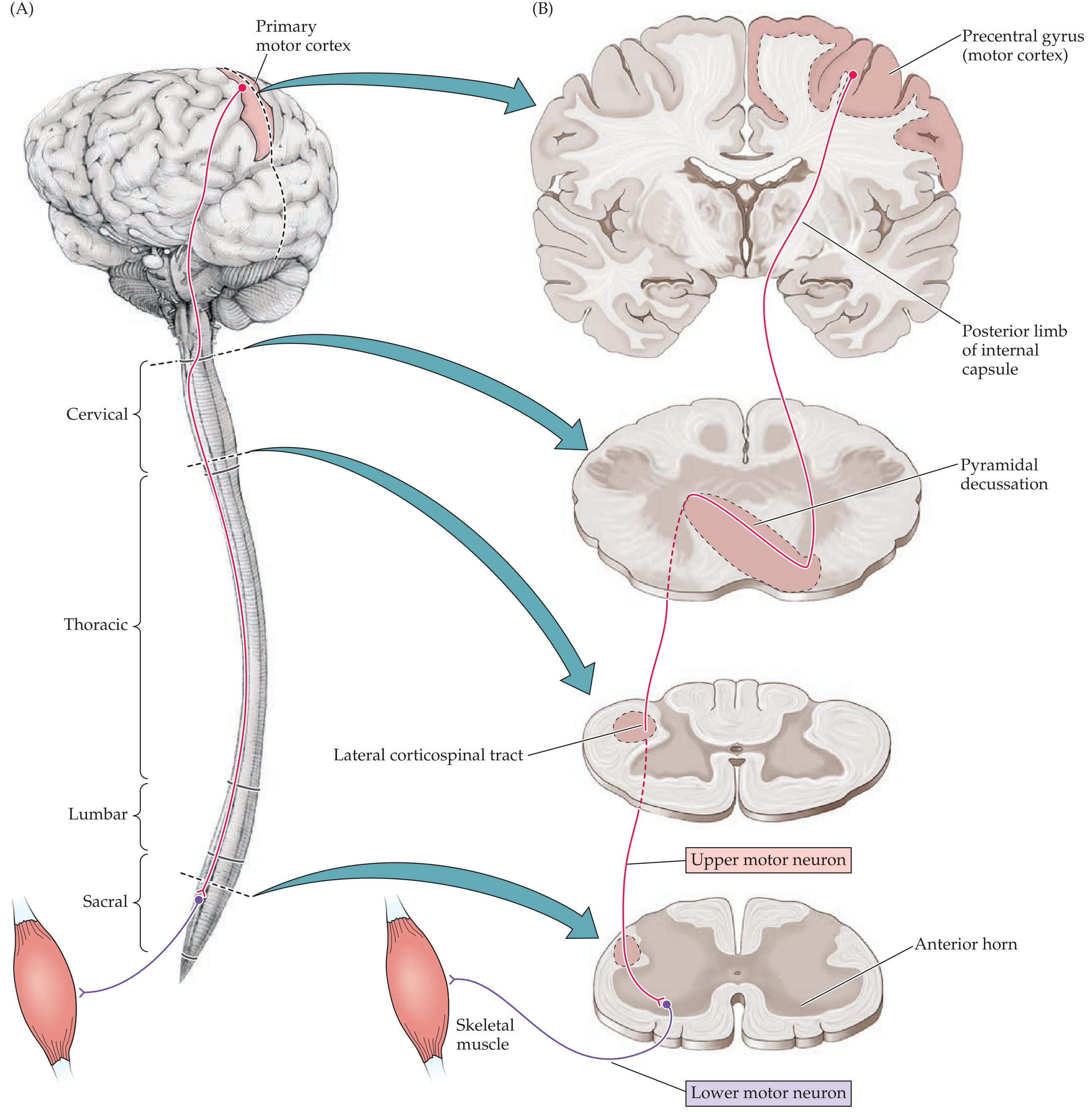
The pyramidal (motor) decussation occurs at the cervicomedullary junction (lower medulla / junction of medulla and spinal cord). About 85-90% of corticospinal fibers cross here to form the lateral corticospinal tract in the contralateral spinal cord.
| Lesion Location | Side of Deficit |
|---|---|
| Above the decussation (cortex, internal capsule, midbrain, pons, upper/mid medulla) | Contralateral (opposite side) weakness |
| Below the decussation (spinal cord - lateral corticospinal tract) | Ipsilateral (same side) weakness |
| At the decussation itself | Can produce complex or bilateral deficits |
Clinical Features of a Lesion Above the Decussation (UMN Syndrome - Contralateral Side)
Because these are upper motor neuron (UMN) lesions, the deficit on the contralateral side includes:
- Contralateral hemiplegia or hemiparesis - weakness of the face, arm, and leg on the opposite side
- Spasticity - increased muscle tone (clasp-knife)
- Hyperreflexia - exaggerated deep tendon reflexes
- Positive Babinski sign (extensor plantar response)
- No significant muscle wasting (wasting occurs only with LMN lesions)
- Clonus may be present
Why Contralateral?
The motor cortex in the left hemisphere controls movement of the right side of the body and vice versa. Its fibers travel uncrossed all the way down through the internal capsule, cerebral peduncle, pons, and medullary pyramids - only crossing at the pyramidal decussation in the lower medulla. So a lesion anywhere rostral to (above) this crossing point will damage fibers that were destined to cross - their effects are felt on the opposite side.
"Lesions of the corticospinal tract occurring above the pyramidal decussation produce contralateral weakness, whereas lesions below the pyramidal decussation produce ipsilateral weakness."
- Neuroanatomy through Clinical Cases, 3rd Edition
Common Clinical Examples of "Above-Decussation" Lesions
| Location | Example Condition | Result |
|---|---|---|
| Cerebral cortex | Middle cerebral artery stroke | Contralateral face + arm weakness |
| Internal capsule | Lacunar infarct | Contralateral pure motor hemiparesis |
| Midbrain (cerebral peduncle) | Weber's syndrome | Contralateral hemiplegia + ipsilateral CN III palsy |
| Pons | Millard-Gubler syndrome | Contralateral hemiplegia + ipsilateral CN VI/VII palsy |
| Upper/rostral medulla | Medial medullary syndrome (rostral to decussation) | Contralateral hemiplegia |
Special Note: At the Decussation Level
Lesions at the pyramidal decussation itself (e.g., "cruciate paralysis") can produce the unusual pattern of ipsilateral arm weakness and contralateral leg weakness, because arm fibers cross more rostrally and leg fibers cross more caudally within the decussation zone.
- Neuroanatomy through Clinical Cases, 3rd Ed. (Blumenfeld)
- Gray's Anatomy for Students
- Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.