Can you explain to me? How in the setting of, uh, diabetic ketoacidosis, we do the step-by-step management? Can you tell me the exact dosages and how they are administered?
"diabetic ketoacidosis" AND management
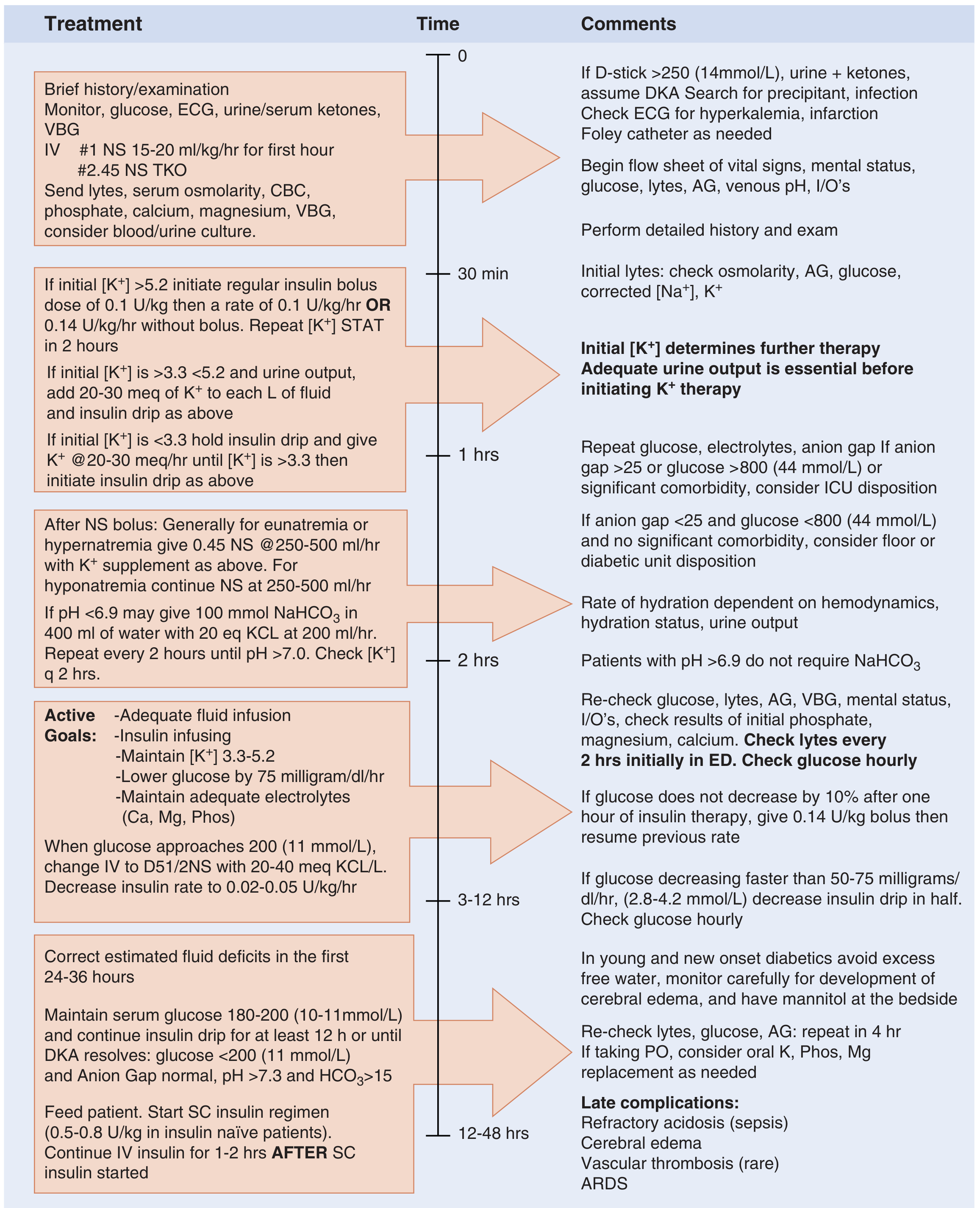
Diabetic Ketoacidosis (DKA): Step-by-Step Management
Diagnostic Criteria (before starting treatment)
- Blood glucose >250 mg/dL (or known diabetes)
- Ketonemia (β-hydroxybutyrate ≥3 mmol/L) or ketonuria (2+ or more)
- Anion-gap metabolic acidosis: arterial/venous pH <7.3 and/or serum bicarbonate <18 mEq/L
Immediate Steps (Time 0 - First 30 Minutes)
- Place at least one large-bore IV (16-18 gauge); consider a second line
- Cardiac monitor (ECG to detect hyper/hypokalemia and ischemia)
- Foley catheter for strict urine output monitoring
- Vital signs, mental status, glucose every hour; electrolytes every 2-4 hours
- Serum glucose, BMP (electrolytes, BUN, creatinine), venous blood gas (VBG)
- Serum β-hydroxybutyrate (preferred over urine dipstick for ketones)
- CBC, phosphate, magnesium, calcium, serum osmolality
- Blood/urine cultures if infection suspected
- ECG (for hyperkalemia signs: peaked T waves)
- Search for the precipitant (infection, ACS, missed insulin, etc.)
Step 1: Fluids (The #1 Priority - Start BEFORE insulin or lab results)
| Time | Fluid | Rate |
|---|---|---|
| Hour 0-1 | 0.9% Normal Saline (isotonic crystalloid) | 15-20 mL/kg/h (approximately 1-1.5 L in first hour) |
| Hours 1-2 | Continue 0.9% NS or switch to 0.45% NS | 500-1000 mL/h (if hemodynamically stable) |
| Hours 2-6 | Adjust based on sodium status: 0.45% NS for eunatremic/hypernatremic; continue 0.9% NS if hyponatremic | 250-500 mL/h |
| Hours 6-12 | Continue replacing deficit | 250-500 mL/h |
Note: Lactated Ringer's or balanced crystalloids are acceptable alternatives to normal saline. Large volumes of normal saline risk hyperchloremic metabolic acidosis, which can prolong the anion gap closure.
- Tintinalli's Emergency Medicine, p. 1479
- Washington Manual of Medical Therapeutics, p. 890
Step 2: Potassium Replacement (MUST Check Before Starting Insulin)
| Initial Serum K+ | Action |
|---|---|
| >5.2 mEq/L | Hold potassium replacement; start insulin; recheck K+ every 2 hours |
| 3.3-5.2 mEq/L | Add 20-40 mEq KCl to each liter of IV fluid; start insulin |
| <3.3 mEq/L | HOLD INSULIN - replace K+ at 20-40 mEq/h IV until K+ >3.3; then start insulin |
-
Once urine output is confirmed (>0.5 mL/kg/h), add 10-40 mEq KCl/h to IV fluids (use continuous cardiac monitoring when rate >10 mEq/h)
-
Target serum K+ of 3.5-5.2 mEq/L throughout treatment
-
Tintinalli's Emergency Medicine, p. 1479; Barash's Clinical Anesthesia, p. 4059
Step 3: Insulin Therapy
For Severe DKA (requires IV insulin):
- IV bolus: 0.1 units/kg regular insulin
- Followed immediately by continuous infusion: 0.1 units/kg/h
- Continuous infusion at 0.14 units/kg/h without bolus
- Glucose should fall by 50-75 mg/dL/h
- If glucose does NOT fall by ≥10% in the first hour → give a rescue bolus of 0.14 units/kg IV, then resume at the same rate
- Add dextrose (D5W) at 100 mL/h OR switch to D5/0.45% NS
- Reduce insulin infusion to 0.02-0.05 units/kg/h to maintain glucose at 150-200 mg/dL
- Do NOT stop insulin - continue until DKA resolves (this is the common mistake)
- Subcutaneous rapid-acting insulin analogs can be used in non-ICU settings
- New evidence (PMID: 39090718, 2024 meta-analysis) confirms comparable outcomes between subcutaneous insulin and IV continuous infusion for adult DKA management
DKA Resolution Criteria:
- Blood glucose <200 mg/dL, AND
- Serum bicarbonate ≥15-18 mEq/L, AND
- Venous pH >7.3, AND
- Anion gap closed (note: bicarbonate normalization is a more reliable endpoint than anion gap closure alone - hyperchloremia can close the gap before full recovery)
Transitioning to Subcutaneous Insulin:
-
Patient must be eating/drinking
-
Administer SC basal insulin 2 hours BEFORE stopping the IV insulin infusion (overlap is mandatory to prevent rebound ketosis)
-
Insulin-naive patients: start at 0.5-0.8 units/kg/day in divided doses
-
Washington Manual, p. 891; Tintinalli's, p. 1479; Barash's Clinical Anesthesia, p. 4059
Step 4: Bicarbonate (NOT Routine)
- pH <6.9 (with or without hemodynamic instability), OR
- Hemodynamic instability with pH <7.1, OR
- Severe hyperkalemia with cardiac/respiratory dysfunction
-
100 mmol (100 mEq) NaHCO₃ in 400 mL of water (or 50-100 mEq in 1 L of 0.45% NS)
-
Infuse over 30-60 minutes at 200 mL/h
-
Add 20 mEq KCl to the bicarbonate infusion to prevent hypokalemia
-
Repeat every 2 hours until pH >7.0
-
Barash's Clinical Anesthesia, p. 4060; Washington Manual, p. 891
Step 5: Phosphate, Magnesium (Not Routine)
- Routine supplementation is not recommended (no proven benefit)
- May consider IV potassium phosphate if patient cannot eat and phosphate is severely low (risk: respiratory muscle weakness, hemolytic anemia)
-
May give 10-20 mEq magnesium sulfate IV if ventricular arrhythmias are present
-
Washington Manual, p. 891
Ongoing Monitoring
| Parameter | Frequency |
|---|---|
| Blood glucose | Every hour |
| Serum electrolytes + anion gap | Every 2-4 hours |
| Venous pH / blood gas | As needed (especially in severe acidosis) |
| β-hydroxybutyrate | Trending down is a reliable marker of recovery |
| Urine output | Continuously via Foley |
| ECG / telemetry | Continuously |
DKA Treatment Timeline (Tintinalli's Emergency Medicine)
Common Pitfalls to Avoid
- Stopping insulin too early - insulin must continue until anion gap closes and pH normalizes, even if glucose is near normal (add dextrose to allow this)
- Not overlapping SC basal insulin - if IV insulin is stopped without starting SC basal 2 hours before, rebound ketoacidosis can occur (especially in SGLT2-inhibitor-associated euglycemic DKA, where the drug effect can persist 10-14 days)
- Starting insulin before correcting K+ - if K+ <3.3, insulin will drive potassium so low it causes fatal arrhythmias
- Using anion gap closure alone as endpoint - hyperchloremia from NS resuscitation can close the gap before full metabolic recovery; track bicarbonate and β-hydroxybutyrate
- Stopping fluids too early - the fluid deficit is massive (5-10 L); replace it over 24-36 hours
Recent Evidence Update
Okay, so I have a few questions. Number one, is there any role for calcium gluconate? Number two... Isn't the insulin drip rate too slow? Like, suppose you are using a micro-drip set. 10 units per hour, doesn't that equate to about six drops per minute? Plus, if the infusion rate is supposed to be 0.1 unit per kg per hour... Will we still use the same formulation for administration if the patient is about... 50 kg. In weight.
Question 1: Is There a Role for Calcium Gluconate in DKA?
- Initial K+ is severely elevated (generally >6.5 mEq/L) AND
- There are active ECG changes of hyperkalemia (peaked T waves, widened QRS, sine wave pattern)
- Swanson's Family Medicine Review, p. 803
- Fischer's Mastery of Surgery; Schwartz's Principles of Surgery, p. 265
Question 2 & 3: The Insulin Drip Rate, Microdrip Math, and the 50 kg Patient
The Standard Formulation (from the textbooks):
Regular insulin 100 units in 100 mL of 0.9% NS = 1 unit/mL Run at 10 mL/h = 10 units/h
Your Microdrip Calculation - Is It Right?
| Step | Calculation |
|---|---|
| Rate needed | 10 mL/h |
| Convert to mL/min | 10 ÷ 60 = 0.167 mL/min |
| Drops/min (microdrip at 60 gtt/mL) | 0.167 × 60 = ~10 drops/min |
| Drip set | gtt/mL | gtt/min for 10 mL/h |
|---|---|---|
| Macrodrip (standard) | 20 gtt/mL | 10 ÷ 60 × 20 = ~3.3 gtt/min |
| Microdrip (pediatric) | 60 gtt/mL | 10 ÷ 60 × 60 = 10 gtt/min |
Now, for your 50 kg Patient:
- 0.1 units/kg/h × 50 kg = 5 units/h
Run at 5 mL/h on your infusion pump
- 0.1 units/kg × 50 kg = 5 units IV push (draw up 5 mL of the 1 unit/mL solution)
- Give rescue bolus: 0.14 units/kg × 50 kg = 7 units IV push, then resume at 5 mL/h
Summary Table for a 50 kg Patient
| Action | Calculation | Dose / Rate |
|---|---|---|
| IV bolus (optional) | 0.1 units/kg × 50 kg | 5 units IV |
| Infusion rate | 0.1 units/kg/h × 50 kg | 5 units/h = 5 mL/h (using 1 unit/mL formulation) |
| Rescue bolus if no response at 1 hr | 0.14 units/kg × 50 kg | 7 units IV |
| When glucose <250 mg/dL | Reduce infusion | 0.02-0.05 units/kg/h = 1-2.5 mL/h, add dextrose |
| Transition basal insulin | 0.5-0.8 units/kg/day SC | 25-40 units/day divided |
Can you tell me the exact... Indications for the use of, uh, IV pump and syringe pump. And, uh... Where the micro and macro drip sets are used.
IV infusion pump vs syringe pump indications clinical use microdrip macrodrip sets
IV Infusion Pumps, Syringe Pumps, and Drip Sets: Indications and Uses
Part 1: Gravity Drip Sets (No Pump)
Macrodrip Set
- Drop factor: 10, 15, or 20 drops per mL (varies by manufacturer; always check the packaging)
- Designed to deliver large volumes quickly
- Used for:
- Routine adult IV fluid replacement (NS, RL, D5W)
- Rapid volume resuscitation (trauma, hypovolemic shock, burns)
- Blood and blood product transfusions (usually 10-15 gtt/mL sets)
- Any situation where the required rate is >60 mL/h and precision is not critical
- Preoperative and postoperative fluid maintenance in adults
Microdrip Set (Mini-drip / Pediatric Set)
- Drop factor: uniformly 60 drops per mL (this is standardized - always 60)
- Produces very small, finely controlled drops
- Used for:
- All pediatric and neonatal patients - to prevent accidental fluid overload (even a few extra drops per minute can overload an infant)
- Adults receiving very low flow rates (where a macrodrip would deliver drops too slowly to count accurately - e.g., 1 drop every 20 seconds becomes error-prone)
- Situations where an IV pump is unavailable (resource-limited settings)
- Drug infusions where some control is needed but pump unavailable
The key rule: microdrip is used when the rate is low AND precision matters (especially in pediatrics). The practical advantage of a microdrip at low rates is that it gives you more drops per minute to count, making gravity titration less error-prone. For example, at 30 mL/h: a macrodrip (20 gtt/mL) gives 10 drops/min (one every 6 seconds - hard to count consistently); a microdrip gives 30 drops/min (one every 2 seconds - much easier).
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 441
- NCBI Nursing Skills, Chapter 23
Part 2: Electronic Infusion Pump (Volumetric IV Pump)
Characteristics
- Volume capacity: typically up to several liters (runs from a bag/bottle)
- Rate range: usually 1 mL/h up to 999 mL/h or more
- Programs in mL/h
- Alarms for occlusion, air-in-line, completion, dose-limit breaches
Indications (an IV pump MUST be used for):
| Indication | Reason |
|---|---|
| All central venous catheter (CVC/PICC/CVP) infusions | Gravity flow through central lines is unreliable and dangerous |
| All pediatric patients | Risk of accidental overhydration with gravity sets; pump enforces exact volume limits |
| Any infusion rate below 60 mL/h | Gravity counting at low rates is too imprecise; a macrodrip at 20 mL/h gives only ~7 drops/min |
| All opioid infusions | High-alert medication; dose errors are life-threatening |
| Total parenteral nutrition (TPN) | Must be precise; infused via volumetric pump with inline filter |
| Chemotherapy | Dose accuracy and infusion time are protocol-mandated |
| Hypertonic solutions (e.g., 3% NaCl) | Rate of osmolality correction must be strictly controlled |
| Oxytocin infusions | Titrated dosing; accidental bolus causes uterine hyperstimulation |
| Any medication with a narrow therapeutic index | Prevents inadvertent under- or over-infusion |
| When the patient is fluid-restricted | Pump enforces total volume delivered |
- Clinical Procedures for Safer Patient Care (BC Open Textbook)
- Washington Manual of Medical Therapeutics, p. 891; Morgan & Mikhail's Clinical Anesthesiology
Part 3: Syringe Pump (Syringe Driver)
Characteristics
- Volume capacity: limited to the syringe size - 10 to 60 mL typically
- Rate range: 0.1 mL/h to ~100 mL/h - but its real advantage is at the low end (0.1 to 10 mL/h), which is called microinfusion
- Extremely precise at low flow rates
- Compact - portable, can attach to IV pole or patient transport equipment
Indications (where syringe pumps excel):
| Indication | Why a Syringe Pump? |
|---|---|
| Vasoactive drugs in ICU (dopamine, norepinephrine, vasopressin, epinephrine) | Must be concentrated and given at very low rates (e.g., 0.1-5 mL/h); rate changes produce near-immediate hemodynamic response - requires precision titration |
| Insulin infusion (like in DKA) | Low rate (e.g., 5 mL/h for a 50 kg patient), concentrated solution (1 unit/mL), narrow therapeutic margin - any inaccuracy causes hypo- or hyperglycemia |
| Sedation and analgesia in ICU (propofol, midazolam, morphine, fentanyl, dexmedetomidine) | Continuous slow infusion, highly potent drugs needing moment-to-moment titration |
| Epidural and intrathecal infusions | Very small volumes into a confined space; no margin for error |
| Neonatal and pediatric ICU drug infusions | Fluid-restricted patients; concentrated drugs at flows as low as 0.1-1 mL/h |
| Chemotherapy (some agents) | Where very small precise volumes must be delivered over hours |
| TPN micronutrient infusions | Concentrated supplements added to TPN at low rates |
| Palliative care / subcutaneous infusions | Syringe drivers administer continuous SC opioids/antiemetics over 24 hours |
| Oxytocin, prostaglandins | Titrated dose in obstetrics where bolus delivery would be dangerous |
| GnRH pulsatile delivery | Timed 2-hourly subcutaneous boluses via miniature syringe pump |
- PMC10155690 - 10 clinical tips for syringe pump microinfusion
- Miller's Anesthesia (10e); Tintinalli's Emergency Medicine
Summary: Quick Reference Table
| Device | Drop factor / Volume | Flow range | Primary use |
|---|---|---|---|
| Macrodrip set (gravity) | 10, 15, or 20 gtt/mL | >60 mL/h | Adult fluid replacement, blood, rapid bolus |
| Microdrip set (gravity) | 60 gtt/mL (always) | <60 mL/h (where some precision needed without pump) | Pediatrics, low-rate adult infusions, resource-limited settings |
| Volumetric IV pump | Bag (up to several litres) | 1-999 mL/h | CVC infusions, all pediatric patients, opioids, TPN, hypertonic fluids, any rate <60 mL/h |
| Syringe pump | Syringe (10-60 mL) | 0.1-100 mL/h (best at 0.1-10 mL/h) | ICU vasoactives, insulin drips, sedation/analgesia, epidurals, neonates, palliative SC infusions |
Directly Applied to the DKA Insulin Infusion
- This is a microinfusion rate (low volume, concentrated drug, narrow therapeutic index)
- A syringe pump is the ideal device: load 50 mL syringe with 50 units regular insulin in 50 mL NS (1 unit/mL), set at 5 mL/h
- A volumetric IV pump can also work if the pump supports low-rate accuracy at 5 mL/h
- A gravity microdrip at 5 mL/h = 5 drops/min - this is too slow and too imprecise for safe insulin delivery; gravity should not be used for insulin infusions
In the emergency setting How do we differentiate between HHS and DKA? What is the step-by-step management for HHS?
HHS vs DKA: Differentiation and Management
Part 1: How to Differentiate HHS from DKA at the Bedside
Clinical Clues at Triage
| Feature | DKA | HHS |
|---|---|---|
| Typical patient | Type 1 DM, any age (toddler to adult) | Type 2 DM, typically elderly |
| Onset | Hours to 1-2 days (rapid) | Days to weeks (insidious) |
| Abdominal pain | Common (can mimic acute abdomen) | Rare |
| Nausea / vomiting | Common | Less frequent |
| Kussmaul breathing (deep, rapid) | Present - driven by metabolic acidosis | Absent |
| Fruity/acetone breath | Present | Absent |
| Altered mental status | Mild to moderate (correlates with osmolality) | Prominent - up to 10% in frank coma; correlates directly with degree and rate of hyperosmolarity |
| Focal neurologic signs | Uncommon | Common - hemiplegia, aphasia, focal deficits, seizures (phenytoin contraindicated here) |
| Degree of dehydration | Significant (5-10 L deficit) | More profound (9-12 L deficit; longer duration of illness) |
| Precipitant | Missed insulin, infection, ACS, new T1DM | Infection most common; stroke, dehydration, medications, inability to access water |
Biochemical Differentiation (the definitive step)
| Lab Value | DKA | HHS |
|---|---|---|
| Blood glucose | >250 mg/dL (but can be lower in euglycemic DKA) | >600 mg/dL (often 800-1000+ mg/dL) |
| Serum ketones / β-hydroxybutyrate | Elevated (≥3 mmol/L) | Absent or trace (starvation ketones only) |
| Arterial/venous pH | <7.3 | >7.3 (rarely drops below 7.30) |
| Serum bicarbonate | <18 mEq/L (often <10 in severe DKA) | >18-20 mEq/L |
| Anion gap | Elevated (wide gap metabolic acidosis) | Normal or mildly elevated (from lactic acidosis/starvation ketones, NOT from diabetes itself) |
| Serum osmolality | Mildly elevated (~300-320 mOsm/L) | Markedly elevated (>320 mOsm/L; often >350) |
| BUN / Creatinine | Elevated (prerenal) | More markedly elevated |
| Sodium | Low-normal (pseudohyponatremia from hyperglycemia) | Normal or elevated; correct for glucose |
The Osmolality Calculation (do this on every hyperglycemic patient)
- Normal: ~285-295 mOsm/L
- DKA: typically 300-320 mOsm/L
- HHS: >320 mOsm/L (diagnostic threshold); severe cases often 350-380+
- Add 1.6 mEq/L to reported Na⁺ for every 100 mg/dL of glucose above 100 mg/dL
- (Some sources use 2.4 for glucose >400 mg/dL)
Quick Summary: The Diagnostic "Shortcut"
DKA = Acidosis + Ketosis + Moderate hyperglycemia HHS = No acidosis + No ketosis + Marked hyperglycemia + Marked hyperosmolality + Altered mental status
- Rosen's Emergency Medicine, Table 115.6, p. 2547
- Goldman-Cecil Medicine, p. 1302
- Harrison's Principles of Internal Medicine (22e), p. 3262
Part 2: Step-by-Step Management of HHS
Step 0: Immediate Setup
- Large-bore IV access (at least one, preferably two lines)
- Cardiac monitor + ECG (check for hyperkalemia, precipitating MI)
- Foley catheter for strict urine output monitoring
- Neurologic assessment (GCS) - repeat frequently throughout treatment
- Supplemental O₂ if needed
Step 1: Fluids (The Central Pillar of HHS Treatment)
- 0.9% Normal Saline: 1-1.5 L over the first 1-2 hours (some sources say 1-3 L over 2-3 hours)
- Goal: restore blood pressure, perfuse kidneys, establish urine output
- Use isotonic saline even though the patient is hyperosmolar - you need to restore intravascular volume first
| Corrected Sodium | Fluid Choice |
|---|---|
| Normal (<145 mEq/L) | 0.45% NS at 200-500 mL/h |
| Elevated (>150 mEq/L) | 0.45% NS (hypotonic) |
| Low (<135 mEq/L) | Continue 0.9% NS |
- Replace the remaining free water deficit gradually over 24-72 hours
- Typical infusion rates: 200-300 mL/h of hypotonic solution after stabilization
- Target: positive fluid balance over 24-72 hours (may require 10-12 L total)
- Monitor for fluid overload closely in elderly patients with heart failure or renal disease - consider invasive hemodynamic monitoring (CVP, arterial line) if at risk for pulmonary edema
- Add D5W or D5/0.45% NS to prevent hypoglycemia while continuing osmolality correction
Step 2: Potassium Replacement
- Total body potassium is still depleted (from prolonged osmotic diuresis)
- Patients on diuretics may have especially large K⁺ deficits, often with accompanying magnesium deficiency
- Add KCl 10-20 mEq/h to IV fluids once urine output is confirmed
- Do not start insulin until K⁺ >3.5 mEq/L
- Target K⁺: 3.5-5.0 mEq/L throughout treatment
Step 3: Insulin (Secondary Role in HHS)
- Fluid resuscitation is underway (at least 1-2 L infused)
- K⁺ is >3.5 mEq/L
- Hemodynamic stability achieved
| Parameter | Dose |
|---|---|
| IV Bolus (if glucose >600 mg/dL) | 5-10 units regular insulin IV |
| Infusion rate | 0.10-0.15 units/kg/h |
| If glucose does not fall | Double the infusion rate |
| When glucose reaches 250-300 mg/dL | Add dextrose to fluids; reduce infusion to 1-2 units/h to maintain glucose 200-300 mg/dL until osmolality normalizes |
- Begin SC basal insulin 2 hours before stopping the infusion
- Once eating and drinking, switch to SC regimen
- Many HHS patients can eventually be managed with oral agents; some may not need insulin long-term
Step 4: Bicarbonate
Step 5: Find and Treat the Precipitant
- Infection - most common: pneumonia, UTI, sepsis (start broad-spectrum antibiotics early after cultures)
- Acute MI (get ECG and troponins)
- Stroke
- GI bleeding
- Pancreatitis
- Thromboembolic events
- Medications: steroids, thiazide diuretics, atypical antipsychotics, SGLT2 inhibitors
Step 6: Anticoagulation (HHS-Specific, Not Routine in DKA)
- Volume depletion and hemoconcentration
- Hyperviscosity
- Hypotension
- Immobility
- Hypercoagulable state
Step 7: Monitoring
| Parameter | Frequency |
|---|---|
| Blood glucose | Every hour |
| Serum electrolytes, BUN, osmolality | Every 2-4 hours |
| Neurological status (GCS) | Every hour - worsening may indicate cerebral edema |
| Urine output | Continuously via Foley |
| Cardiac monitor | Continuously |
- Serum osmolality <310-315 mOsm/L
- Patient alert and oriented
- Blood glucose <300 mg/dL (some use <250)
- Patient able to eat and drink
Summary Comparison Table
| DKA | HHS | |
|---|---|---|
| Primary problem | Ketoacidosis | Hyperosmolality |
| Primary treatment | Insulin + fluids equally | Fluids first, insulin secondary |
| Fluid deficit | 5-10 L | 9-12 L |
| Fluid type | 0.9% NS → 0.45% NS → D5/0.45% NS | 0.9% NS → 0.45% NS → D5W |
| Fluid replacement timeline | 24-36 hours | 24-72 hours (slower correction) |
| Insulin bolus | 0.1 units/kg | 5-10 units (smaller, or none initially) |
| Insulin infusion | 0.1 units/kg/h | 0.05-0.1 units/kg/h |
| Add dextrose when glucose reaches | ~250 mg/dL | ~250-300 mg/dL |
| Bicarb | Only if pH <6.9 | Not indicated |
| Resolution endpoint | pH >7.3, HCO₃ >15, AG closed | Osmolality <315, oriented, glucose <300 |
| Mortality | 1-5% | 15-25% (much higher) |
| Anticoagulation | Not routine | Yes - prophylactic heparin |
| Seizure treatment | Standard | Benzodiazepines (avoid phenytoin) |
- Rosen's Emergency Medicine, pp. 2546-2547
- Harrison's Principles of Internal Medicine (22e), pp. 3262-3263
- Washington Manual of Medical Therapeutics, pp. 892-893
- Goldman-Cecil Medicine, p. 1302
I just read that there's a way that we can, uh, run insulin via a Macrodrip set, if we use 500 ml NS, and in that, we add 25 units of insulin and run it at 100 ml per hour. Is this ture?
insulin infusion 25 units 500ml NS 100ml/hr DKA macrodrip formulation
Is the 25 units in 500 mL NS at 100 mL/h formulation correct?
The Math First
Concentration = 25 units ÷ 500 mL = 0.05 units/mL
Dose delivered = 0.05 units/mL × 100 mL/h = 5 units/h
0.1 × 50 = 5 units/h ✓
Target = 0.1 × 70 = 7 units/h At 100 mL/h with this formulation = only 5 units/h - that is underdosing by 2 units/h
Where Does This Formulation Come From?
"Larger volumes of an insulin and isotonic sodium chloride solution mixture can be used, providing that the infusion dose of insulin is similar. Larger volumes may be easier in the absence of an IV infusion pump — e.g., 60 units of insulin in 500 mL of isotonic sodium chloride solution at a rate of 50 mL/h."
The Three Recognized Standard Formulations
| Formulation | Concentration | Rate for 5 units/h | Rate for 7 units/h | Best for |
|---|---|---|---|---|
| 100 units in 100 mL NS (standard) | 1 unit/mL | 5 mL/h | 7 mL/h | Syringe pump or volumetric pump |
| 60 units in 500 mL NS (Medscape alternative) | 0.12 units/mL | 41.7 mL/h | 58 mL/h | Gravity/macrodrip when pump unavailable |
| 25 units in 500 mL NS (your formulation) | 0.05 units/mL | 100 mL/h (only works for ~50 kg) | 140 mL/h | Only practical for small/light patients |
The Problem With the 25-units-in-500 mL Formulation
Bottom Line
| Verdict | |
|---|---|
| Is the concept valid? | Yes - diluting insulin into larger volumes to achieve a countable gravity drip rate is an accepted resource-limited technique |
| Does the math check out? | Only for a ~50 kg patient. For any other weight, you are over- or under-dosing |
| Is it the standard formulation? | No - the standard is 100 units/100 mL (1 unit/mL) via pump |
| Is it safe as a routine practice? | Not recommended as routine - the fluid volume load, adsorption losses, and inability to weight-adjust make it inferior to pump-based delivery |
| When is it acceptable? | Pump unavailable, patient ~50 kg, and you know exactly what dose you are delivering |
How do we classify DKA as mild, moderate, and severe?