Spinal fusion methods
Reading File
Finding Sources
Finding Sources
Searching PubMed
"spinal fusion"[MeSH Terms] AND techniques
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information to give a thorough, well-sourced answer. Let me compile everything.
Spinal Fusion Methods
Spinal fusion (arthrodesis) is a surgical procedure that permanently joins two or more vertebrae, eliminating motion between them. It is performed for fracture stabilization, tumor-related instability, degenerative disc disease, deformity correction (scoliosis/kyphosis), spondylolisthesis, and other mechanical spine disorders.
1. Approaches to Spinal Fusion
Fusion can be performed via three broad surgical routes, which can be combined:
A. Anterior Approach
The surgeon accesses the spine from the front. Used primarily in the cervical spine for Anterior Cervical Discectomy and Fusion (ACDF), and in the lumbar spine for ALIF. Anterior-only constructs are generally avoided in osteoporotic patients due to poor pullout strength and risk of hardware failure.
- Grainger & Allison's Diagnostic Radiology, p. 1312-1313
B. Posterior Approach
The most common route. Provides access for pedicle screw/rod fixation, decompression, and interbody cage placement. Used for PLIF, TLIF, posterolateral fusion, and cervical procedures.
- Grainger & Allison's Diagnostic Radiology, p. 1313
C. Combined / 360° Fusion
Anterior interbody fusion combined with posterior stabilization using pedicle screws, rods, and/or facet/intertransversal fixation. Highest reported fusion rates (~91%).
- Campbell's Operative Orthopaedics 15th Ed 2026, Table 46.3
2. Specific Fusion Techniques
Posterolateral Fusion (PLF)
The most traditional lumbar technique. Bone graft is placed lateral to the facets between the transverse processes. Can be done with or without pedicle screw instrumentation. Reported fusion rate ~85% (uninstrumented) to 89% (instrumented).
Interbody Fusion Techniques
All involve disc removal, endplate preparation, and insertion of an interbody cage (± bone graft) to restore disc height, achieve indirect neural decompression, and promote anterior column fusion. Fusion rate ~89% (posterior interbody) and ~86% (anterior interbody).
| Technique | Abbreviation | Approach | Key Notes |
|---|---|---|---|
| Anterior Lumbar Interbody Fusion | ALIF | Retroperitoneal/transperitoneal | Large cage footprint, good lordosis restoration; avoids posterior musculature |
| Posterior Lumbar Interbody Fusion | PLIF | Posterior midline | Bilateral cage placement via bilateral retraction of thecal sac |
| Transforaminal Lumbar Interbody Fusion | TLIF | Posterior, unilateral facetectomy | Unilateral neural retraction; lower nerve injury risk than PLIF |
| Minimally Invasive TLIF | MIS-TLIF | Posterior, percutaneous | Same corridor as TLIF with less muscle damage |
| Oblique Lumbar Interbody Fusion | OLIF / ATP | Oblique retroperitoneal (anterior to psoas) | L2-L5; avoids psoas and posterior structures |
| Lateral Lumbar Interbody Fusion | LLIF / XLIF | Lateral transpsoas | L2-L4 primarily; risk of lumbar plexus injury |
- Campbell's Operative Orthopaedics 15th Ed 2026, Figure 44.37
- Grainger & Allison's Diagnostic Radiology, p. 1313
Cervical Interbody Fusion
- ACDF: Standard approach - anterior discectomy followed by cage or cortical graft placement, typically with anterior plate fixation.
- Posterior Cervical Fusion: Used for multilevel stenosis, deformity, or when anterior approach is contraindicated. Lateral mass screws or pedicle screws with rod constructs are used.
3. Instrumentation
Rigid spinal fixation hardware holds the construct stable while biological fusion occurs. Instrumentation alone is NOT the fusion - it is temporary support until bony union is achieved.
- Pedicle screw and rod constructs: Gold standard for posterior lumbar/thoracic fixation. Provides three-column stability. Can be augmented with cement in osteoporotic bone.
- Translaminar / transfacet screws: Used as an adjunct or minimally invasive option.
- Anterior plates: Used in ACDF and corpectomy reconstructions.
- Hooks and wires: Older methods; still used in some scoliosis constructs.
Cement augmentation of pedicle screws (PMMA injected before or through cannulated screws) has Level II evidence supporting its use in osteoporotic vertebrae to reduce loosening and pseudarthrosis risk. A newer technique - Stent-Screw-Assisted Internal Fixation (SAIF) - uses balloon-expandable vertebral body stents with fenestrated pedicle screws for severe osteoporotic fractures.
- Rockwood and Green's Fractures in Adults 10th Ed 2025, p. 2296-2297
4. Bone Graft and Biologics
Fusion depends on biological bone formation. Graft options:
| Type | Examples | Role |
|---|---|---|
| Autograft | Iliac crest (ICBG), local bone, rib, fibula | Gold standard osteogenic material |
| Allograft | Femoral rings, fibular struts, bone chips | Structural support; lower osteogenicity |
| Synthetic substitutes | Hydroxyapatite, tricalcium phosphate, calcium sulfate | Osteoconductive scaffolds |
| Biologics | Recombinant BMP-2 (rhBMP-2), demineralized bone matrix (DBX) | Osteoinductive; BMP increases fusion rates but raises perioperative complication risk |
| Cage + graft | PEEK, titanium, carbon composite packed with graft | Load-bearing with central fusion |
Note: BMP use in spinal fusion has been associated with increased perioperative complications - a large study of 55,862 fusions found higher complication rates with BMP compared to autograft alone.
- Campbell's Operative Orthopaedics 15th Ed 2026
5. Fusion Rates by Method (Evidence-Based Summary)
From a critical meta-analysis (Campbell's Table 46.3):
| Variable | Fusion Rate |
|---|---|
| No instrumentation | 84% |
| Any instrumentation | 89% |
| Posterolateral fusion | 85% |
| Posterior interbody fusion | 89% |
| Anterior interbody fusion | 86% |
| Circumferential (360°) fusion | 91% |
| Autogenous bone alone | 87% |
| Autogenous bone + interbody cage | 90% |
6. Pseudarthrosis (Failed Fusion)
Reported in 9-30% of cases. Risk is not reliably reduced by bracing or extending the construct. Diagnosis requires correlation of persistent localized pain, progressive deformity, flexion-extension radiographs showing > 5° motion, and ultimately surgical exploration. 50% of pseudarthroses are asymptomatic; repair is indicated only for disabling pain.
- Campbell's Operative Orthopaedics 15th Ed 2026, pp. 277-284
7. Minimally Invasive Spinal Fusion
MIS approaches (percutaneous pedicle screws, tubular retractors, endoscopic fusion) aim to reduce blood loss, muscle damage, and hospital stay while achieving equivalent fusion. Pedicle screw stabilization remains the preferred instrumentation method even in MIS settings.
- Miller's Anesthesia 10th Ed, Common Spinal Procedures
Indications summary (from Gray's Anatomy for Students): Spinal fusion is indicated for post-fracture stabilization, tumor-related instability, and mechanical pain originating from the disc or posterior elements. Choice of approach (anterior, posterior, or combined) depends on the pathology level, patient factors, and surgeon preference.
Can you give some diagrams
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
I have a strong set of diagrams and radiological images from the textbooks. Here they all are, organized by fusion method:
Spinal Fusion - Diagrams & Images from Textbooks
1. Graft Materials & Radiological Appearances (ACDF, PLIF, TLIF)
Grainger & Allison's Diagnostic Radiology - Fig. 51.1
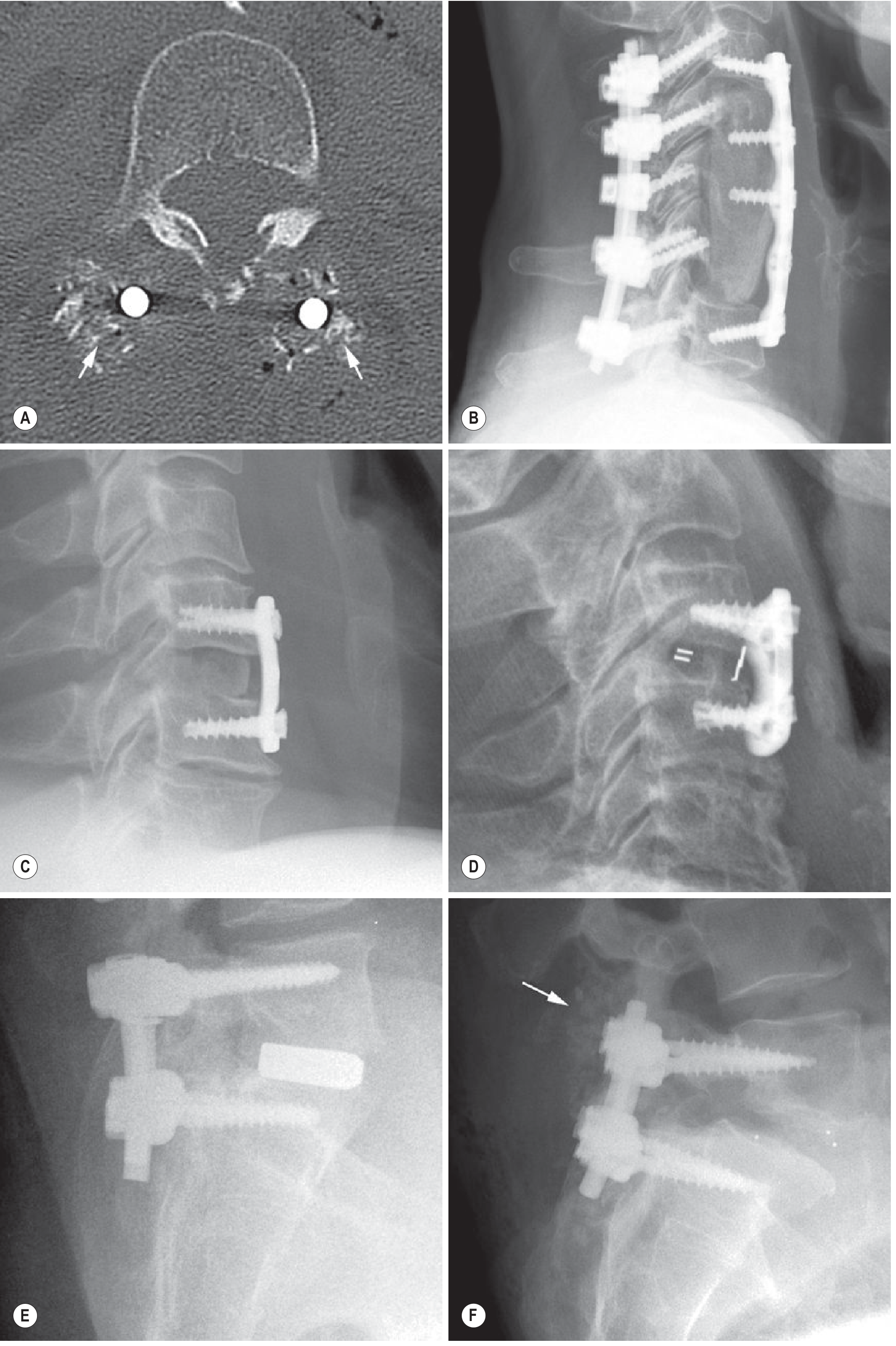
(A) Axial CT - morselised bone chips (arrows) in lumbar fixation. (B) Lateral X-ray - cervical corpectomy (C4-C6) with iliac crest autograft, anterior plate + posterior pedicle screw-rod construct (C3-C7). (C) Cortical autograft in ACDF. (D) Radiolucent PEEK cage in ACDF with radiopaque markers. (E) PLIF with radiopaque interbody cage in lumbar spine. (F) TLIF with radiolucent cage - only the cage markers are visible as dots; note bone chips posterior to hardware (arrow).
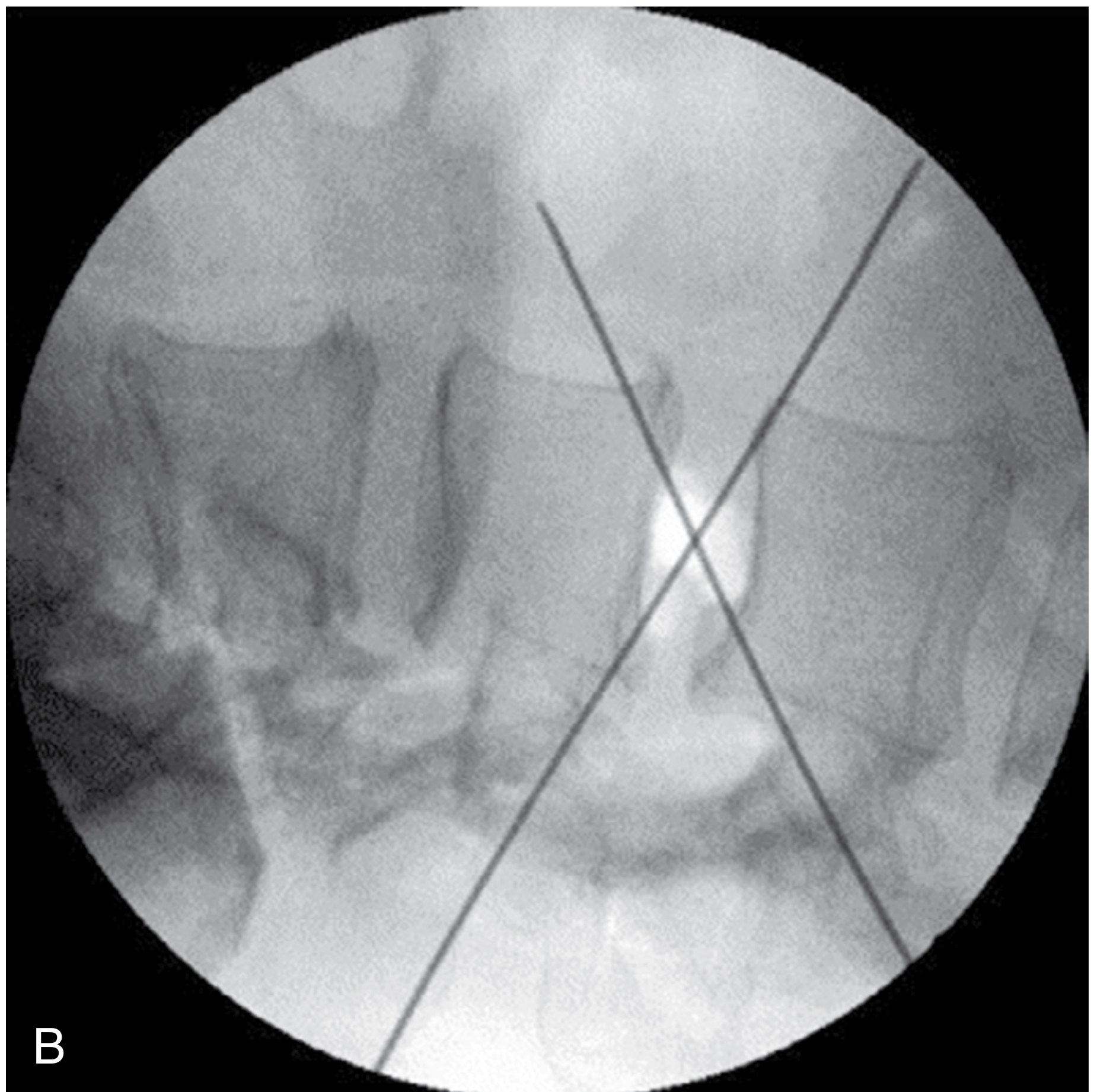
2. XLIF (Extreme Lateral Interbody Fusion) - Percutaneous Lateral Approach
Campbell's Operative Orthopaedics 15th Ed - Fig. 44.33 (fluoroscopy) & Fig. 44.34 (surgical illustration)
Fluoroscopic K-wire placement (lateral approach, L1-L4-5):
Step-by-step dilator insertion through psoas major to reach the disc:
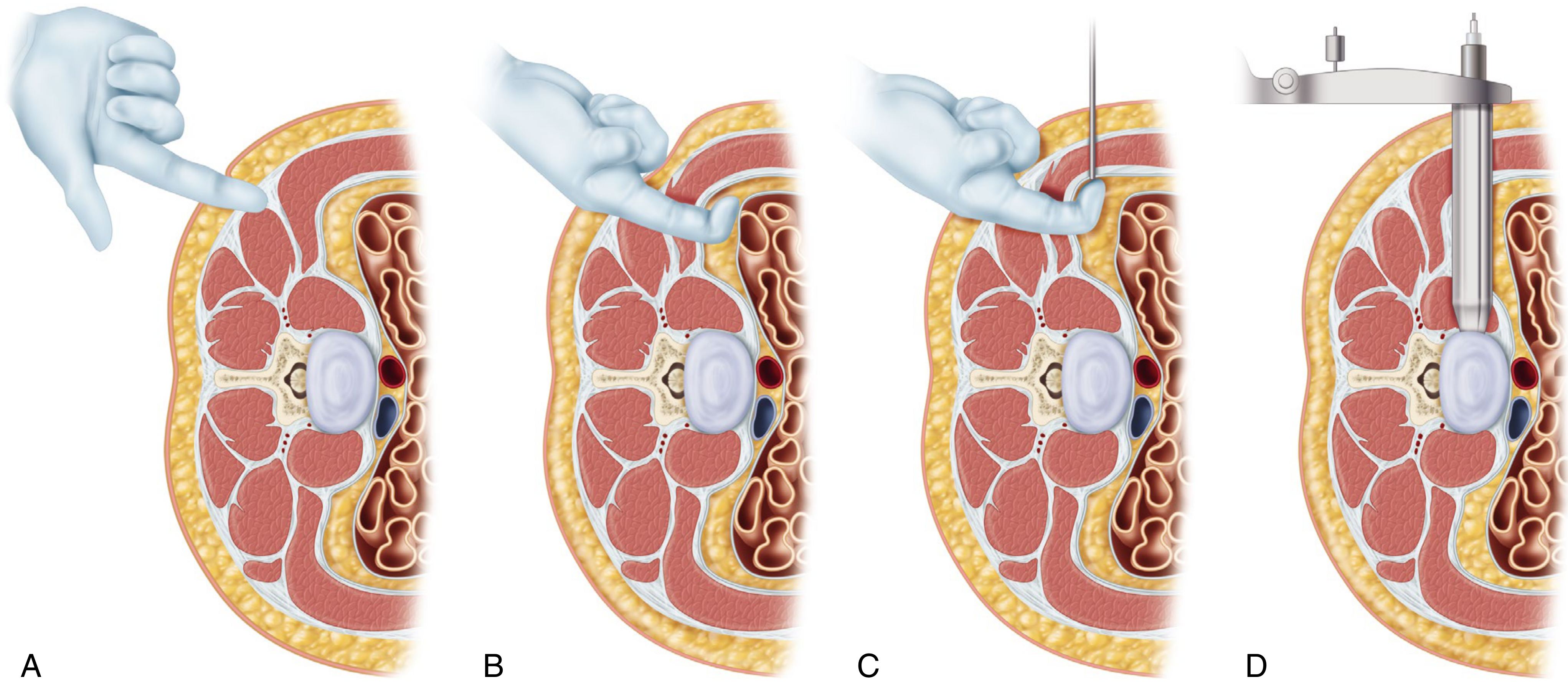
(A) Index finger identifying retroperitoneal space. (B) Retroperitoneal blunt dissection. (C) Initial dilator guided into position. (D) Final retractor through psoas major, seated directly on the lateral disc space.
3. OLIF (Oblique Lumbar Interbody Fusion) - Patient Positioning & Exposure
Campbell's Operative Orthopaedics 15th Ed - Fig. 44.38
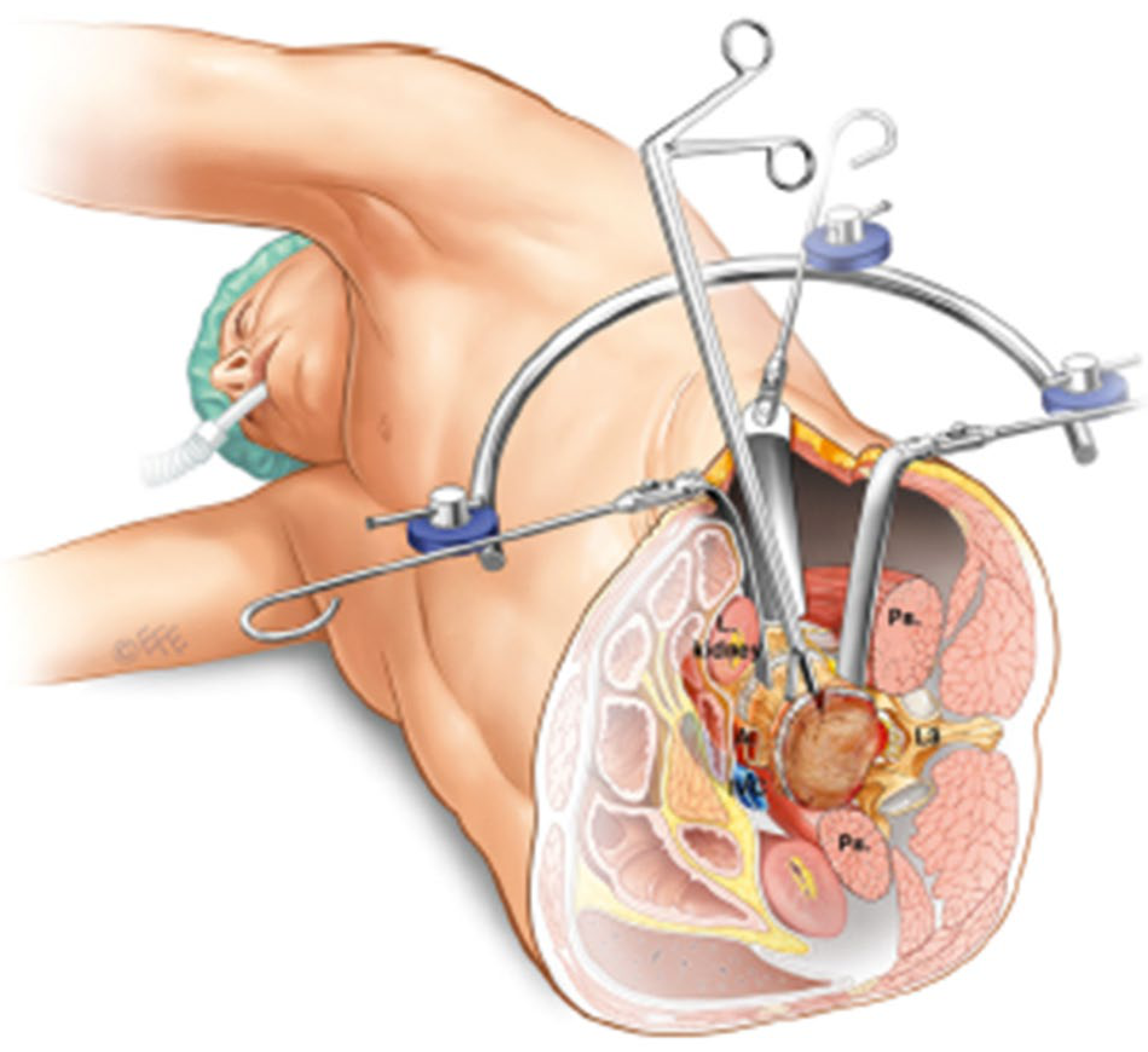
The OLIF corridor passes between the anterior vessels and the psoas muscle (labelled "Ps." on each side), avoiding both. The left kidney is visible superiorly. Langenbeck hooks and self-retaining retractors hold the retroperitoneal space open for disc access.
4. OLIF / Anterolateral Approach - Intraoperative Endoscopic View
Campbell's Operative Orthopaedics 15th Ed - Fig. 44.39
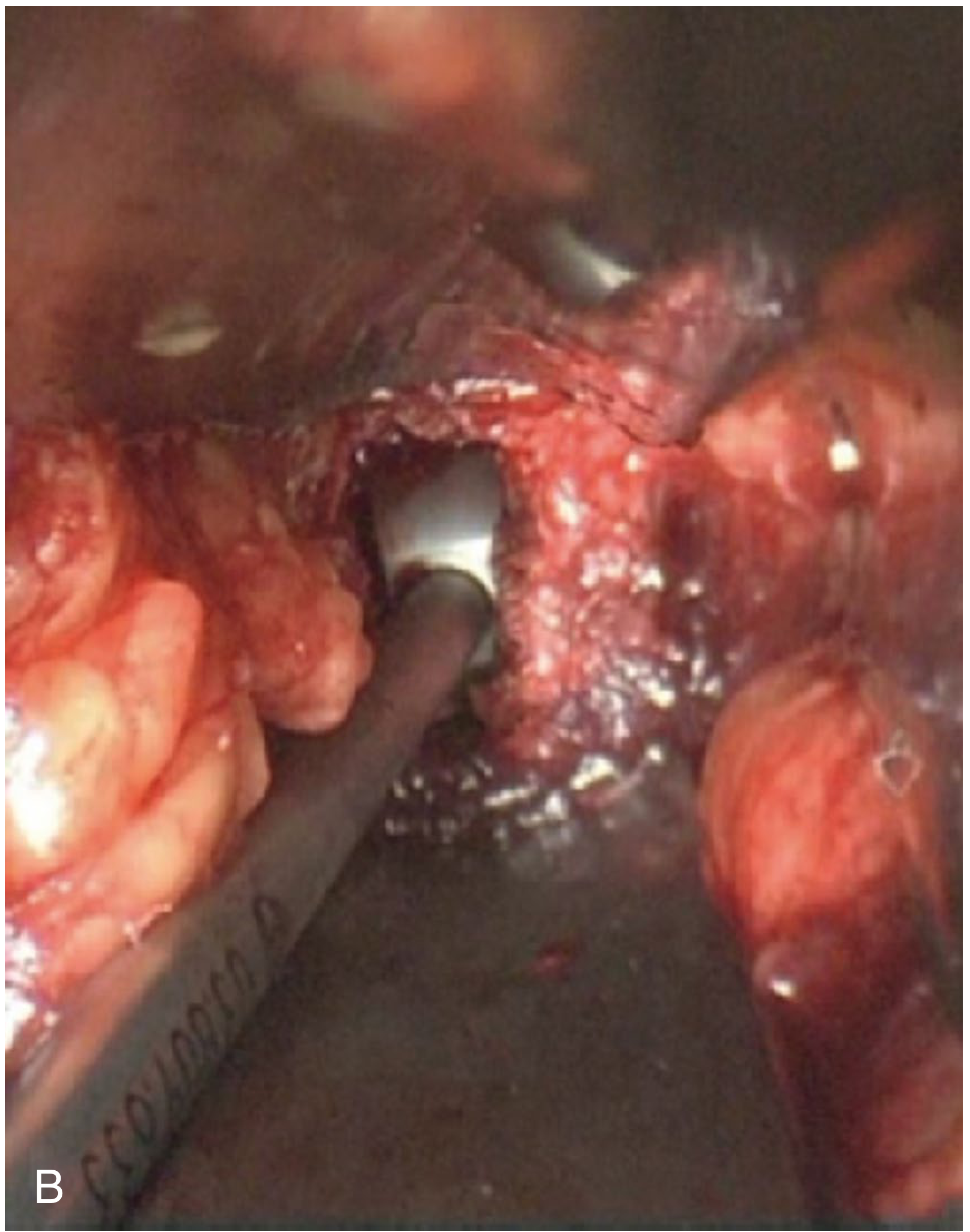
Endoscopic view of the oblique anterolateral approach with psoas muscle retracted, exposing the anterolateral surface of the disc space directly.
5. XLIF - Operative Photo of Lateral Dilators In-Situ
Campbell's Operative Orthopaedics 15th Ed - Fig. 44.35

Patient in lateral decubitus. The colored sequential dilators are shown penetrating psoas major and resting on the desired disc space. This MIS technique avoids the posterior musculature entirely.
Quick Reference - Approach Zones
The zones of approach for all lumbar interbody techniques are shown in Campbell's Fig. 44.37 (referenced in our previous answer). From anterior to posterior:
- ALIF - directly anterior, transperitoneal/retroperitoneal
- OLIF/ATP - oblique, between vessels and psoas
- LLIF/XLIF - directly lateral, trans-psoas
- TLIF - posterolateral, through the foramen
- PLIF - posterior midline, bilateral retraction of thecal sac
This is a shared conversation. Sign in to Orris to start your own chat.