Posterior one third of tongue carcinoma answer from Scott and brown textbook
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
I now have all the information needed. Let me compile the comprehensive answer from Scott-Brown's Otorhinolaryngology Head & Neck Surgery.
Carcinoma of the Posterior One-Third of the Tongue (Base of Tongue)
Source: Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Anatomy
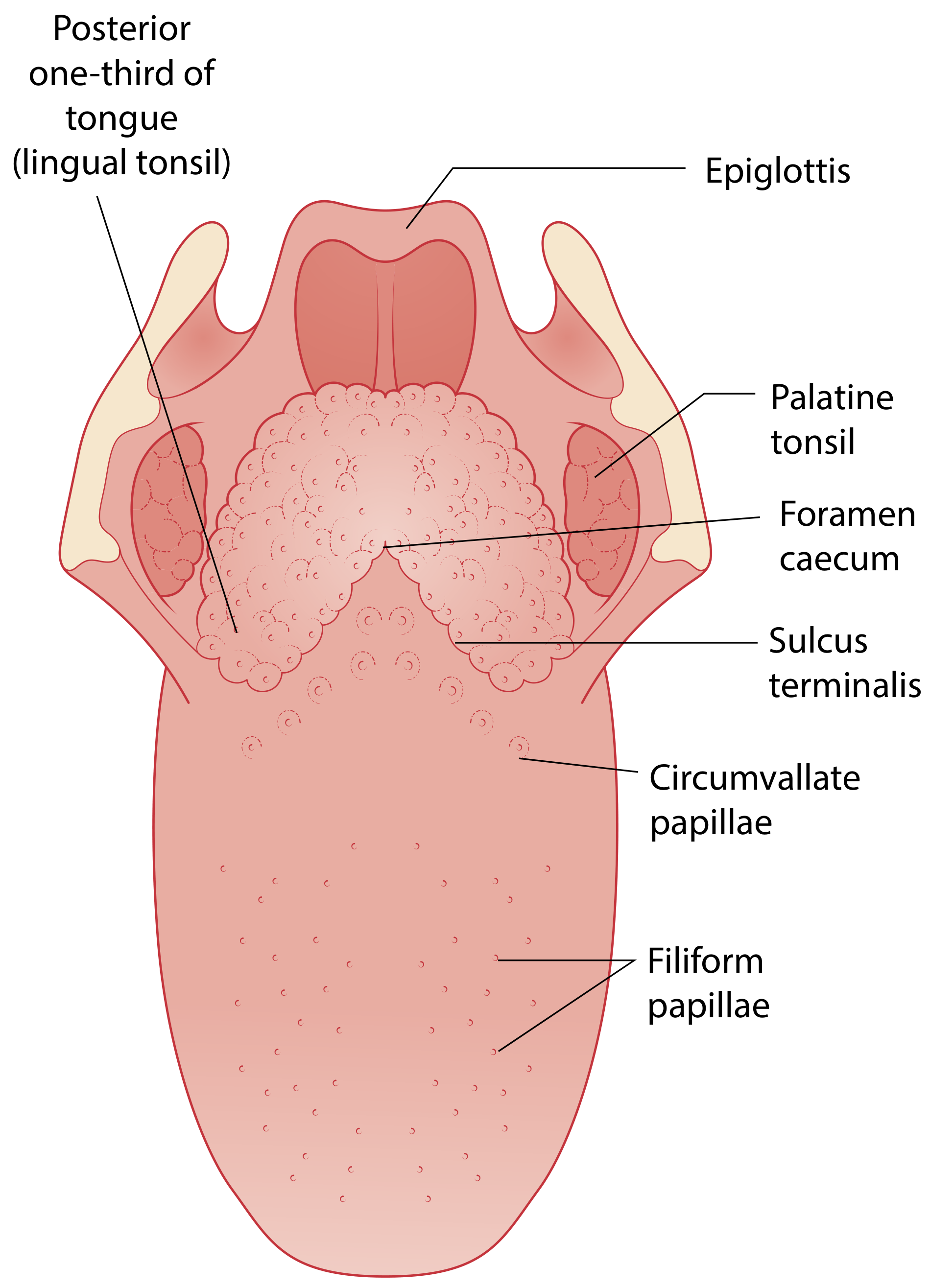
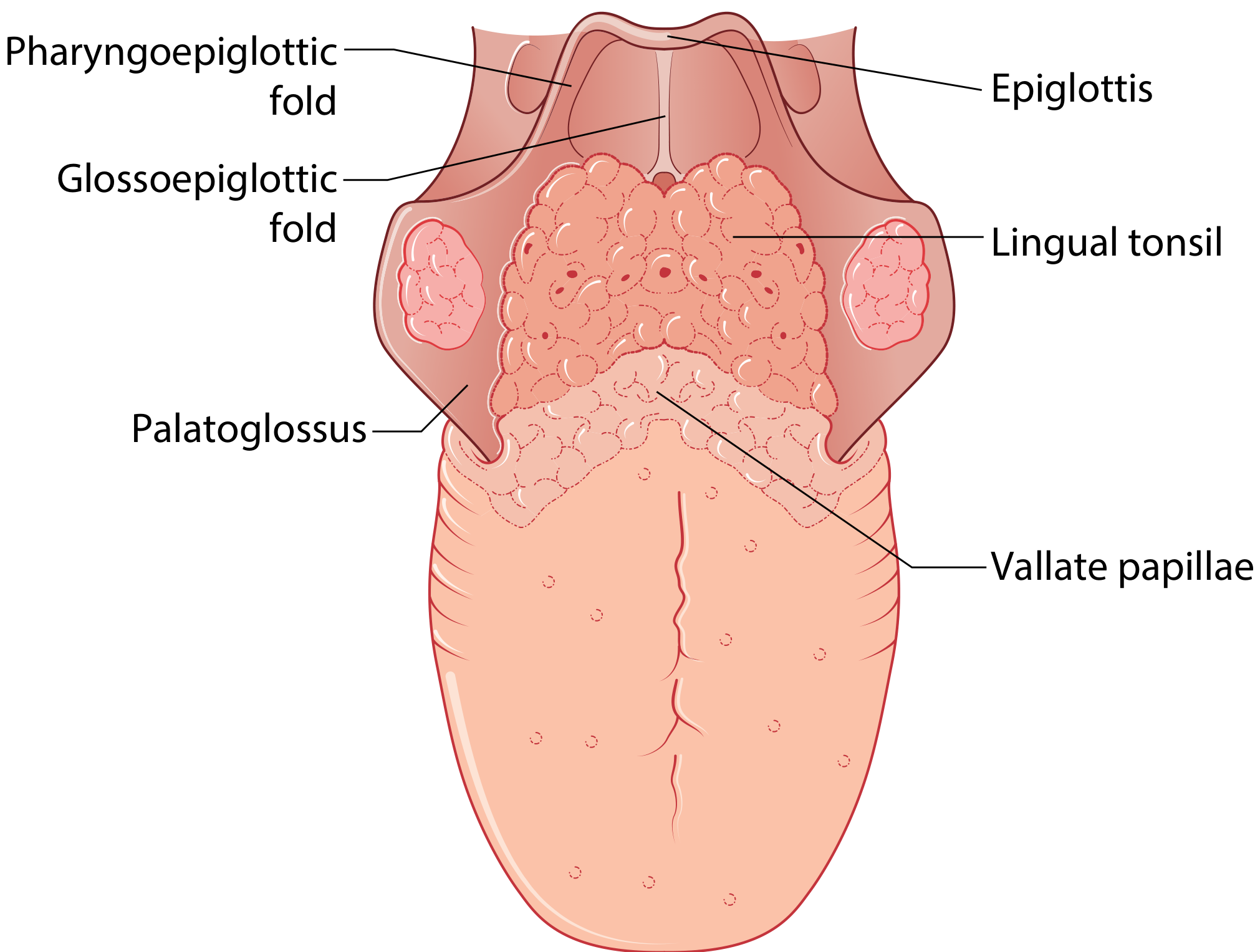
The posterior one-third of the tongue (base of tongue) is part of the oropharynx - not the oral cavity. It is separated from the anterior two-thirds (oral tongue) by the circumvallate (vallate) papillae and the sulcus terminalis. According to the Scott-Brown classification, it falls under the oropharynx and is bounded:
- Anteriorly: anterior palatoglossal folds (vertical plane)
- Superiorly: horizontal line at the level of the hard palate
- Inferiorly: floor of the valleculae
The tongue base is derived from the 2nd, 3rd and 4th branchial arches and contains the lingual tonsils as well as the pharyngoepiglottic and glossoepiglottic folds.
Innervation of the posterior third:
- Sensation (general and taste): Glossopharyngeal nerve (CN IX) - via lingual branches providing common sensation, taste, and secretomotor supply
- Near the vallecula/epiglottis: Internal laryngeal nerve (branch of vagus)
Lymphatic drainage: The tongue base drains bilaterally to cervical nodes (midline structure), unlike the lateral borders of the oral tongue which drain ipsilaterally.
Vascular anatomy relevant to surgery: The lingual artery lies approximately 2.7 cm inferior and 1.6 cm lateral to the foramen cecum; its main trunk runs on the lateral surface of the genioglossus muscle.
Classification (TNM Staging - UICC/AJCC)
Scott-Brown's notes that the 8th edition staging separates oropharyngeal carcinoma into two distinct entities:
p16-Negative (non-HPV-associated) OPC
| Stage | Criteria |
|---|---|
| T1 | Tumour ≤2 cm in greatest dimension |
| T2 | Tumour >2 cm but ≤4 cm |
| T3 | Tumour >4 cm or extension to lingual surface of epiglottis |
| T4a | Invades larynx, deep extrinsic tongue muscles, medial pterygoid, hard palate, or mandible |
| T4b | Invades lateral pterygoid, pterygoid plates, lateral nasopharynx, skull base, or encases carotid |
p16-Positive (HPV-associated) OPC
- No Tis category (due to non-aggressive pattern of invasion and lack of distinct basement membrane in Waldeyer's ring epithelium)
- No T4b category (survival curves of T4a and T4b are indistinguishable in HPV-positive disease)
Epidemiology and Aetiology
- Base of tongue carcinomas are among the most common oropharyngeal subsites for malignancy
- The palatine tonsils and base of tongue are specifically described as common sites for HPV-associated squamous cell carcinoma
- HPV-16 has the strongest association with oropharyngeal cancer, especially tonsillar and base-of-tongue cancer
- HPV-positive head and neck SCC is associated with improved prognosis compared to HPV-negative disease
Clinical Features (Presentation)
Tongue base (posterior third) carcinomas are clinically silent and typically present late:
- Lesions of the base of tongue are less symptomatic than oral tongue lesions
- The majority present at Stage III/IV - this contrasts sharply with oral tongue cancers which usually present at Stage I/II
- May spread along the palatoglossal muscle to involve the anterior tonsillar pillar
- May spread along the hyoglossal and mylohyoid muscles to the floor of mouth
- Differentiation from normal lingual lymphoid tissue may be difficult on all cross-sectional imaging
- Can present as a neck mass (unknown primary) - the tongue base is a common occult primary site (PET-CT shows increased activity in the tongue base)
Workup and Investigations
- Clinical examination - difficult due to location; line-of-sight constraints
- CT and MRI - standard cross-sectional imaging; MRI preferred for soft tissue detail (e.g. T2N2b base of tongue carcinoma)
- PET-CT - particularly useful when:
- Presenting with neck nodes and no apparent primary on clinical examination or conventional CT
- Response assessment after chemoradiotherapy (performed at 12-16 weeks post-treatment for highest diagnostic accuracy)
- Note: physiological FDG activity in normal lingual lymphoid tissue can complicate interpretation
- Biopsy - tongue base biopsies may be needed; distinguishing SCC from normal lymphoid tissue can be difficult
- Pre-treatment FDG-tumour uptake - independent prognostic factor; high uptake may indicate better treatment with surgery + post-operative radiotherapy ± chemotherapy
Spread of Tumour
- Local spread: Along palatoglossal muscle to anterior tonsillar pillar; along hyoglossal/mylohyoid muscles to floor of mouth
- Nodal spread: Bilateral cervical lymphadenopathy (midline structure - drains bilaterally)
- Occult cervical metastasis: present in up to 53% of patients with tongue cancer
- Up to 4.5% may have occult disease in the contralateral neck
- Clinical N0 neck management in T1/T2 disease remains a dilemma as CT, MRI, and PET-CT all fail to detect micrometastases reliably
Treatment
Modalities
Oropharyngeal cancer (including base of tongue) is treated with curative intent by:
- Surgery
- Radiotherapy with or without chemotherapy
- Combined surgery + radiotherapy
Surgical Access
Access to the tongue base is challenging compared to the tonsil/soft palate:
- Usually achieved via a bivalved distending oropharyngoscope
- Even then, complete tumour exposure is not guaranteed due to line-of-sight constraints
- Resection proceeds in a superficial to deep direction, appreciating the 3D orientation of the tongue base and vallecula
- Frozen section may be used to distinguish tumour from normal lingual lymphoid tissue
Transoral Laser Microsurgery (TLM) and Transoral Robotic Surgery (TORS)
TORS has become a key modality for tongue base tumours:
- The da Vinci robot provides excellent 3D visualization, immaculate precision, and absence of tremor
- Allows tongue base reduction and management of malignancy with improved access
- Marginal biopsies taken from mucosal edges and deep tissues after resection; zero tolerance for positive margins
- Similar resection principles to tonsillar tumours but marginal biopsy positions are less proscriptive
Surgical Margin
- Resection with 1 cm margin in three dimensions
- Even with apparently adequate margins, 10% of resections may demonstrate histologically positive margins
- For resections of posterior tongue: preserve the contralateral vascular pedicle if tongue tip is to be maintained
Neck Management
- T1/T2 N0: elective neck treatment dilemma (micrometastases unreliably detected by imaging)
- The contralateral N0 neck: staging selective neck dissection may be performed routinely given bilateral lymphatic drainage
- Post-treatment: PET-CT used to guide neck dissection - only performed if residual nodal disease is present
Chemoradiotherapy
- Response to definitive radiotherapy ± chemotherapy is a powerful predictor of outcome
- Perfusion CT can predict response to induction chemotherapy
- Post-treatment PET-CT (at 12-16 weeks) guides decision making on salvage surgery
Prognosis
- Base of tongue tumours have worse prognosis than oral tongue tumours - primarily because they present at advanced stage (Stage III/IV)
- HPV-positive OPC has significantly improved prognosis compared to HPV-negative disease
- This has driven trials of treatment de-escalation in HPV-positive patients to reduce morbidity while maintaining oncological outcomes (e.g. ECOG 3311 trial - transoral surgery followed by low-dose or standard-dose radiotherapy ± chemotherapy in HPV-positive Stage III/IVA OPC)
- Extracapsular nodal spread (identified on imaging by poorly defined nodal margins and surrounding fat stranding) is associated with a 3-5-fold increase in local recurrence
- High pre-treatment FDG uptake on PET-CT is an independent adverse prognostic factor
Source: Scott-Brown's Otorhinolaryngology Head & Neck Surgery, 8th Edition - Chapters on Tongue Carcinoma, Oropharynx, Oropharyngeal Cancer Imaging, Tongue Base Anatomy (TLM/TORS), and TNM Staging.
This is a shared conversation. Sign in to Orris to start your own chat.