Hello
Hello! I'm Orris. How can I help you today?
Can u please explain parkinson with it’s pathophysiology and features with its cause in a proper 10 marker for mbbs from standard book
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material from Adams and Victor's Principles of Neurology (12th Edition) and Bradley and Daroff's Neurology. Let me compile the full 10-marker answer.
Parkinson's Disease - 10 Marker (MBBS Standard)
(Source: Adams and Victor's Principles of Neurology, 12th Ed. & Bradley and Daroff's Neurology in Clinical Practice)
Definition
Parkinson's Disease (PD) is a progressive neurodegenerative disorder characterized by the classic tetrad of bradykinesia, resting tremor, rigidity, and postural instability, first described by James Parkinson in 1817 as "involuntary tremulous motion with lessened muscular power and propensity to bend the trunk forward."
Epidemiology
- Peak onset: 6th decade (45-70 years); rare before 30 years
- Affects ~1% of population over 65 years
- Slightly more common in males
- Universal in all ethnic groups; incidence in Asians is one-third to one-half that in whites
Etiology / Causes
PD is broadly classified as:
1. Idiopathic (Most Common)
- No identifiable cause; multifactorial (genetic + environmental)
2. Genetic Causes (Familial PD)
| Gene | Inheritance | Notes |
|---|---|---|
| SNCA (α-synuclein) - PARK1/4 | Autosomal Dominant | Mutations A53T, A30P promote synuclein oligomerization |
| PARK2 (parkin) | Autosomal Recessive | 50% of early-onset inherited PD; no Lewy bodies |
| PINK1 (PARK6) | Autosomal Recessive | Mitochondrial gene |
| DJ-1 (PARK7) | Autosomal Recessive | Oxidative stress pathway |
| LRRK2 (PARK8) | Autosomal Dominant | Most common hereditary PD; especially Ashkenazi Jews |
3. Environmental / Toxic Causes
- MPTP (1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine): A meperidine analogue used by drug addicts; converted by MAO-B to MPP+, which selectively destroys dopaminergic neurons in substantia nigra
- Pesticides / organophosphates: Slight increased incidence in agrarian regions
- Heavy metals, iron deposition in substantia nigra
4. Post-encephalitic Parkinsonism
- Following encephalitis lethargica; neurofibrillary tangles rather than Lewy bodies
Pathology
Gross
- Pallor of substantia nigra (visible to naked eye) due to loss of neuromelanin-containing pigmented neurons
Microscopic
- Loss of pigmented dopaminergic neurons in the substantia nigra pars compacta - reduced to 30% or less of age-matched controls (>66% reduction in absolute numbers)
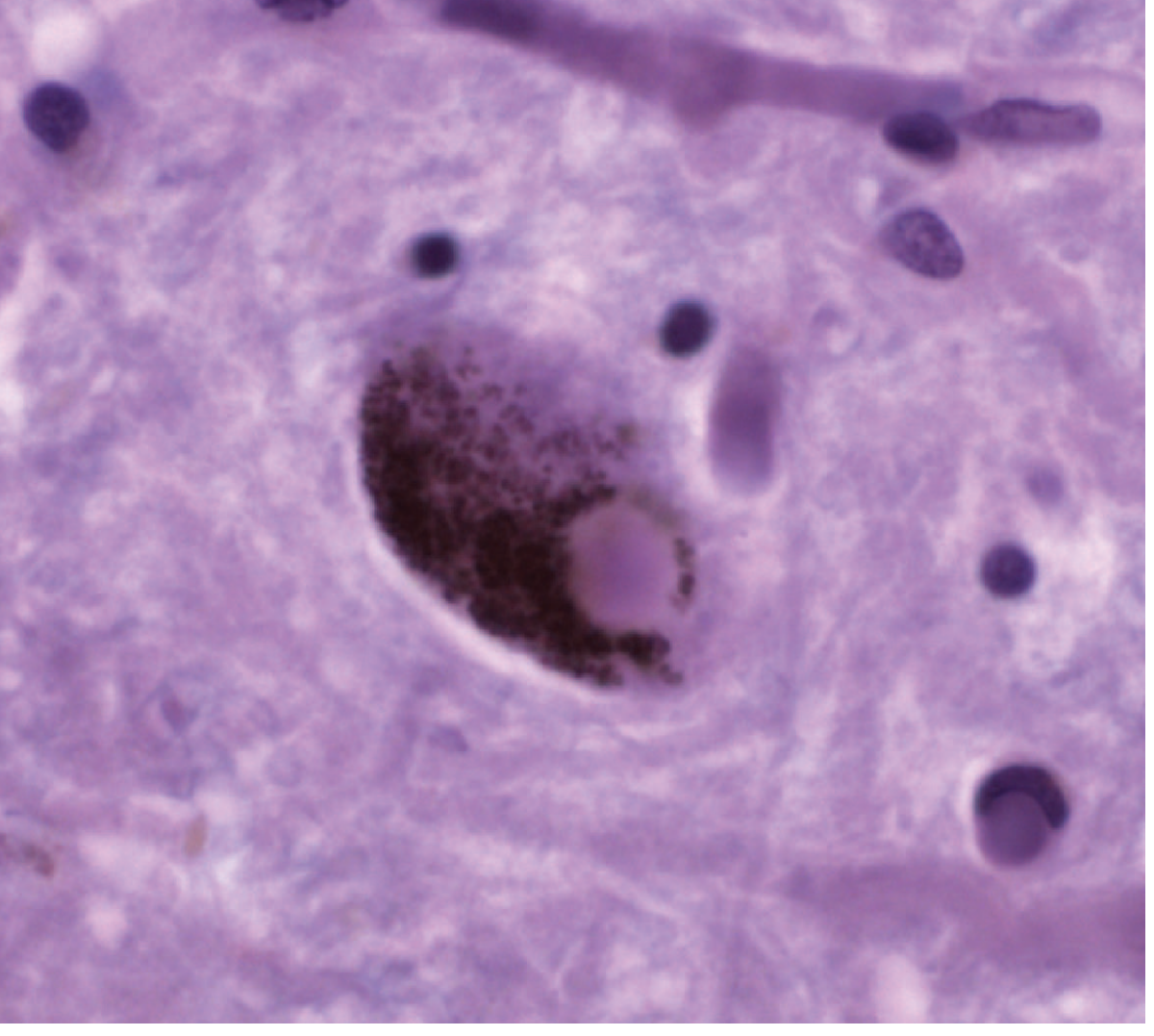
- Lewy bodies: Eosinophilic cytoplasmic inclusions with a faint halo, seen in practically all idiopathic cases - the hallmark of PD
- Neuronal loss also occurs in: locus ceruleus, dorsal motor nucleus of vagus, sympathetic ganglia, putamen, pallidum
Pathophysiology
Normal Basal Ganglia Circuit
- Substantia nigra pars compacta → releases dopamine → acts on striatum (putamen + caudate)
- Direct pathway: D1 receptors → facilitates movement (excitatory)
- Indirect pathway: D2 receptors → inhibits movement
In Parkinson's Disease
Loss of nigral dopaminergic neurons
↓
Reduced dopamine in striatum
↓
Direct pathway UNDERACTIVE + Indirect pathway OVERACTIVE
↓
Globus pallidus internus (GPi) becomes HYPERACTIVE
↓
Thalamus INHIBITED (excessive inhibition)
↓
Reduced thalamocortical drive
↓
BRADYKINESIA + AKINESIA + RIGIDITY
Molecular Mechanism - α-Synuclein Toxicity
- Mutant/misfolded α-synuclein aggregates form Lewy bodies
- Normal α-synuclein is degraded by ubiquitin-proteasome system
- Dysfunction of parkin (E3 ubiquitin ligase) → impaired protein clearance → accumulation
- Mitochondrial dysfunction (PINK1, DJ-1 mutations) → oxidative stress → neuronal death
Clinical Features
Cardinal Motor Features (TRAP)
| Feature | Description |
|---|---|
| T - Tremor | Resting "pill-rolling" tremor (4-6 Hz), disappears with voluntary movement; most common presenting symptom (70%) |
| R - Rigidity | "Lead-pipe" rigidity or "cogwheel" rigidity (rigidity + tremor); affects all muscle groups |
| A - Akinesia/Bradykinesia | Slowness, poverty of movement; expressionless "mask-like" facies; micrographia |
| P - Postural instability | Stooped posture; impaired righting reflexes; festinating gait (short, shuffling, accelerating steps) |
Non-Motor Features
- Autonomic: Constipation, orthostatic hypotension, sialorrhea (drooling), urinary dysfunction, sexual dysfunction
- Neuropsychiatric: Depression (most common non-motor feature), anxiety, dementia (late), psychosis
- Sleep: REM sleep behavior disorder (can precede motor symptoms by years), insomnia
- Sensory: Anosmia (often an early sign), pain
- Speech: Hypophonia (soft voice), dysarthria, dysphagia
Early vs Late Features
- Early: Unilateral tremor, anosmia, constipation, depression, REM sleep disorder
- Late: Bilateral involvement, dementia, falls, autonomic failure, dysphagia
Gait in PD
- Short shuffling steps, reduced arm swing
- Festination: involuntary acceleration of gait
- Freezing of gait: sudden inability to initiate steps
- Difficulty turning; en-bloc turning
Hoehn and Yahr Staging
| Stage | Description |
|---|---|
| I | Unilateral disease only |
| II | Bilateral disease, no postural impairment |
| III | Bilateral disease + mild postural instability |
| IV | Severely disabling, can walk unaided |
| V | Wheelchair bound or bedridden |
Diagnosis
Primarily clinical based on TRAP features. Supportive imaging: DaTscan (dopamine transporter SPECT) shows reduced uptake in striatum.
Summary Box (for quick recall)
PD = Progressive loss of dopaminergic neurons in substantia nigra pars compacta → reduced dopamine → overactive indirect pathway → TRAP (Tremor, Rigidity, Akinesia, Postural instability). Pathological hallmark = Lewy bodies (α-synuclein aggregates). Mainly idiopathic; genetic causes include SNCA, PARK2, LRRK2.
Sources: Adams and Victor's Principles of Neurology, 12th Ed.; Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.