Anal canal gross anatomy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed for a comprehensive answer. Let me compile the full response.
Anal Canal - Gross Anatomy
Overview and Extent
The anal canal is the terminal segment of the gastrointestinal tract. It begins at the anorectal junction (where the rectum narrows at the pelvic floor) and terminates at the anal orifice (anus) after passing through the perineum. It measures 2.5 to 4 cm in length (generally longer in men than in women).
Two definitions are used clinically:
- Surgical (functional) anal canal: from the anorectal ring to the anal verge (~4 cm)
- Anatomical anal canal: from the dentate/pectinate line to the anal verge (~2 cm)
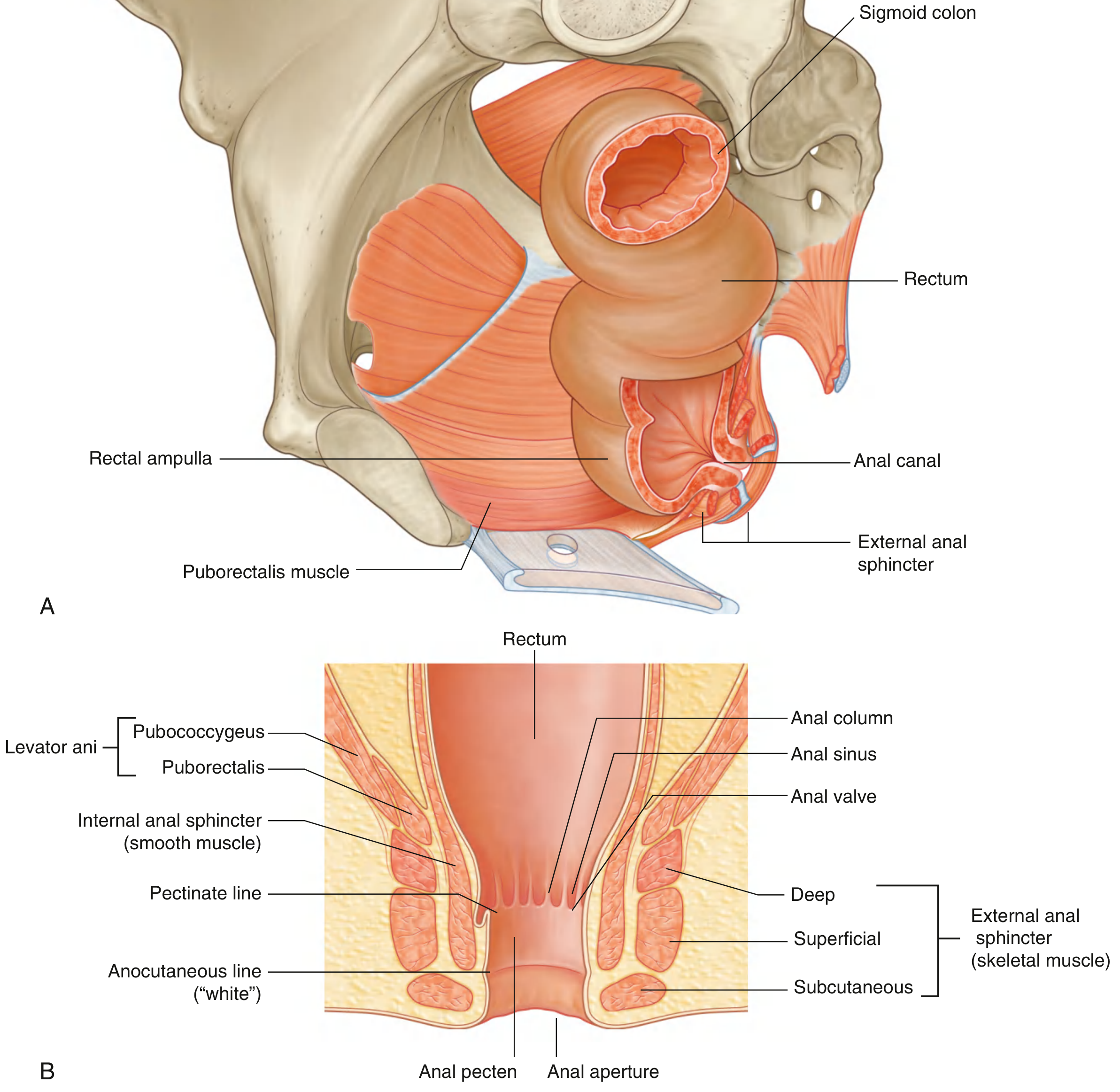
Fig. 1 - Rectum and Anal Canal (Gray's Anatomy for Students, longitudinal section)
Lining / Mucosal Zones
The lining changes progressively from above downward, reflecting the embryological fusion of endoderm and ectoderm at the cloacal membrane:
| Zone | Location | Epithelium |
|---|---|---|
| Proximal zone | Above dentate line (~1-2 cm) | Columnar (rectal mucosa) |
| Transition zone (ATZ) | Just above dentate line | Mixed columnar, cuboidal, squamous |
| Anal pecten / anoderm | Dentate line to anocutaneous line | Non-keratinized stratified squamous |
| Anal margin | Below anocutaneous line ("white line") | True skin (keratinized, with hair) |
Key Surface Features (Above the Dentate Line)
- Anal columns (Columns of Morgagni): 8-12 vertical mucosal folds in the upper anal canal, containing terminal branches of the superior rectal artery and the internal rectal (hemorrhoidal) plexus.
- Anal valves: Crescentic transverse folds connecting the lower ends of adjacent anal columns.
- Anal sinuses: Small depressions (pockets) located superior to each anal valve.
- Anal crypts: Recesses at the anal valves where the anal glands open. These glands are the origin of most cryptoglandular abscesses and fistulae.
- Anal papillae: Folds of tissue at the dentate line, between the crypts.
Key Landmarks
- Dentate (pectinate) line: Formed by the row of anal valves. Marks the approximate site of the embryological cloacal membrane and the boundary between endodermal and ectodermal territory. This is the single most important landmark of the anal canal - blood supply, venous/lymphatic drainage, and innervation all change at this line.
- Anocutaneous line ("white line" of Hilton): The lower boundary of the anal pecten, where stratified squamous epithelium transitions to true skin.
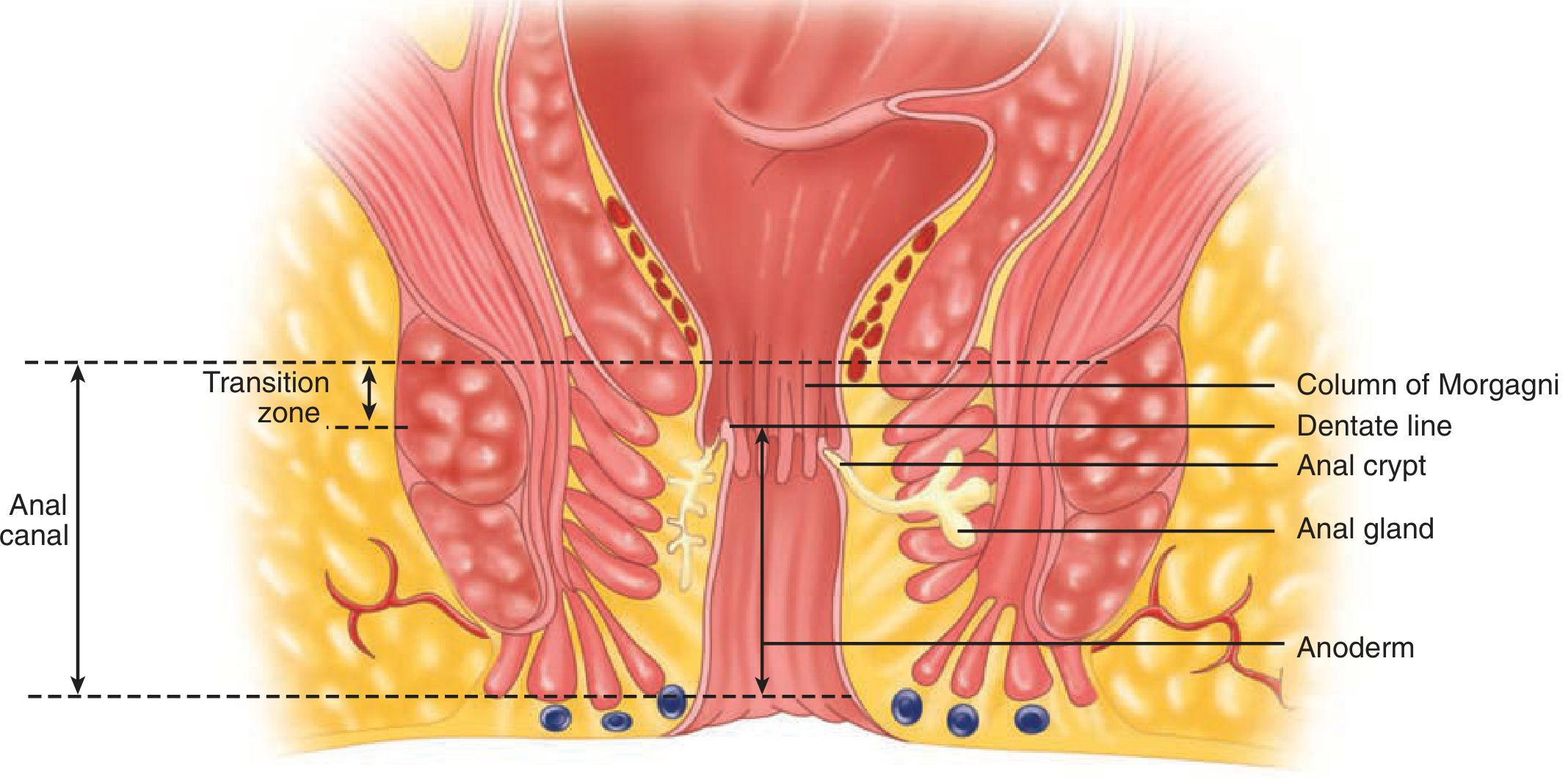
Fig. 2 - Lining zones and cryptoglandular structures (Schwartz's Principles of Surgery)
Sphincter Complex and Pelvic Floor
The anal canal is enclosed along its entire length by two sphincters, which maintain it in a closed resting state.
Internal Anal Sphincter (IAS)
- A thickening of the circular smooth muscle layer of the rectal wall, extending 2-4 cm.
- Involuntary, supplied by autonomic nerves (sympathetic and parasympathetic - both inhibit contraction, i.e., both promote relaxation).
- Responsible for approximately 85% of resting anal tone.
External Anal Sphincter (EAS)
- Striated (skeletal) voluntary muscle, surrounding and overlapping the IAS.
- Divided into three parts: deep, superficial, and subcutaneous.
- Contiguous superiorly with the levator ani and puborectalis; attached inferiorly to the coccyx via the anococcygeal ligament.
- Supplied by the inferior rectal branch of the pudendal nerve (S2, S3).
Longitudinal Muscle
- The "conjoined longitudinal muscle" lies between the IAS and EAS in the intersphincteric plane. It is formed by extensions of the rectal longitudinal muscle blended with fibres from levator ani. Its terminal fibres fan out as the corrugator cutis ani, which create the puckered appearance of the anus.
Puborectalis and the Levator Ani
- The levator ani muscle (pubococcygeus, puborectalis, iliococcygeus) forms the pelvic floor.
- Puborectalis forms a U-shaped sling around the anorectal junction, passing from the posterior pubis around the back of the rectum. This creates the anorectal angle (~90°), a key mechanism of continence.
- The deep part of the EAS is essentially fused with the puborectalis.
Intersphincteric Space
- The space between the IAS and EAS. This is the most common pathway for the spread of cryptoglandular infection (abscess and fistula formation).
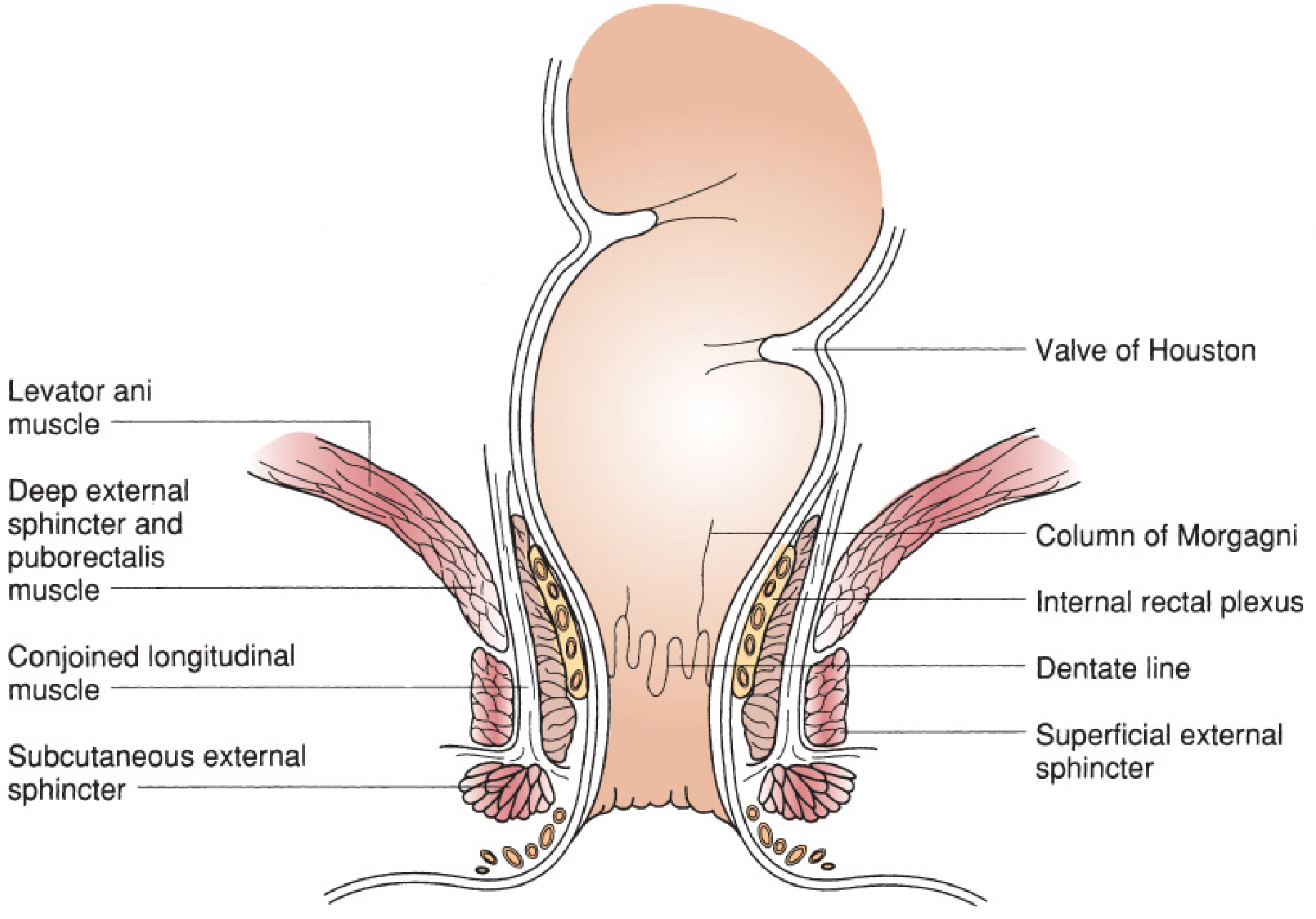
Fig. 3 - Anatomy of the anal canal (Mulholland & Greenfield's Surgery)
Anorectal Spaces
Several potential spaces surround the anal canal and are clinically relevant to abscess spread:
| Space | Contents / Notes |
|---|---|
| Perianal space | External haemorrhoids, subcutaneous EAS, distal IAS; communicates with intersphincteric space |
| Intersphincteric space | Between IAS and EAS; most common path for cryptoglandular infection |
| Ischioanal (ischiorectal) space | Largest; between ischial tuberosities laterally and levator ani superiorly; communicates posteriorly |
| Postanal / postrectal space | Behind anus and rectum; limited by anococcygeal ligament; infections here spread laterally, creating horseshoe abscesses |
Blood Supply
The anal canal has a dual blood supply above and below the dentate line:
Arterial:
- Superior rectal artery (terminal branch of inferior mesenteric artery): supplies the upper anal canal and rectum. Descends posterior to the rectum and bifurcates.
- Middle rectal arteries (from internal pudendal or inferior gluteal arteries, branches of internal iliac): present as a distinct vessel in fewer than 15% of people; supply the lower rectum and upper anal canal.
- Inferior rectal arteries (from internal pudendal artery, within Alcock's canal): traverse the ischioanal space to supply the anal sphincters and lower canal.
- Median sacral artery: provides additional supply to the posterior anal canal and IAS.
Venous:
- Superior rectal vein → inferior mesenteric vein → portal system
- Middle and inferior rectal veins → internal iliac veins → systemic (caval) system
- This portosystemic communication is the anatomical basis for rectal varices in portal hypertension.
- The haemorrhoidal plexus (internal rectal plexus) is a submucosal plexus deep to the columns of Morgagni - a sinusoidal (not true venous) network draining into all three rectal veins.
Lymphatic Drainage
The dentate line is the critical landmark:
| Level | Drainage |
|---|---|
| Above dentate line | Along superior rectal vessels → inferior mesenteric nodes → para-aortic nodes |
| Above dentate line (lower) | May also drain along middle rectal vessels → internal iliac nodes |
| Below dentate line | Superficial → deep inguinal lymph nodes |
This has critical clinical significance: carcinoma above the dentate line spreads to pelvic/para-aortic nodes, while carcinoma below it may first present with inguinal lymphadenopathy.
Nerve Supply
Again divided at the dentate line:
| Level | Innervation | Sensitivity |
|---|---|---|
| Above dentate line | Autonomic (sympathetic: L1-L3 via hypogastric plexus; parasympathetic: S2-S4 via pelvic splanchnic / nervi erigentes) | Insensate to pain/touch (visceral) |
| Below dentate line | Somatic - inferior rectal branch of pudendal nerve (S2-S4) | Exquisitely sensitive to pain, touch, temperature |
- IAS: autonomic innervation; both sympathetic and parasympathetic fibres inhibit (relax) the sphincter.
- EAS and puborectalis: inferior rectal branch of internal pudendal nerve.
- Levator ani: pudendal nerve + direct branches from S3-S5.
This explains why procedures below the dentate line (e.g., injection of haemorrhoids) must use local anaesthetic, while those above the dentate line can be performed without anaesthesia.
Summary: Clinical Significance of the Dentate Line
| Feature | Above dentate line | Below dentate line |
|---|---|---|
| Embryology | Endoderm (hindgut) | Ectoderm (proctodeum) |
| Epithelium | Columnar/transitional | Squamous |
| Arterial supply | Superior rectal a. | Inferior rectal a. |
| Venous drainage | Portal (sup. rectal v.) | Systemic (inf. rectal v.) |
| Lymphatics | Para-aortic / pelvic nodes | Inguinal nodes |
| Innervation | Autonomic (visceral) | Somatic (pudendal) |
| Sensitivity | Pain insensate | Pain sensitive |
| Haemorrhoids | Internal | External |
Sources: Gray's Anatomy for Students, p. 535-536 | Mulholland & Greenfield's Surgery 7e, p. 3533-3535 | Schwartz's Principles of Surgery 11e, p. 1288-1290 | Fischer's Mastery of Surgery 8e, p. 3999-4003 | Bailey & Love's Short Practice of Surgery 28e
This is a shared conversation. Sign in to Orris to start your own chat.