Purpose of needle and curvature use
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Now I have rich textbook content and diagrams. Here is a thorough answer:
Surgical Suturing Needles: Purpose and Curvature
Overview of Needle Design
A suturing needle has three main components: the point, the body, and the swage (where the suture attaches). Each component is designed with specific function in mind. The needle must pass through tissue smoothly, maintain structural integrity under force, and exit cleanly without causing unnecessary damage.
Needle Body Shape (Curvature)
The curvature of the needle body determines how the needle tracks through tissue during a suture pass. Force during needle placement must always be applied in the direction of the curvature - the wrist is everted and supinated as the needle passes through tissue to avoid bending or breaking it.
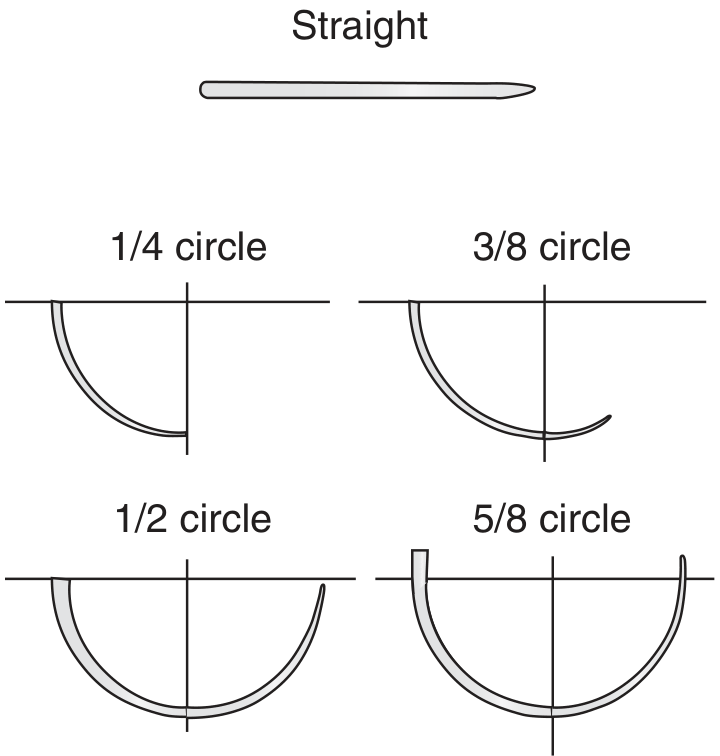
Needle body shapes - from straight to 5/8 circle (Pfenninger & Fowler's Procedures for Primary Care)
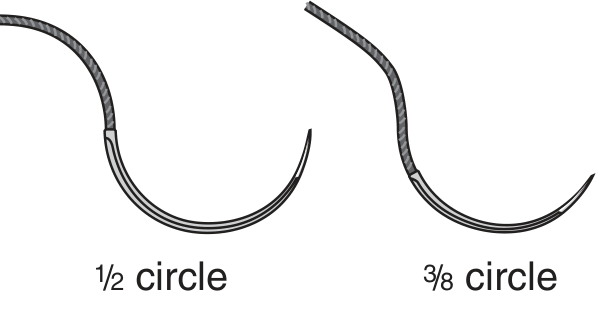
1/2 circle and 3/8 circle needles used for most traumatic wound closures (Roberts & Hedges' Clinical Procedures in Emergency Medicine)
Curvature Types and Their Uses
| Curvature | Description | Clinical Use |
|---|---|---|
| Straight | No curve | Accessible, superficial tissue; tendon repair |
| 1/4 circle | Shallow arc | Ophthalmic surgery, microsurgery |
| 3/8 circle | Moderate arc | Most cutaneous procedures - the standard for skin closure |
| 1/2 circle | Half arc | Deep or confined spaces; abdominal wall, GI tract, urologic surgery |
| 5/8 circle | Deep arc | Very confined spaces (e.g., pelvis, oral cavity, urethral anastomosis) |
| Double curvature | S-shaped curve | Narrow, deep wounds - easier to maneuver |
"In general, a 3/8-inch curvature is adequate for most cutaneous procedures."
- Pfenninger & Fowler's Procedures for Primary Care
The principle: the more confined and deep the operative field, the greater the curvature needed. More curved needles allow a full pass through tissue without requiring much lateral hand movement - critical in tight spaces like the pelvis or oral cavity.
A flattened body with concave or convex surfaces is used to reduce unwanted needle rotation while suturing, improving control.
Needle Point Types
The point type is arguably the most important needle consideration, as it determines how the needle interacts with tissue.
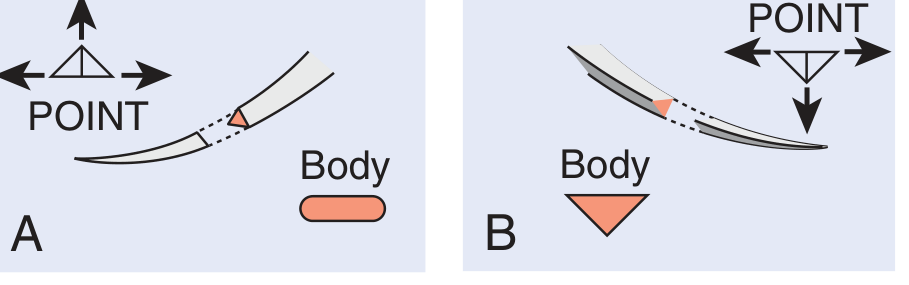
A = conventional cutting needle (third edge on inner curvature). B = reverse cutting needle (third edge on outer curvature) (Roberts & Hedges')
Three Main Point Types
1. Cutting Needles
- Have two opposing cutting edges, plus a third edge
- Conventional cutting: third edge is on the inner (concave) curvature
- Reverse cutting: third edge is on the outer (convex) curvature - preferred for tough tissue like fascia and skin, as the cut is directed away from the wound edge, reducing the risk of tissue tear-through
- Ideal for skin, fascia, and other dense structures
- A drawback: cutting edges can damage tendons and oral mucous membranes if not chosen carefully
2. Tapered (Round-Bodied) Needles
- No cutting edges; penetrate by separating tissue fibers rather than cutting them
- Used for soft, friable, or vascular tissues - bowel, peritoneum, blood vessels, nerve repair
- Less tissue trauma; tissue closes around the suture track
3. Blunt-Point Needles
- Used for friable parenchymal tissue such as liver and kidney
- Allows dissection through tissue without the trauma of a cutting needle
- Also used where accidental needle-stick protection is desired (e.g., in HIV-positive patients)
Needle Holder Technique and Curvature
Proper technique is directly tied to needle curvature:
- The needle holder should grasp the needle below the shank, at the mid-to-distal body - not at the swage (which is soft and will bend) and not at the tip
- Handle closed only to the first or second ratchet to avoid weakening the metal
- Drive the needle by following the arc of its curvature with a pronation-supination wrist motion
"During needle placement the force must be advanced in the direction of the curvature of the needle. The wrist must be everted and supinated as the needle goes through tissue to avoid undue pressure and bending."
- Pfenninger & Fowler's Procedures for Primary Care
Summary
| Situation | Recommended Curvature | Recommended Point |
|---|---|---|
| Skin laceration repair | 3/8 circle | Reverse cutting |
| Deep abdominal wall | 1/2 circle | Reverse cutting or tapered |
| Pelvis/oral cavity | 5/8 circle | Tapered or cutting |
| Bowel/vascular anastomosis | 1/2 circle | Tapered (round-bodied) |
| Liver/kidney | Any | Blunt |
| Ophthalmic/microsurgery | 1/4 circle | Tapered or spatulated |
The core principle: curvature = access and control in the operative field; point type = tissue compatibility.
Sources: Pfenninger & Fowler's Procedures for Primary Care, 3rd ed.; Roberts & Hedges' Clinical Procedures in Emergency Medicine
Compare cutting vs reverse-cutting vs tapered needles
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
That diagram is perfect. Here is a complete comparison:
Cutting vs. Reverse Cutting vs. Tapered Needles
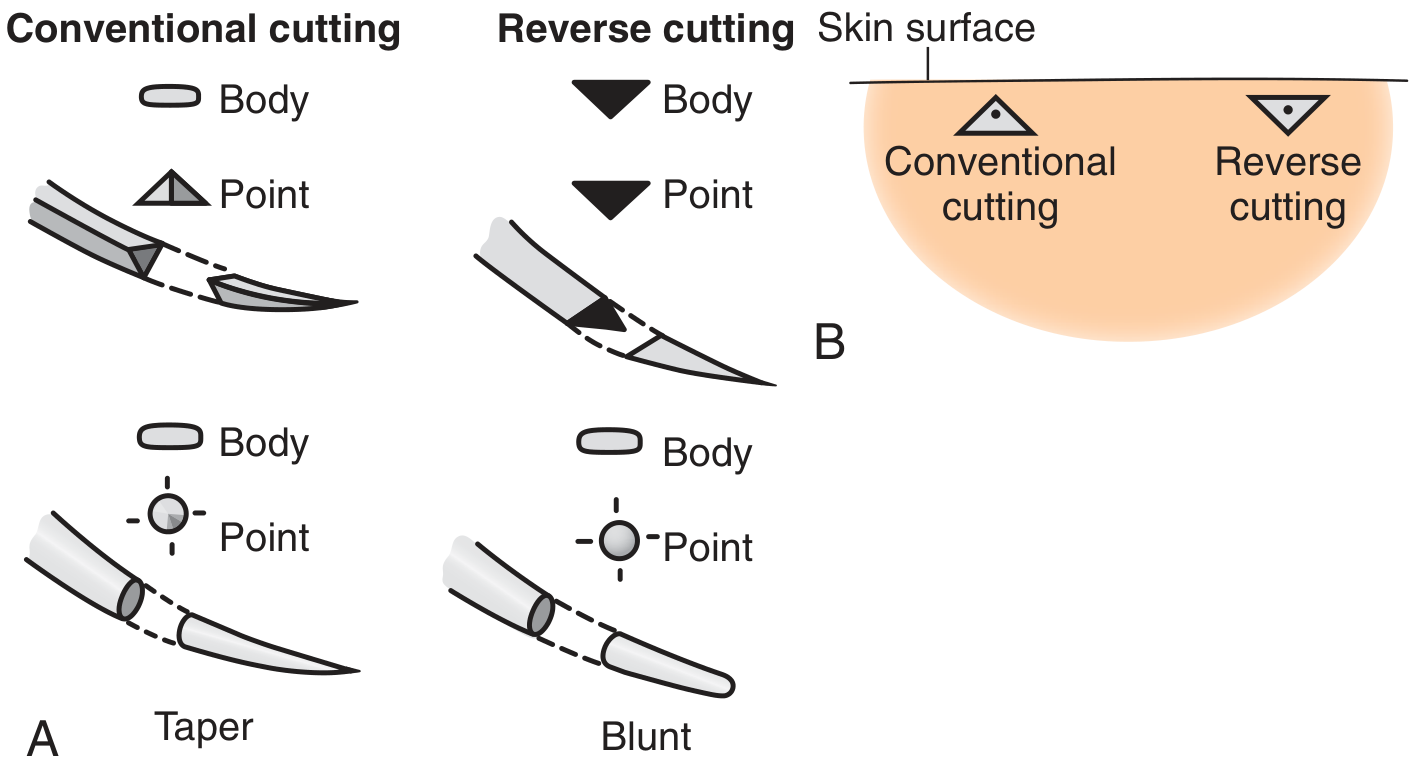
A: Cross-sections and profiles of all four point types. B: Comparison of suture channel orientation in skin for conventional vs. reverse cutting.
1. Conventional Cutting Needle
Structure:
- Triangular cross-section with 3 cutting edges
- The third (apex) edge faces the inside (concave) curvature of the needle
- Body transitions from triangular tip to a flattened profile
Mechanism:
- As the needle passes through tissue, the inner apex cuts directly toward the wound edge - in the direction of suture tension
- The suture force concentrates at the apex of the triangle, causing the needle to cut outward through the tissue margin
The key problem: Because the cut faces the wound edge, the suture has a tendency to tear through tissue when tension is applied - the suture track is oriented in the most vulnerable direction.
Uses: Now largely superseded by reverse cutting for most applications. Still found in ophthalmic surgery and certain delicate procedures.
2. Reverse Cutting Needle
Structure:
- Also has 3 cutting edges in a triangular cross-section
- The third edge faces the outside (convex) curvature of the needle
- Triangular shape extends all the way from point to swage; only the edges near the tip are sharpened
Mechanism:
- The inner surface of the needle is flat - this flat surface faces the wound edge
- When the suture is tensioned, force is distributed across the broad flat base of the triangle, not concentrated at a sharp apex
- The cut is oriented away from the wound edge, so the tissue between the suture and the wound margin is much less likely to tear
Advantages over conventional cutting:
- Significantly reduces suture pull-through and tissue tearing
- Still cuts through tough, dense tissue easily
- The flat inner surface creates a more stable suture track
Uses: The standard for skin, fascia, and any dense connective tissue. When a "cutting needle" is specified today without further qualification, reverse cutting is almost always what is meant.
"The reverse cutting needle has its cutting edge on the outer curvature of the needle. This provides a flat surface along the inner edge, thereby reducing the incidence of sutures pulling through tissues into the margin of the wound. Unless specified otherwise, a 'cutting needle' now refers to a reverse cutting design."
- Pfenninger & Fowler's Procedures for Primary Care, 3rd ed.
3. Tapered (Round-Bodied) Needle
Structure:
- Circular cross-section throughout the body
- Smooth, round body that tapers to a sharp point - no cutting edges at all
- Oval body reduces twisting in the needle holder
Mechanism:
- The needle does not cut tissue - it separates and pushes apart tissue fibers
- The tissue closes snugly around the suture after the needle passes, creating a watertight seal around the thread
- Minimal trauma to tissue architecture
Advantages:
- Less tissue trauma and inflammation
- The suture hole seals around the thread, reducing leakage (critical for bowel, vessels)
- Lower risk of accidental cutting of fragile structures
Disadvantage:
- Cannot penetrate tough, dense tissue - requires significantly more force on resistant structures, which risks needle bending or deflection
Uses: Bowel, peritoneum, GI anastomoses, cardiovascular surgery, nerve repair, fascia (when tissues are pliable), and any soft tissue where minimal trauma matters.
"Round-bodied needles are designed to separate tissue fibres rather than cut through them and are commonly used in intestinal and cardiovascular surgery."
- Bailey & Love's Short Practice of Surgery, 28th ed.
Head-to-Head Comparison
| Feature | Conventional Cutting | Reverse Cutting | Tapered (Round) |
|---|---|---|---|
| Cutting edges | 3 (apex on inner curve) | 3 (apex on outer curve) | None |
| Body cross-section | Triangular | Triangular | Circular |
| Tissue action | Cuts | Cuts | Separates fibers |
| Suture track | Open toward wound edge | Open away from wound edge | Closes around suture |
| Tear-through risk | High | Low | Very low |
| Penetration force needed | Low | Low | High (on dense tissue) |
| Primary use | Largely obsolete; some ophthalmic | Skin, fascia, tendons | Bowel, vessels, peritoneum |
| Contraindicated in | Most skin closures (risk of tear-through) | Bowel, vessels | Skin, fascia (too tough) |
Special Variants Worth Knowing
- Taper-cut (tapercut): Hybrid - tapered body with a short cutting tip. Combines the penetrating power of a cutting needle through tough outer layers with the tissue-separating action of a taper for deeper passage. Used for calcified tissue, dense fascia, sternal closure.
- Blunt point: No sharp tip at all - pushes through friable parenchyma (liver, kidney) without cutting. Also advocated for abdominal wall closure to reduce needlestick injuries.
- Spatulated (side-cutting): Flat on top and bottom, cutting edges on the sides - used almost exclusively in ophthalmic surgery to pass parallel to tissue layers.
Sources: Pfenninger & Fowler's Procedures for Primary Care, 3rd ed.; Roberts & Hedges' Clinical Procedures in Emergency Medicine; Bailey & Love's Short Practice of Surgery, 28th ed.
This is a shared conversation. Sign in to Orris to start your own chat.